Abstract
Background:
Contributing factors for arm injuries among baseball players have been described. However, no review has systematically identified risk factors with findings from prospective cohort studies.
Purpose:
To systematically review prospective cohort studies that investigated risk factors for arm injury among baseball players.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
Electronic databases were searched for relevant English-language studies. Titles, abstracts, and full-text articles were screened by 2 blinded reviewers to identify only prospective cohort studies and randomized controlled trials. Two independent investigators screened each article for appropriate criteria.
Results:
Fourteen prospective articles were selected for this review. Youth, high school, and professional baseball players (N = 2426) were pooled, and 43 risk factors were assessed in relation to general arm, shoulder, and elbow injuries. All studies evaluated players for at least 1 season. Deficits in preseason shoulder range of motion and strength were significant risk factors for general arm or shoulder injury among high school and professional players. Elbow and shoulder varus torque at peak external shoulder rotation during pitching, high pitch velocity, and shoulder rotational and flexion deficits were risk factors for elbow injuries among professional pitchers. Pitching >100 innings in 1 year, being aged 9 to 11 years, being a pitcher or catcher, training >16 hours per week, and having a history of elbow pain were significant risk factors for elbow injury among youth players.
Conclusion:
History of elbow pain and age had a high risk of associated elbow injury among youth players. Training or pitching load also increased elbow injury risk for youth athletes. Loss of shoulder range of motion appears to increase risk for elbow injury among professional athletes. Single time-point data collections per season, studies with the same sample population, and studies with self-reported injury and risk factor data may limit the interpretation of these findings. Health care professionals should use caution when assessing injury risk during evaluation and making decisions about the training workload and playing time of baseball players.
Arm injuries among baseball pitchers are highly prevalent at all levels of the sport. In Major League Baseball (MLB), an estimated half-billion dollars is lost annually as a result of professional pitchers being placed on the disabled list (DL). 12 Furthermore, these injuries account for nearly 50% of all injuries in MLB and equate to approximately 460,432 days on the MLB DL, with numbers continuing to rise. 12 While the risk of injury increases with age and level of competition, 32 arm injuries among youth and collegiate pitchers are alarmingly common. 16 Twenty-five percent of all arm injuries in collegiate baseball are categorized as severe (≥10 days of time loss from participation), 16 with a 4-fold increase in surgical intervention seen over the past decade. 21 The mechanisms that underlie these injuries are not well understood; however, it is generally accepted that upper extremity injuries in baseball pitchers are a result of repeated microtrauma to the musculoskeletal structures due to high-velocity repetitive loading. 10
Previous reviews about risk factors for baseball-related injuries have been descriptive or narrative reviews. 10,22,41 In these reviews, pitch type, player fatigue, faulty mechanics, and physical attributes were described as risk factors for injury. However, the studies that were cited to support these claims utilized cross-sectional studies 1,2,9,15,17,19,20,26,36 or case reports. 44,46 While these study designs can offer insight into associations of injury risk, they cannot infer a causal relationship, which is critical in understanding injury etiology and making general recommendations for safe play. To our knowledge, there does not exist a systematic account of factors that are causally linked through prospective observation. Therefore, the purpose of this study was to systematically review only prospective cohort studies investigating risk factors for upper extremity injuries of baseball players.
Methods
Information Sources
Four databases (PubMed, Web of Science, SPORTDiscus, and PEDro) were searched to identify studies that included data on risk factors for baseball-related injuries. Language was restricted to English, but date of publication was not restricted. Full details for the electronic search are available in Appendix Table A1.
Study Selection
Two reviewers (C.E.A., K.K.) screened eligible studies in 2 steps. In step 1, investigators evaluated titles and abstracts for prespecified inclusion and exclusion criteria. Inclusion criteria included the following: studies on baseball players, studies of upper extremity injuries, articles written in English, articles available in full text, and original research (prospective cohort studies and randomized controlled trials). We included only prospective cohort studies because they are the preferred design to provide direct and accurate estimates of incidence and risk. 5 Studies on athletes from all levels of play (ie, youth to professional) were included; as this was the first review to investigate risk factors causally related to injury, we felt it critical to include all skill levels. Furthermore, examination of risk factors across a broad range of athletes could provide insight on factors that lead to arm injury regardless of age or skill level. Exclusion criteria included the following: studies that did not include upper extremity injuries or that focused on traumatic injury (eg, eye injury, face injury); original study designs that were cross-sectional, case-control, case series, case reports, review articles, or articles describing injury medical management; studies that did not include baseball players; studies that analyzed the effectiveness of an intervention or surgical procedure; and studies that analyzed injured or postsurgical athletes only. Moreover, we excluded studies that assessed only pain rather than injury, where injury was considered some amount of time loss from play. All abstracts were evaluated independently by 2 reviewers and were either included or excluded. In step 2, the 2 reviewers independently read all full-text articles included in step 1 and evaluated for selection criteria. In cases of disagreement between them, a third reviewer (M.T.F.) made the final decision of article selection.
Data Collection
Data extracted from selected articles included the following: author and year of publication, study design, sample size, description of the study population, player position, specific type of injury and description, reported risk factor, and statistical measurement of injury risk (Table 1). Statistical measures were reported as expressed by the original authors: hazard ratio (HR), odds ratio (OR), relative risk (RR), and relative injury rate (RIR). A risk factor was considered when HR, OR, RR, or RIR was >1.0, and a protective factor was considered when HR, OR, RR, or RIR was <1.0.
Characteristics of 14 Prospective Studies Included in Systematic Review a

a DL, disabled list; MLB, Major League Baseball; SLAP, superior labrum anterior and posterior; UCL, ulnar collateral ligament.
Risk-of-Bias Assessment
Risk of bias was assessed with a modified version of the Newcastle-Ottawa Scale. 40 The scale was adapted for use among baseball players, modeled after the adaptations from Saragiotto et al 35 for their review on running-related injuries. The Newcastle-Ottawa Scale is a quality assessment tool in which a star rating system is used to indicate the quality of a study, with a maximum of 12 stars. 25 Criteria in this study to assess risk of bias were as follows: adequate description of baseball player type (eg, position, age, skill level), definition or description of baseball-related injury, representativeness of the exposed cohort, selection of the nonexposed cohort, ascertainment of exposure, demonstration that outcome of interest was not present at start of study, comparability of cohorts on the basis of the design or analysis, assessment of outcome, whether follow-up was long enough for outcomes to occur, adequacy of follow-up, and statistical measurement of the association of risk factors (eg, HR, OR, RR). The articles could be awarded a maximum of 1 star for each of the 11 items, except for item 7, which could be awarded 2 stars. Risk-of-bias assessment criteria for each study is available in Appendix Table A2.
