
Abstract
Background:
An adductor canal block (ACB) and preoperative oral gabapentin have each been shown to decrease postoperative pain scores and opioid usage in patients undergoing anterior cruciate ligament (ACL) reconstruction.
Purpose/Hypothesis:
This study evaluated the efficacy of preoperative gabapentin on postoperative analgesia in patients who received an ACB. We hypothesized that patients undergoing ACL reconstruction with an ACB who utilized a single dose of preoperative oral gabapentin would have decreased pain and opioid consumption in the 24 to 72 hours after surgery compared with patients who did not utilize gabapentin.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between January and October 2016, patients at a single institution who underwent ACL reconstruction and received an ACB were identified. Patients who underwent surgery before May 2016 were placed in the control group, and patients seen after May 2016 received a preoperative dose of gabapentin and were placed in the gabapentin group. All patients completed a pain log via a smartphone application to record pain scores and opioid usage after surgery.
Results:
A total of 74 patients were identified: 41 in the gabapentin group and 33 in the control group. There were no significant differences between groups in demographics and operative characteristics. There were no differences in pain scores on postoperative day 1 (gabapentin vs control: 5.53 vs 5.56; P = .95), day 2 (4.58 vs 4.83; P = .59), or day 3 (4.15 vs 3.87; P = .59). The mean opioid consumption in oral morphine equivalents was not different on postoperative day 1 (gabapentin vs control: 47.2 vs 48.1; P = .90), day 2 (29.9 vs 33.5; P = .60), or day 3 (17.4 vs 18.7; P = .80).
Conclusion:
Preoperative gabapentin did not reduce pain scores or opioid usage in patients who received an ACB and underwent ACL reconstruction in this retrospective cohort study.
Keywords
In Western countries, about 40% of outpatients and up to 70% of hospitalized patients suffer from pain of moderate to severe intensity after surgery, with orthopaedic procedures identified as having the highest rate of pain complaints. 7 Anterior cruciate ligament (ACL) tears are one of the most common problems that lead to arthroscopic reconstruction, a procedure that is accompanied by moderate to severe postoperative pain. 1,19 Nearly all of these reconstructions are performed on an outpatient basis because of the significant reduction in cost compared with an overnight admission. To accomplish this safely and maintain a high degree of patient satisfaction, adequate postoperative control must be available. 3
In an effort to balance pain control with patient satisfaction, physicians are continuing to prescribe opioid medication at an alarming rate. From 1997 to 2005, there was a 588% increase in oxycodone prescriptions and a 198% increase in hydrocodone prescriptions, ultimately leading to a reported 79.5 million prescriptions in 2009 for all opioids. 2,14 While there is no gold standard for the management of postoperative pain after ACL reconstruction, physicians are now utilizing a multimodal approach to decrease the prescription and usage of opioid medications and alleviate some of these societal burdens. One of these modalities is a peripheral nerve block. The ideal nerve block would provide effective analgesia, minimize opioid use and side effects, and hasten mobilization by preserving motor strength. 4
Two of the most commonly used blocks in ACL reconstruction are the femoral nerve block and adductor canal block (ACB). The current literature has shown that both provide adequate pain control and minimize opioid consumption. 4,5,8,16 –18,20 There has been increased interest in the use of an ACB in lower extremity surgery as a motor-sparing sensory blockade. Studies in healthy volunteers have shown better short-term quadriceps strength and a decreased risk of falls. 3,4,10 –12 In addition to a peripheral nerve block, adjuvant oral medication such as gabapentin has been shown to decrease pain scores and opioid usage after arthroscopic ACL repair. 13 To our knowledge, no study has directly compared the use of an ACB with and without the addition of adjuvant oral gabapentin.
The purpose of this study was to evaluate the effect of preoperative gabapentin on a cohort of patients undergoing ACL reconstruction with the use of a concomitant ACB. We hypothesized that preoperative oral gabapentin would decrease pain and opioid consumption in the 24 to 72 hours after surgery.
Methods
This study was approved by the institutional review board of our institution. As the standard of care, all patients undergoing ACL reconstruction are invited to register to complete a pain management log for the first 72 postoperative hours via a secure smartphone application. All agreeing patients freely consented to the use of this application. Patient records were identified for all of those who underwent ACL reconstruction with a concomitant ACB between January and October 2016 and who agreed to complete the postoperative pain log. Patients who underwent surgery before May 2016 did not receive gabapentin and were placed in the control group. Patients who were seen after May 2016 received a 1-time dose of gabapentin 1 hour before surgery based on their weight as the standard of care and were placed in the gabapentin group. Patients weighing less than 54.4 kg received 300 mg, while those weighing over 54.4 kg received 600 mg of gabapentin. The single preoperative administration and dosage were determined after an extensive literature review demonstrated gabapentin’s efficacy in reducing postoperative pain in doses ranging from 300 to 1200 mg given before surgery. In addition, all patients in this study were gabapentin-naive, and it was our opinion that this regimen could minimize the dose-related sedative side effect of gabapentin. 6,7,13,14,16,19
All instances of the ACB were performed using 20 mL ropivacaine 0.5%, and all patients received general anesthesia with an inhalational anesthetic and a laryngeal mask airway after an intravenous induction dose of propofol (∼2-2.5 mg/kg).
Postoperatively, all patients were prescribed oxycodone/acetaminophen 7.5/325 mg to be taken as needed but not to exceed 1 tablet every 4 hours as well as naproxen 500 mg to be taken twice daily. All patients were placed in a soft dressing. They were instructed to be nonweightbearing until their first clinic visit. Additionally, they were instructed to work on quadriceps sets, heel slides, and straight-leg raises in the interim. All patients returned to the clinic by postoperative day 4, when the dressings were removed, weightbearing was advanced, and a formal rehabilitation protocol was prescribed.
Exclusion criteria for this study consisted of pregnancy/lactating, liver or renal dysfunction, known gabapentin or ropivacaine allergies, active infections, chronic pain and/or opioid use, known coagulopathies, and those receiving neuraxial anesthesia. The primary outcomes determined were mean pain scores (with 10 being worst pain) and opioid usage. Opioid data were converted with an equianalgesic chart to oral morphine equivalents. To ensure similarity between the 2 groups, demographic data (age, sex, height, weight) and operative characteristics (tourniquet time, graft selection) were compared.
Statistical analysis was performed using R (R Foundation for Statistical Computing, http://www.R-project.org) or JMP Pro 12 (SAS Institute). We utilized Student t tests for continuous data, such as for the primary outcome, and chi-square or Fisher exact tests for categorical data, as appropriate. Two-tailed P values <.05 were considered statistically significant.
Results
Overall, 74 patients met all inclusion criteria: 37 were male, and 37 were female. The gabapentin group consisted of 41 patients (23 male, 18 female), and the control group consisted of 33 patients (14 male, 19 female) (P = .242). The overall mean patient age was 27.3 years. The mean age in the gabapentin and control groups was 25.8 and 29.1 years, respectively (P = .203). The overall mean height and weight were 174.38 cm and 74.91 kg; when broken down by study group, the mean height and weight were 174.83 cm and 76.39 kg for the gabapentin group and 173.84 cm and 73.07 kg for the control group (P = .653 and .382, respectively). The overall mean tourniquet time was 80.84 minutes; 79.58 minutes for the gabapentin group and 82.29 minutes for the control group (P = .624). This information can be seen in Table 1. The graft selection broken down by treatment group (P = .901) can be seen in Table 2.