Results
A total of 3224 studies were found as a result of our search criteria. Of those, 60 were duplicates, appearing in >1 database, and thus removed. After full-text articles were screened for selection criteria, only 12 prospective cohort articles § remained. Two studies classified as case-control 31,39 were included, as the methods were in alignment with a prospective cohort study. Thus, a total of 14 articles were included in this systematic review. Figure 1 depicts the complete article selection process.
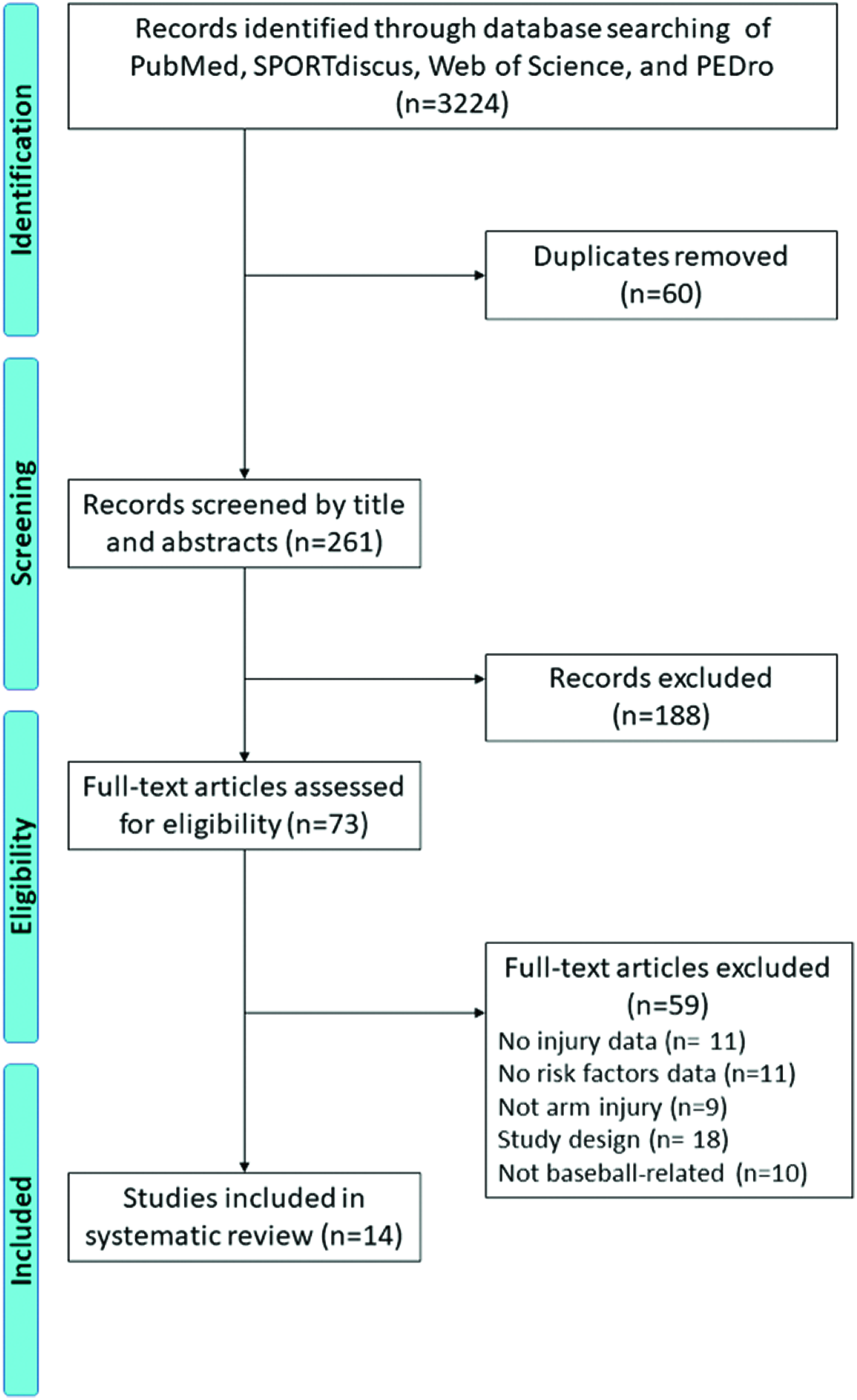
CONSORT (Consolidated Standards of Reporting Trials) diagram of selection process for systematic review articles.