Demographics and Operative Characteristics a
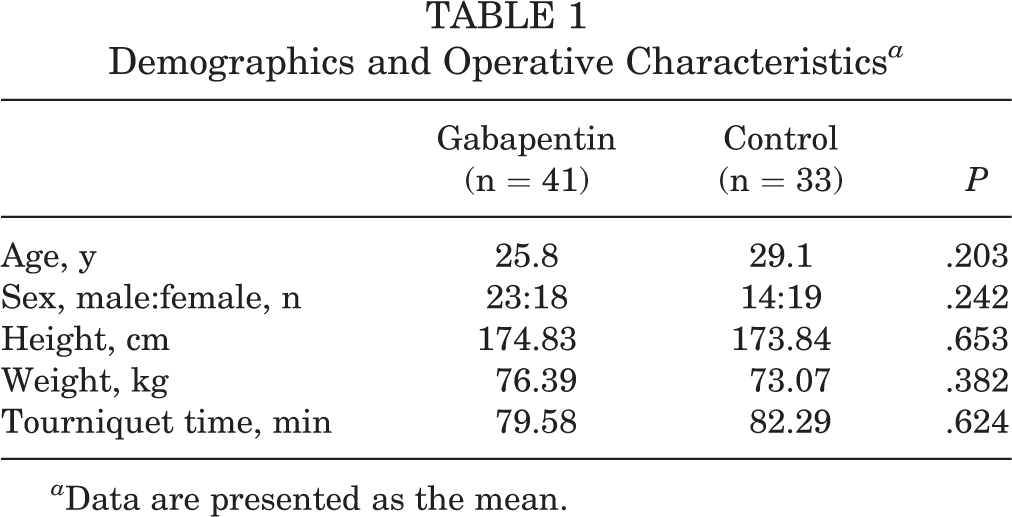
a Data are presented as the mean.
Type of Graft Utilized a
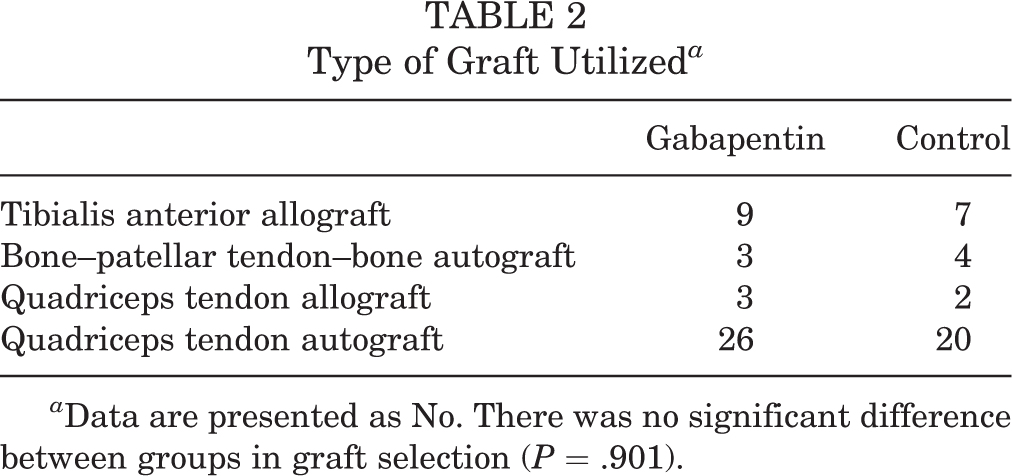
a Data are presented as No. There was no significant difference between groups in graft selection (P = .901).
Tables 3 and 4 outline the mean pain score and opioid consumption (in morphine equivalents) based on treatment group over time, and this is plotted in Figures 1 and 2. Although mean pain scores decreased over time for both groups, they were not statistically significant between groups on postoperative day 1 (gabapentin vs control: 5.53 vs 5.56; P = .95), postoperative day 2 (4.58 vs 4.83; P = .59), or postoperative day 3 (4.15 vs 3.87; P = .59). The mean opioid consumption reported in oral morphine equivalents also decreased over time for both groups and was not significantly different between groups on postoperative day 1 (gabapentin vs control: 47.2 vs 48.1; P = .90), postoperative day 2 (29.9 vs 33.5; P = .60), or postoperative day 3 (17.4 vs 18.7; P = .80).
Pain Scores a
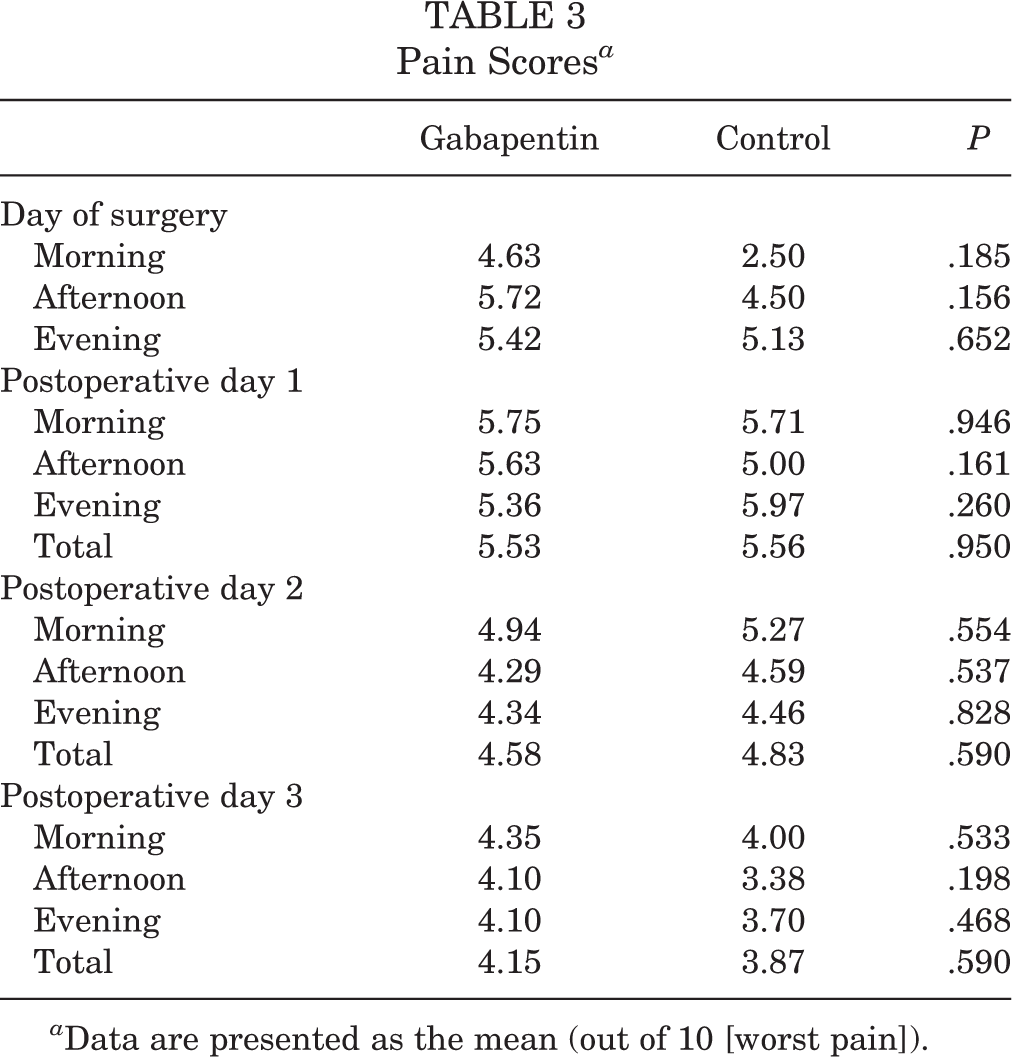
a Data are presented as the mean (out of 10 [worst pain]).
Opioid Consumption in Oral Morphine Equivalents a

a Data are presented as the mean.