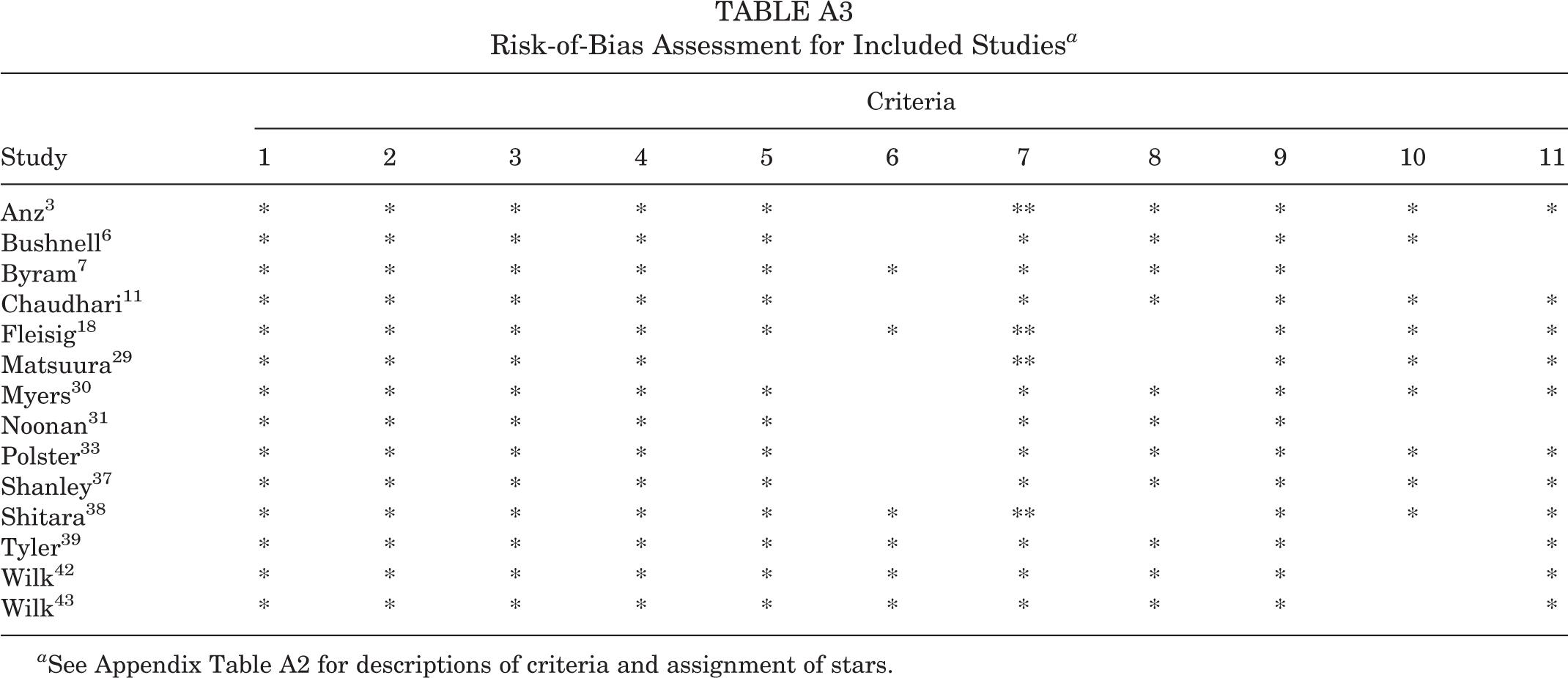
With respect to risk-of-bias assessment, the criteria with the most frequently awarded stars across studies were the description of the baseball player (14 of 14), the definition of musculoskeletal injury (14 of 14), the representativeness of the exposed cohort (14 of 14), and the selection of the nonexposed cohort (14 of 14). Criteria with the fewest stars awarded included demonstration that the outcome of interest was not present in the study (6 of 14) and adequacy of follow-up of cohorts (9 of 14) (Appendix Table A3). The mean number of stars awarded was 9.75 (range, 8-10).
Complete prospective analysis was conducted on a total of 559 professional baseball players, 521 high school athletes, and 1346 youth athletes (age range, 9-14 years). Studies utilized different injury definitions for risk analysis. All but 1 study 11 conducted on professional baseball players considered injury as placement on the official MLB DL. 3,6,7,42,43 Instead of DL placement, Chaudhari et al 11 defined injury in terms of time loss, in which a participant was unable to complete his scheduled work because of a musculoskeletal injury suffered during a baseball-related activity—whether that schedule included a desired number of pitches in practice, bullpen activity, or competition. The remaining studies differed in their injury definition by time loss. Five studies considered at least 1 day or missed event an injury 7,11,29,30,39 ; others used 8 or 10 days 33,38 or surgery and/or retirement 18 to define an injury.
Thirty-nine risk factors falling into 3 broad categories were studied: physical strength or structure, age, and throwing quantification or characteristics (Appendix Table A4). The majority of studies ∥ (10 of 14) assessed structural or strength deficits in relation to injury, with an emphasis on shoulder function. The remaining studies assessed throwing characteristics, such as pitch velocity 6 or pitch type and volume, 18 or player characteristics such as age, position, and baseball experience. 29 Only 1 study 3 assessed throwing mechanics in relation to injury risk.
One study 29 indicated that risk of shoulder injury for youth athletes (aged 7-11 years) increased for pitchers and catchers and for those athletes who trained 16 to 36 hours per week or had a history of shoulder or elbow pain. Two studies 38,39 examined shoulder risk factors among high school athletes and had conflicting results. Shitara et al 38 found that reduced glenohumeral internal range of motion at 90° of shoulder abduction increased shoulder injury risk, while Tyler et al 39 found no increase in shoulder or elbow injury risk for pitchers with excessive loss of internal range of motion or total shoulder range of motion loss. Likewise, Tyler et al 39 found that only supraspinatus weakness measured in the preseason was significantly associated with a major injury (>3 missed games), while Shitara et al 38 found that a greater difference in prone external rotation strength between arms was associated with shoulder injury risk among high school baseball players. For professional players, Byram et al 7 found deficits in preseason supraspinatus and prone external rotation strength to be risk factors for shoulder injury. In contrast, Wilk et al 44 found that reduced external rotation range of motion in the throwing arm was a risk factor for shoulder injury in professional players.