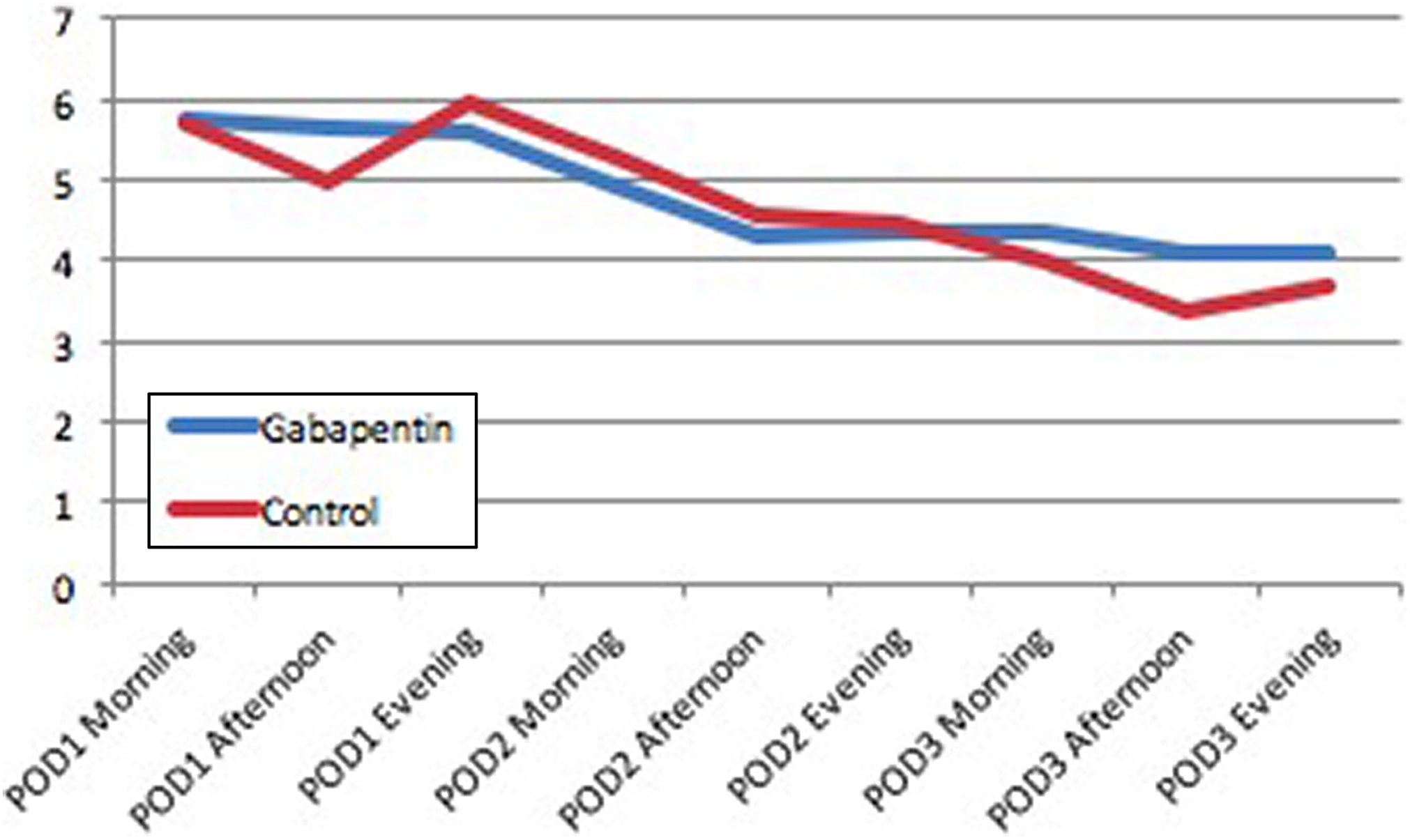
Pain scores (out of 10 [worst pain]) over time in the gabapentin and control groups. POD, postoperative day.
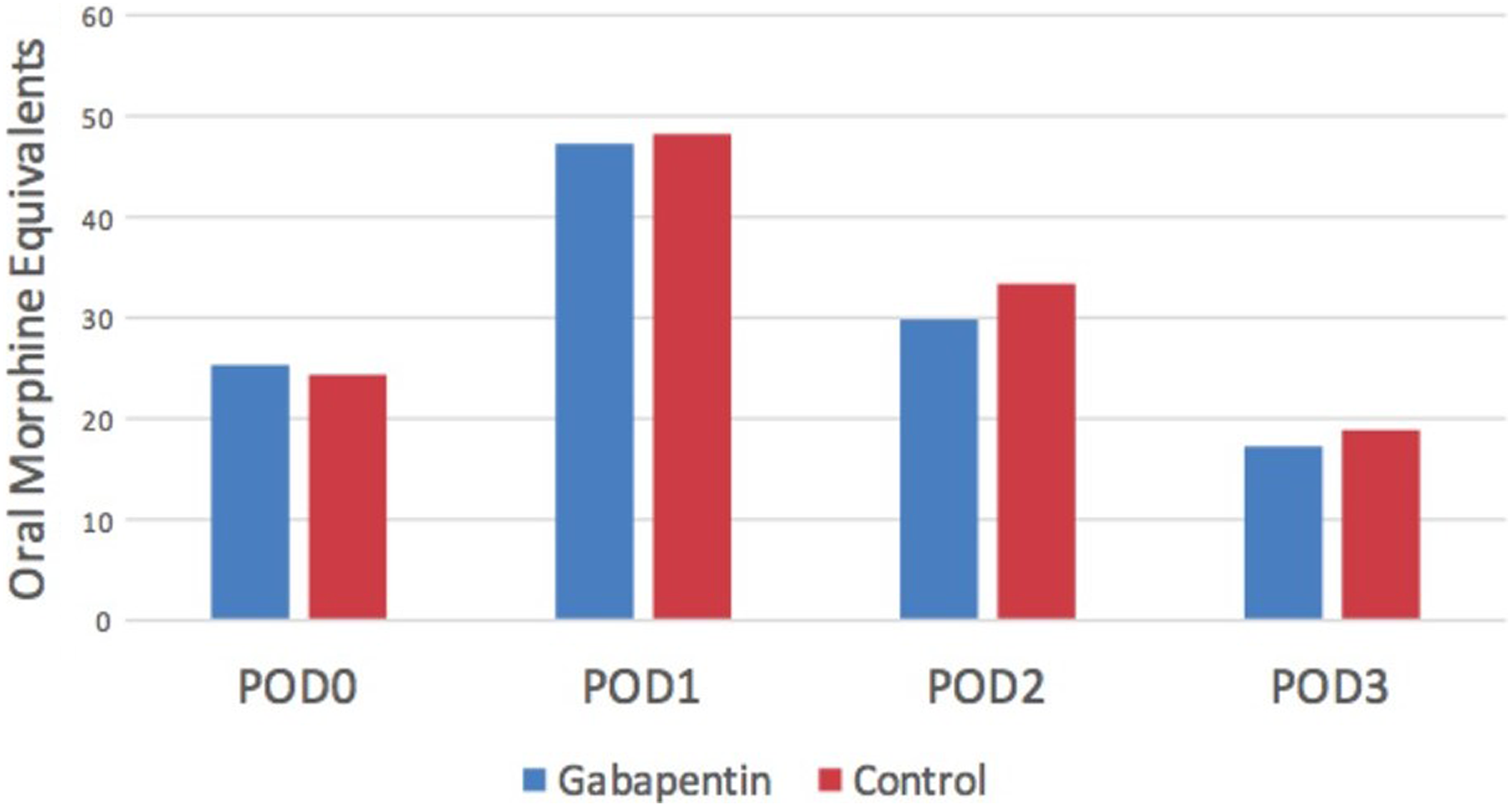
Opioid consumption by postoperative day (POD) in the gabapentin and control groups.
Discussion
At present, there is no consensus regarding the optimal management of pain after ACL reconstruction. Multimodal pain regimens have been utilized with increasing frequency in an effort to minimize pain and opioid consumption and maximize recovery. This study was designed to evaluate the efficacy of a single dose of preoperative gabapentin in addition to an ACB as part of a multimodal pain regimen after ACL reconstruction.
We found that gabapentin did not further improve postoperative analgesia with respect to pain scores or opioid usage in the setting of an ACB. Tables 3 and 4 show that pain scores and opioid usage were similar between treatment groups at all time points postoperatively. This finding is contrary to numerous well-designed studies that have demonstrated that gabapentin is efficacious in reducing postoperative pain and opioid use. 6,7,13,14,16,19 However, the data among these studies are inhomogeneous, and it is difficult to draw direct comparisons from across the board. Additionally, none of these studies have directly compared the efficacy of gabapentin in the setting of an ACB.