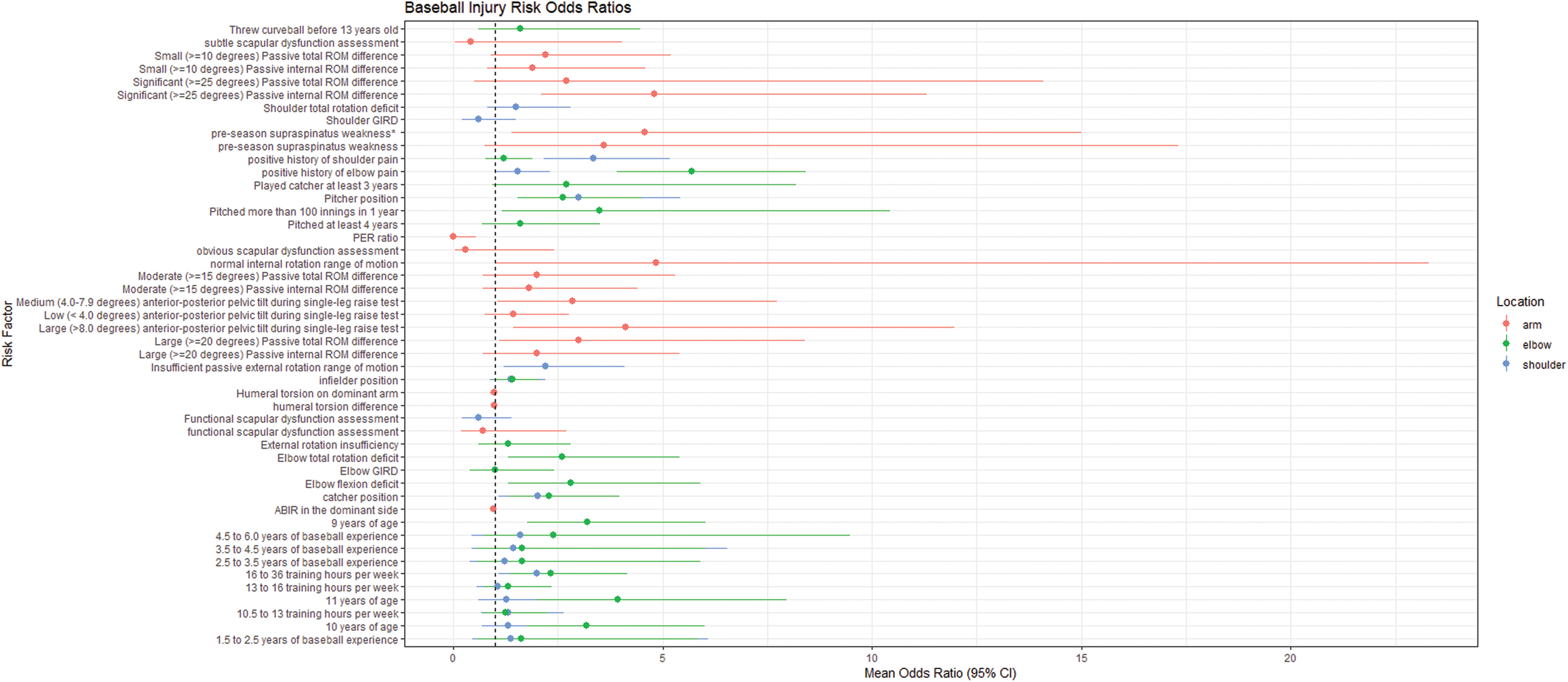
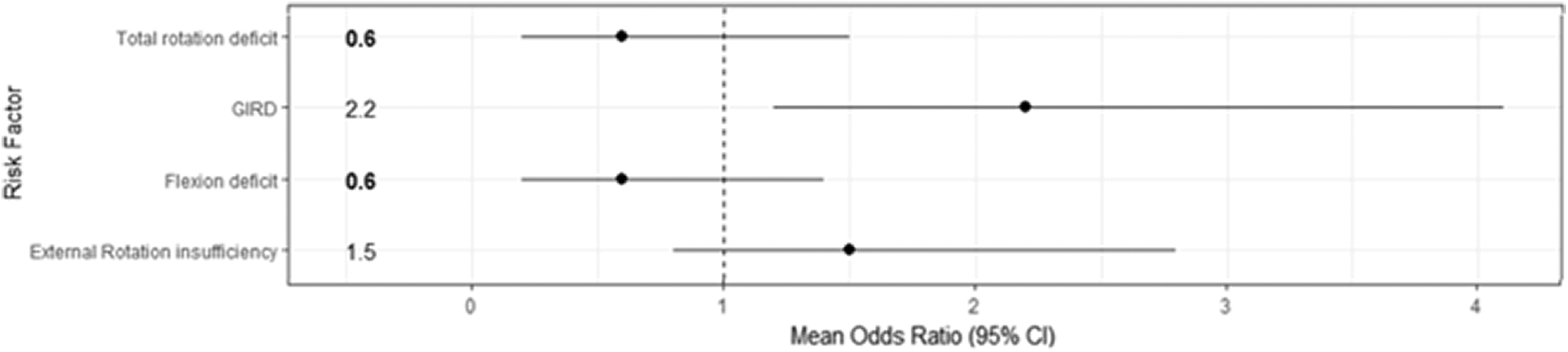
With respect to elbow injuries, 1 study 29 found that increased risk of elbow injuries for youth athletes (aged 7-11 years) was significantly associated with age, player position (pitcher or catcher), training 16 to 36 hours per week, and history of elbow pain. Another study 18 found that pitching >100 innings in a year was significantly associated with elbow injury among youth players (aged 9-14 years). Shitara et al 38 found that the difference in prone external rotation strength between arms was associated with elbow injury risk for high school baseball players. For professional players, increased risk of elbow injury was significantly associated with higher peak shoulder external rotation torque and elbow varus at maximum external rotation of pitching motion, 3 faster pitching velocity, 6 and reduced total shoulder rotation deficit and flexion deficit. 42 Figures 2, 3, and Appendix Figure A1 give odds ratios and 95% CIs for each risk factor for arm, shoulder, and elbow injury from each study, respectively.

Odds ratio and 95% CI for risk factors related to elbow injury. Bold numbers indicate significant association (P < .05). Dashed vertical line represents “no effect.” GIRD, glenohumeral internal rotation deficit.
Odds ratio and 95% CI for risk factors related to shoulder injury. Bold numbers indicate significant association (P < .05). Dashed vertical line represents “no effect.” GIRD, glenohumeral internal rotation deficit.
Discussion
Arm injuries among baseball players continue to rise. For the professional athlete, these injuries can have personal and financial implications. For youth athletes, injuries can have long-term consequences, as previous injury is a strong predictor of subsequent injury for several conditions and populations. 5 Strong evidence from prospective studies is needed to fully appreciate injury risk factors in baseball and help develop prevention programs. To our knowledge, this is the first review to systematically assess risk factors examined via prospective studies related to arm injuries in baseball.
Risk factors for shoulder injury were related to reduced preseason strength 38,39 and range of motion 7,44 among mature athletes (high school and professional) and player position, training time, and history of previous arm pain for youth athletes. 29 Likewise, risk factors for elbow injury differed among skill levels. Elbow varus and shoulder external rotation torque during maximal external rotation during pitching, 3 passive shoulder rotational and flexion range of motion deficits, 42 and high pitch velocity 6 were risk factors for elbow injury among professional baseball players. For youth players, pitching >100 innings in 1 year, 18 age 9 to 11 years, being a pitcher or catcher, and training >16 hours per week 29 were significant risk factors for elbow injury (Figure 2). However, these findings should be interpreted cautiously.
Importantly, there is only 1 risk factor—preseason prone internal rotation range of motion—that was examined prospectively in the same manner on the same type of athlete (ie, high school pitchers) by more than 1 study (see Appendix Table A4). 38,39 Two studies 7,39 examined the same risk factor—preseason supraspinatus and prone external rotation strength—in the same manner but in different types of pitchers. The other studies involving range of motion measures 42,44 reported injury risk related to differences between arms only, rather than on the throwing arm, making comparison difficult. While it is likely that some risk factors may differ among ages or skill level, a thorough investigation of the same potential risk factors may facilitate better general recommendations to reduce arm injury at all levels of play. Likewise, a better understanding of the influence of risk factors across age and skill can help to deduce potential mechanisms of injury specific to each population.
Additionally, the methodological choices of prospective studies should be considered when evaluating the findings. Matsuura et al 29 captured injury data using self-report via a questionnaire. Furthermore, the study utilized self-reported pitching and player characteristics collected from a coach- or parent-completed questionnaire filled out the previous year to determine risk of injury. This data collection method has the potential for recall bias and human error. Likewise, Fleisig et al 18 utilized self-reported injury and risk factor data in the form of postseason questionnaires to determine risk of association. Peak elbow and varus torque were identified as risk factors for elbow injury among professional baseball players, 3 however only 1 pitching cycle was utilized for analysis: fastest pitch that was a strike, which was thrown in a controlled laboratory setting. Given that variability in movement patterns exist, particularly for experts, 4,14,24 variables calculated from 1 pitch thrown may not accurately represent the athlete’s native or habitual mechanics. Likewise, only the maximum pitch velocity was utilized for risk association measurement. Again, this velocity illustrates an athlete’s capacity, rather than his habitual velocities, across a bullpen session, game, or season and may not truly represent contributing factors to overuse or overloading of musculoskeletal tissues.
Many studies examined pitching mechanics in relation to joint loading 1,2,15,26,34 and fatigue. 13,17 Often, changes in loading and fatigue, even a decline in pitch velocity, 8 are used to infer injury risk from cross-sectional or retrospective data. The danger in this method is that correlations can be misrepresented as causal links and potential latent contributing factors for injury can go unexplored. To date, no prospective studies exist linking specific mechanical patterns to injury incidence. Longitudinal tests are necessary to determine what mechanics, if any, are critical to train and monitor in order to reduce injury rates.
Some limitations exist for this review. We limited our search to English-language articles and those that were available to reviewers in full text. It is possible that additional prospective studies exist on risk factors related to upper extremity injuries among baseball players. The small number of studies and repeated sample populations from these articles weaken the findings from this review. In addition, we acknowledge that ages and skill ranges may have different risk factors for injury. All studies included only a single time point for data collection, typically during preseason assessment. Since shoulder range of motion measurements are known to change over a season, 23 a single time-point data collection method may not accurately reflect risk association. Furthermore, for most studies, there was just a single article that provided data on the risk factor; therefore, a true meta-analysis was not possible. Moreover, 4 studies 3,6,42,43 used the same sample of participants to examine and report on risk factors for shoulder and/or elbow injury concomitantly.
Finally, while all injuries had a time-loss component, the length and severity of injury were not comparable across studies. The definition of injury ranged from any time loss in play to forced retirement because of injury. Thus, the interpretation of injury for each study must be considered when assessing the associated risk factor. Additionally, we constrained our injury definition inclusion criteria to include some measure of time loss. While large prospective studies 27 found pitch type and pitch count to be significant predictors of pain, we do not believe that pain is synonymous with time-loss injury, as many athletes play with pain and many do so without significant loss of participation or performance. However, findings from these studies can be used to construct longitudinal studies and help to determine the relevance of each to injury development.
This review has significant clinical implications. For instance, of the 12 risk factors listed on the USA Baseball and MLB Pitch Smart initiative, 28 only 1 (ie, throwing too many innings over the course of the year) 18 has causal evidentiary support for injury, and only for youth athletes (Table 2). Moreover, the method to derive the measurement of risk was done so with subjective data and has a wide confidence interval (OR, 3.5; 95% CI, 1.16-10.44), thus limiting the confidence in the strength of the association. Consequently, more research is needed to appropriately design effective and efficient injury prevention programs across all levels of play. Additional research should focus on (1) objectively and prospectively capturing injury data rather than relying on self-report, (2) employing data collection methods and analyses that represent a player’s habitual and native mechanics and/or pitching characteristics, and (3) including multiple time points of data collection across a season or competitive year. Furthermore, standardized injury definitions or more objective units of injury (eg, injuries per 1000 pitches or 1000 athletic exposures) should be considered so that findings can be synthesized and more readily applied to clinical practice.