One explanation for the difference between the findings of the current study and previous research could be the similar site of action of gabapentin and the ropivacaine used in the ACB. Gabapentin is thought to act by binding to voltage-dependent Ca2+ channels on the presynaptic neuron that are upregulated after a peripheral nerve injury, leading to inhibition of the afferent pain response. 6 Ropivacaine also prevents afferent pain transmission by acting on the presynaptic neuron; however, its mechanism of action relies on inhibition of presynaptic sodium ion influx. 9 Mardani-Kivi et al 13 showed that administering a single preoperative dose of 600 mg gabapentin without the use of a peripheral nerve block in patients undergoing ACL reconstruction decreased both pain intensity and opioid consumption, which was consistent with the findings of Menigaux et al. 14 Therefore, it is possible that the concomitant use of gabapentin with ropivacaine leads to a redundant rather than synergistic effect on postoperative analgesia.
A second potential explanation for our results could be a dose-related response in the setting of a peripheral nerve block. In our study, 300 versus 600 mg of gabapentin was administered, based on the patient’s weight being below or above 54.4 kg, respectively. Researchers have identified that 600 mg administered before surgery provides the best balance between pain relief and unwanted effects such as sedation. 15 Therefore, this was chosen to be the maximum dose administered in our study, given that all of the enrolled patients were gabapentin-naive. It is possible that this dosage is below the threshold necessary to show improvement in the setting of an ACB.
Numerous prior studies have effectively shown a benefit in the role of gabapentin to reduce postoperative pain and opioid use; however, dosing, medication scheduling, and methods of peripheral and general anesthesia all varied. 6,7,13,14,16,19 In these studies, dosages ranged from 300 to 1200 mg, with the majority being a single preoperative dose. Ho et al 6 performed a meta-analysis of 16 randomized controlled trials studying the efficacy of gabapentin in postoperative pain control. They subdivided the trials into dosing regimens of less than 1200 mg, 1200 mg, and multidosing schedules. They concluded that the treatment regimens of less than 1200 mg or exactly 1200 mg were effective in minimizing postoperative pain levels and opioid requirements within 24 hours; however, most studies required a preoperative dose of 1200 mg to be effective. The multidosing regimens showed no additional benefits within the first 24 hours.
This study has several strengths. It is the first to evaluate the effect of adjuvant gabapentin in the setting of a peripheral nerve block. Additionally, this study utilized a novel pain log smartphone application that allowed patients to document numerous parameters including, but not limited to, postoperative pain scores and medication consumption. This allows for the collection of more accurate data for longer time periods. As such, we were able to collect real-time data up to 72 hours postoperatively compared with other similar studies, which were limited to a smaller time frame, or retroactive surveys in the clinic setting.
This study has several limitations as well. With an enrollment of 74 patients, it is possible that this study is underpowered, despite calculations from our power analysis and it being of a size comparable to similar studies in the literature. Additionally, it is inherently limited by its retrospective nature, yielding level 3 evidence. Last, as mentioned previously, it is possible that our dosing and medication schedule may have limited the ability to detect a difference in pain, especially in the setting of an ACB. Future studies are needed to determine the ideal dosage and schedule of gabapentin in relation to peripheral and central anesthesia methodology.
Conclusion
Physicians are continuing to prescribe opioid pain medications at an alarming rate. Multimodal pain regimens are being utilized by many surgeons today to improve patient pain and satisfaction while decreasing opioid burden and its detrimental effects. This study contributes to the current literature in that it refutes a synergistic effect on postoperative pain and narcotic consumption when adjuvant gabapentin is combined with an ACB after ACL reconstruction. While there is no current gold standard with regard to the optimal postoperative pain regimen after ACL reconstruction, it is important for treating surgeons to be familiar with the current literature to provide patients with the best outcome.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K. has received educational support from Arthrex and Smith & Nephew and has received consulting and speaking fees from Smith & Nephew. J.X. has received educational support from Arthrex, Linvatec, and VisionScope Technologies; has received consulting fees from Arthrex, Linvatec, and Trice Medical; has received speaking fees from Arthrex; and receives royalties from Arthrex. AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Emory University Institutional Review Board (IRB00093879).