USA Baseball and MLB Pitch Smart Initiative List of Risk Factors for Arm Injuries of Baseball Players a
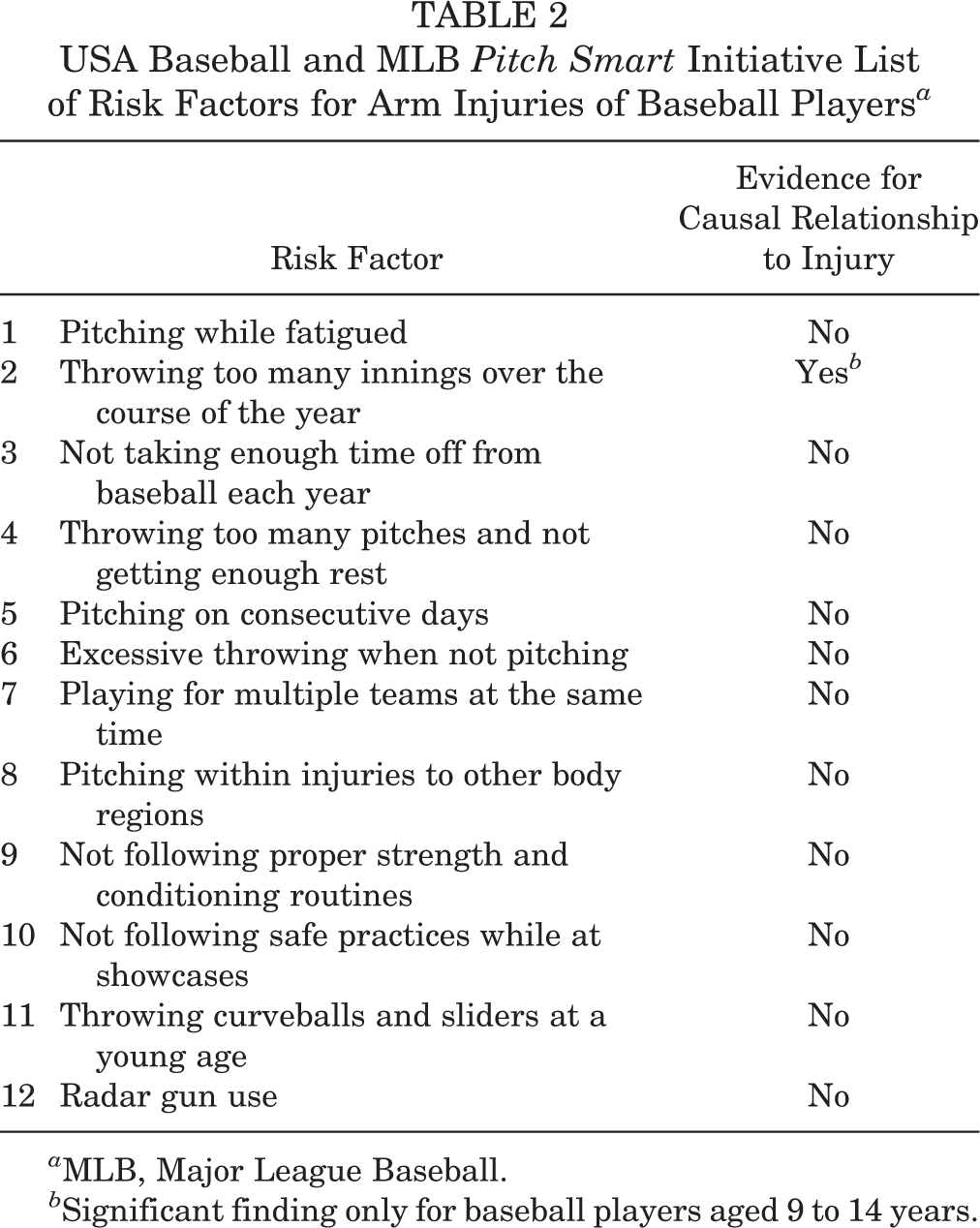
a MLB, Major League Baseball.
b Significant finding only for baseball players aged 9 to 14 years.
Conclusion
High-level evidence is lacking to substantiate current safety guidelines for baseball players. Only weak evidence exists to causally link risk factors such as age, position, and pitching volume to elbow injuries among baseball players, and no evidence exists to support any consistent causal risk factors related to shoulder injury. Well-designed prospective cohort studies are necessary to uncover risk factors related to injury among baseball players from the youth to professional level.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.F. is a consultant for Smith & Nephew, Integra, and Medical Device Business Service/DePuy-Mitek; has received research support from Smith & Nephew; has grants/grants pending from DJO; and has received hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
Appendix
Search Strategy for Electronic Databases Description of Criteria Used to Assess Risk of Bias in Selected Studies
a
Truly representative of the average baseball player in the community or along his athletic career trajectory* Somewhat representative of the average baseball player in the community or along his athletic career trajectory* Selected group of users No description of the derivation of the cohort Drawn from the same community as the exposed cohort* Drawn from a different source No description of the derivation of the nonexposed cohort Secure record (eg, medical records)* Structured interview* Written self-report No description
For this review, secure records also include adequate description of test or measurement protocol (equipment, experience of rater, measurement error, etc)
Yes* No
Studies indicating that all included athletes were injury-free at baseline received a star for this criterion
Study controls for the most important factor (stated in the background of the study)* Study controls for any additional factor*
For this criterion, studies could be awarded 2 stars
Independent blind assessment* Record linkage* Self-report No description Yes* No
Studies that carried out a follow-up period of at least 1 season received a star for this criterion
Complete follow-up of all participants accounted for* Participants lost to follow-up unlikely to introduce bias (up to 20% loss) or description provided of those lost* Follow-up rate <80% and no description of those lost No statement
A loss to follow-up >20% may increase the risk of bias in prospective studies
a
The articles could be awarded a maximum of 1 star (*) for each item, except for item 7, which could be awarded 2 stars. A total of 12 stars could be given for the articles. Risk-of-Bias Assessment for Included Studies
a
a
See Appendix Table A2 for descriptions of criteria and assignment of stars. Independent Variables Investigated for Association With Injury Across Different Levels of Play for Baseball
a
a
ABIR, abducted internal rotation; GIRD, glenohumeral internal rotation deficit; PER, prone external; ROM, range of motion. Odds ratio and 95% CI for risk factors related to elbow, shoulder, or general arm injury. Dashed vertical line represents “no effect.” ABIR, abducted internal rotation; GIRD, glenohumeral internal rotation deficit; PER, prone external; ROM, range of motion.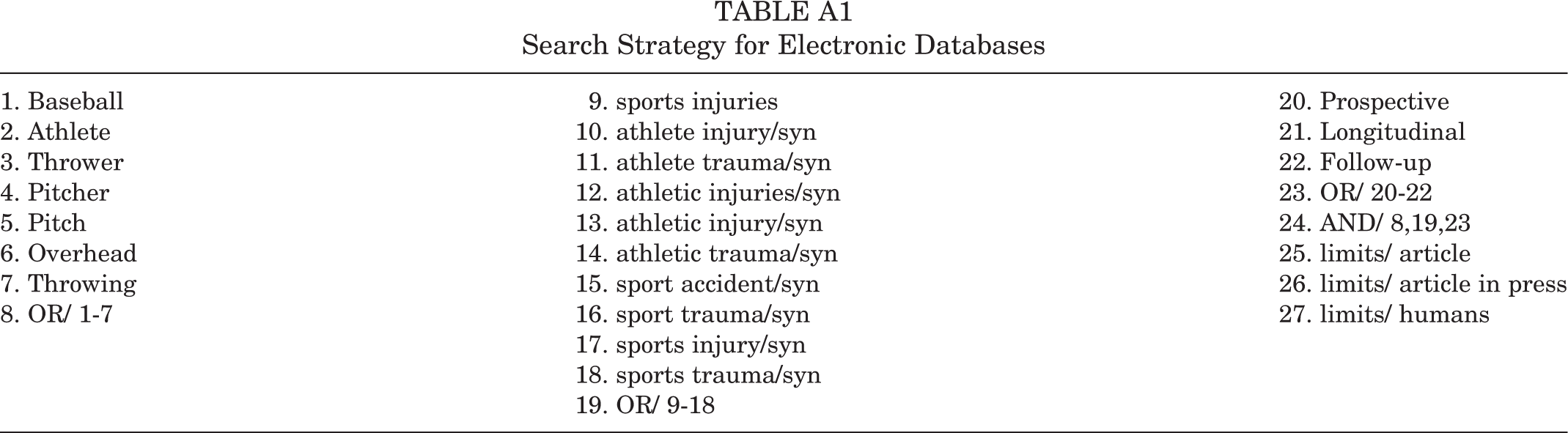
1. Baseball
9. sports injuries
20. Prospective
2. Athlete
10. athlete injury/syn
21. Longitudinal
3. Thrower
11. athlete trauma/syn
22. Follow-up
4. Pitcher
12. athletic injuries/syn
23. OR/ 20-22
5. Pitch
13. athletic injury/syn
24. AND/ 8,19,23
6. Overhead
14. athletic trauma/syn
25. limits/ article
7. Throwing
15. sport accident/syn
26. limits/ article in press
8. OR/ 1-7
16. sport trauma/syn
27. limits/ humans
17. sports injury/syn
18. sports trauma/syn
19. OR/ 9-18

Criterion
Description
1. Description of baseball player or type of baseball player
A description of the athlete’s level of play (eg, youth, high school varsity or junior varsity, minor or major league) and the position (eg, pitcher, catcher, infielder) is necessary to understand risk factors for injury across the athlete career trajectory. Studies that reported a description of the baseball player or information regarding the type of player studied received a star for this criterion
2. Definition of baseball-related musculoskeletal injury
An operational definition of the baseball-related injury is critical to synthesis of information. Studies that included a definition of baseball-related musculoskeletal injury received a star for this criterion
3. Representativeness of the exposed cohort
4. Selection of the nonexposed cohort
5. Ascertainment of exposure
6. Demonstration that the outcome of interest was not present in the study
7. Comparability of cohorts on the basis of the design or analysis
8. Assessment of the outcome
9. Appropriate follow-up period
10. Adequacy of follow-up of cohorts
11. Appropriate statistical measurement for risk association
Prospective studies should inform a statistical measure to determine risk association (eg, hazard ratio, odds ratio, relative risk) and the confidence interval. Studies that gave a statistical measure of risk received a star for this criterion
Criteria
Study
1
2
3
4
5
6
7
8
9
10
11
Anz
3
*
*
*
*
*
**
*
*
*
*
Bushnell
6
*
*
*
*
*
*
*
*
*
Byram
7
*
*
*
*
*
*
*
*
*
Chaudhari
11
*
*
*
*
*
*
*
*
*
*
Fleisig
18
*
*
*
*
*
*
**
*
*
*
Matsuura
29
*
*
*
*
**
*
*
*
Myers
30
*
*
*
*
*
*
*
*
*
*
Noonan
31
*
*
*
*
*
*
*
*
Polster
33
*
*
*
*
*
*
*
*
*
*
Shanley
37
*
*
*
*
*
*
*
*
*
*
Shitara
38
*
*
*
*
*
*
**
*
*
*
Tyler
39
*
*
*
*
*
*
*
*
*
*
Wilk
42
*
*
*
*
*
*
*
*
*
*
Wilk
43
*
*
*
*
*
*
*
*
*
*

Independent Variable
Study
Data Collection Method of Exposure
Collection Time Point
Specification of Independent Variable
Professional Players (Major and Minor League)
Elbow varus at maximum external rotation (fastest strike) pitching motion
Anz
3
(2010)
Motion capture system (Peak Performance Motus Systems; Peak Performance Technologies) captured at 120 Hz
Spring training (preseason)
Forearm rotation about the y-axis in local coordinate system at maximal shoulder external rotation phase of the pitching cycle
Shoulder external rotation torque at maximum external rotation (fastest strike) pitching motion
Motion capture system (Peak Performance Motus Systems; Peak Performance Technologies) captured at 120 Hz
Upper arm rotation about the y-axis in local coordinate system at maximal shoulder external rotation phase of the pitching cycle
Maximum pitch velocity
Bushnell
6
(2010)
Standard pitch velocity radar gun
Spring training (preseason)
Ball speed from fastest recorded pitch thrown for a strike during a spring training game.
Prone internal rotation strength at preseason
Byram
7
(2010)
Handheld dynamometer (PowerTrack II Commander; J-Tech Medical)
Spring training (preseason)
The median value of strength from 3 recorded trials
Prone external rotation strength at preseason
Handheld dynamometer (PowerTrack II Commander; J-Tech Medical)
The median value of strength from 3 recorded trials
Seated external rotation strength at preseason
Handheld dynamometer (PowerTrack II Commander; J-Tech Medical)
The median value of strength from 3 recorded trials
Supraspinatus strength at preseason
Handheld dynamometer (PowerTrack II Commander; J-Tech Medical)
The median value of strength from 3 recorded trials
Ratio of prone external rotation strength to prone internal rotation strength at preseason
Handheld dynamometer (PowerTrack II Commander; J-Tech Medical)
The median value of the calculated ratio from 3 recorded trials
Anterior-posterior pelvic tilt during single-legged raise test
Chaudhari
11
(2014)
iPod based tilt sensor (Level Belt Pro; Perfect Practice, Inc)
Spring training (preseason)
Degree of anterior pelvic tilt during single-legged raise test. Categories of anterior pelvic tilt were HI, poor lumbopelvic control (≥8.0°); MD, moderate lumbopelvic control (4.0°-7.9°); and LO, good lumbopelvic control (<4.0°).
Humeral torsion
Noonan
31
(2016)
Ultrasound (Sonosite, Inc) and digital inclinometer
Spring training (preseason)
Degree of forearm inclination angle with respect to the horizontal plane at the point where the apexes of the greater and lesser tubercles are parallel to the horizontal plane
Humeral torsion on dominant arm
Polster
33
(2013)
Computed tomography (Siemens Sensation 16; Siemens)
Not reported
The amount of torsion on the dominant arm. Torsion was measured as the distal humeral articular axis relative to the humeral head articular axis.
Humeral torsion difference
Computed tomography (Siemens Sensation 16; Siemens)
The amount of torsion difference on the dominant arm minus the nondominant arm. Torsion was measured as the distal humeral articular axis relative to the humeral head articular axis.
GIRD
Wilk
42
(2014)
Standard goniometer with bubble level
Spring training (preseason)
Difference between the internal rotation of the nonthrowing shoulder and the throwing shoulder of ≥20°
External rotation insufficiency
Standard goniometer with bubble level
External rotation of the throwing shoulder was not at least 5° more than the external rotation of the nonthrowing shoulder
Total rotation deficit
Standard goniometer with bubble level
Total rotation of the nonthrowing shoulder was at least ≥5° than the total rotation of the throwing shoulder
Flexion deficit
Standard goniometer with bubble level
Flexion of the nonthrowing shoulder was at least 5° more than flexion of the throwing shoulder
GIRD
Wilk
43
(2015)
Standard goniometer with bubble level
Spring training (preseason)
Difference between the internal rotation of the nonthrowing shoulder and the throwing shoulder of ≥20°
External rotation insufficiency
Standard goniometer with bubble level
External rotation of the throwing shoulder was not at least 5° more than the external rotation of the nonthrowing shoulder
Total rotation deficit
Standard goniometer with bubble level
Total rotation of the nonthrowing shoulder was at least 5° more than the total rotation of the throwing shoulder
Flexion deficit
Standard goniometer with bubble level
Flexion of the nonthrowing shoulder was at least 5° more than flexion of the throwing shoulder
High School Players
Scapular dysfunction assessment
Myers
30
(2013)
Tripod-mounted video camera (Sony MiniDV Handycam Camcorder of America)
Preseason
Classification of dysfunction during the scapular dysfunction test with operational definition from video assessment
Passive internal ROM difference
Shanley
37
(2011)
Standard goniometer with bubble level
Preseason
Difference between the mean dominant shoulder internal rotation value and the mean nondominant shoulder internal rotation value
Passive total ROM difference
Standard goniometer with bubble level
Difference between the mean dominant shoulder total rotation value and the mean nondominant shoulder total rotation value
ABIR in the dominant side
Shitara
38
(2017)
Digital protractor (iGaging) during passive ROM test
Preseason
Range of internal rotation shoulder motion when arm is abducted to 90°
PER ratio
Handheld dynamometer (PowerTrack II Commander; J-Tech Medical) during a make test
The ratio of dominant to nondominant side prone external rotation strength
Youth Players
Pitched at least 4 y
Fleisig
18
(2011)
Self-report via telephone survey occurring postseason and annually
Postseason
Pitched >100 innings in 1 y
Self-report via telephone survey occurring postseason and annually
How many innings pitched and for what teams during the past fall, winter, spring, and summer
Threw curveball before 13 y old
Self-report via telephone survey occurring postseason and annually
What type of pitches thrown in competition (fastball, curveball, etc) and whether player participated in any showcases
Played catcher at least 3 y
Self-report via telephone survey occurring postseason and annually
Whether the athlete played baseball during the past 12 mo and what position he played
Age
Matsuura
29
(2017)
Self-report via questionnaire completed by players with assistance from coaches and parents postseason
Postsummer championships
Position
Self-report via questionnaire completed by players with assistance from coaches and parents postseason
Most often played position
Baseball experience
Self-report via questionnaire completed by players with assistance from coaches and parents postseason
Unspecified
Training hours per week
Self-report via questionnaire completed by players with assistance from coaches and parents postseason
Time spent in practice, the bullpen, and games
History of shoulder pain
Self-report via questionnaire completed by players with assistance from coaches and parents postseason
Whether he experienced any pain from pitching or other throwing and where the pain was located
History of elbow pain
Self-report via questionnaire completed by players with assistance from coaches and parents postseason
Whether he experienced any pain from pitching or other throwing and where the pain was located
Passive internal rotation ROM
Tyler
39
(2014)
Digital level
Preseason
Degree of upper arm internal rotation movement while in supine with shoulder in 90° of abduction and elbow in 90° of flexion
Passive external rotation ROM
Digital level
Degree of upper arm external rotation movement while in supine with shoulder in 90° of abduction and elbow in 90° of flexion
Passive total ROM loss
Digital level
The difference in shoulder ROM between the dominant and nondominant arm
Posterior shoulder ROM loss
Digital level
Degree of upper arm cross-chest abduction movement while in side lying with the shoulder and elbow in 90° of flexion and scapula stabilized at axillary border by the tester
Supraspinatus strength
Held dynamometer (Lafayette Manual Muscle Tester) during a break test
Value of maximal resistance during break (empty can) test. Arm was fully inwardly rotated (thumbs down) with participant in sitting position and shoulder flexed to 90° in scapular plane and the elbow in full extension.
Scapular retraction strength
Held dynamometer (Lafayette Manual Muscle Tester) during a break test
Value of maximal resistance of downwardly directed forced during break test while in prone position with shoulder abducted 90° and elbow in 90° of flexion.
External rotation strength
Held dynamometer (Lafayette Manual Muscle Tester) during a break test
Value of maximal resistance during break test. Arm was in neutral position and participant placed in supine position with shoulder in 90° of abduction and elbow in 90° of flexion.
Internal rotation strength
Held dynamometer (Lafayette Manual Muscle Tester) during a break test
Value of maximal resistance during break test. Arm was in neutral position and participant placed in supine position with shoulder in 90° of abduction and elbow in 90° of flexion.