
Abstract

Keywords
The term “hip pointer,” coined by Blazina 1 in 1967, refers to an injury involving direct trauma to the iliac crest that causes a contusion or subperiosteal hematoma. Such injuries are common in collision sports. 2,5 This case report presents 2 professional Australian rules football players from the Sydney Swans Football Club who sustained a serious variant of the hip pointer injury during match play. These 2 athletes sustained internal degloving and avulsion injury to the internal oblique insertion on the iliac crest, with resultant significant hematoma formation. The internal oblique muscle originates from the iliac crest, thoracolumbar fascia, and inguinal ligament and inserts into the inferior borders of ribs 10 through 12 and the linea alba. 6 This muscle allows flexion and rotation of the trunk while supporting and compressing the abdominal viscera; hence, damage to any part of the muscle can be significantly debilitating, especially to a professional athlete.
The typical hip pointer injury is characterized by localized pain and severe palpable tenderness along a variable distance of the iliac crest. Athletes can often return to the field of play, and in professional sports their pain can be controlled with local anesthetic injection. These athletes usually recover in 1 to 3 weeks. We present a more serious variant of this injury, where pain is most severe at the time of injury, the pain and tenderness extend from the iliac crest into the nearby anterolateral abdominal wall, the pain is poorly controlled by local anesthetic injection, and the athlete experiences notable morbidity and needs numerous weeks or months to recover.
This case report outlines the clinical presentation, investigation, and management of this rare but important injury.
Case Report
Informed written consent was obtained from both athletes for access to clinical information, radiological investigations, and clinical photographs. Approval was granted from the Sydney Swans Football Club.
Both athletes sustained a traumatic blow to their iliac crest from accidental collision with an opponent in a “marking contest” during competition. Athlete 1, a 29-year-old male, sustained a direct blow from an opponent’s elbow (Figure 1). Athlete 2, a 25-year-old male, sustained a disruptive injury to the internal oblique insertion when he was struck by an opponent’s knee.

Athlete 1 being struck accidentally by an opponent’s elbow in a marking contest.
Athlete 1
Athlete 1, who is a 200-cm-tall forward and a left foot–dominant kicker, was injured during competition by an accidental traumatic blow from an opponent’s elbow and left the field of play immediately for medical attention. The provisional diagnosis was a hip pointer injury, given the mechanism of injury outlined above. The athlete limped unaided into the medical rooms, away from the field of play, for assessment. It was immediately apparent that the athlete was troubled by severe pain and dysfunction. He had no previous injury to the hip, pelvis, or abdominal wall. He indicated that the pain affected a broad region involving the left iliac crest and left lower anterolateral abdominal wall. He was unable to perform a sit-up and was maximally tender at the superior border over the middle third of the left iliac crest and the adjacent lower anterolateral abdominal wall. His abdomen was soft to palpation, and his left hip and buttock were normal upon examination.
In professional sports, it is not uncommon to offer athletes guided or unguided local anesthetic injection for hip pointer injury to enable them to return to the field of play. 8 Athlete 1 was treated initially with 20 mL of 0.75% ropivacaine by unguided injection to the 2 sites of maximal tenderness over the superior border of the left iliac crest. Unguided injection requires an understanding of the anatomic features of the iliac crest and anterolateral abdominal wall. The provider palpates the site of maximal tenderness; then, after thoroughly cleansing the skin and using aseptic technique, the provider uses 2-finger palpation on either side of this site to administer local anesthetic via a 22-gauge needle. Great care is taken to use anatomic landmarks in order to avoid injecting the anesthetic intra-abdominally, and no injection is given without aspirating first.
Athlete 1 returned to the field of play for 10 minutes and then voluntarily returned to the sideline stating that his pain was poorly controlled. At this stage, it was suspected that the athlete had sustained a severe variant of hip pointer injury. He was once again taken to the medical room and assessed, where a thorough and complete examination of his abdomen was once again undertaken to exclude intra-abdominal and intrapelvic injury. Splenic, kidney, or bowel injury in particular should be high on the differential. All clinical examination findings were negative for severe generalized abdominal or loin pain. The athlete showed no abdominal wall guarding or rebound tenderness.
Given that the maximal dose of ropivacaine is 3 mg/kg and this athlete weighed 100 kg, a further 10 mL of 0.75% ropivacaine was injected to a third site on the superior border of the left iliac crest. The athlete subsequently returned to the field of play and completed the game, playing with low-grade pain and mild dysfunction for a further 45 minutes.
After the game, athlete 1 required regular ice and simple analgesics to manage his pain. He was assessed at the injury clinic 48 hours after the injury; on examination, he continued to be troubled by significant pain and had obvious ecchymosis over the area of injury (Figure 2). Athlete 1 showing ecchymosis on the left anterolateral abdominal wall on day 3 postinjury.
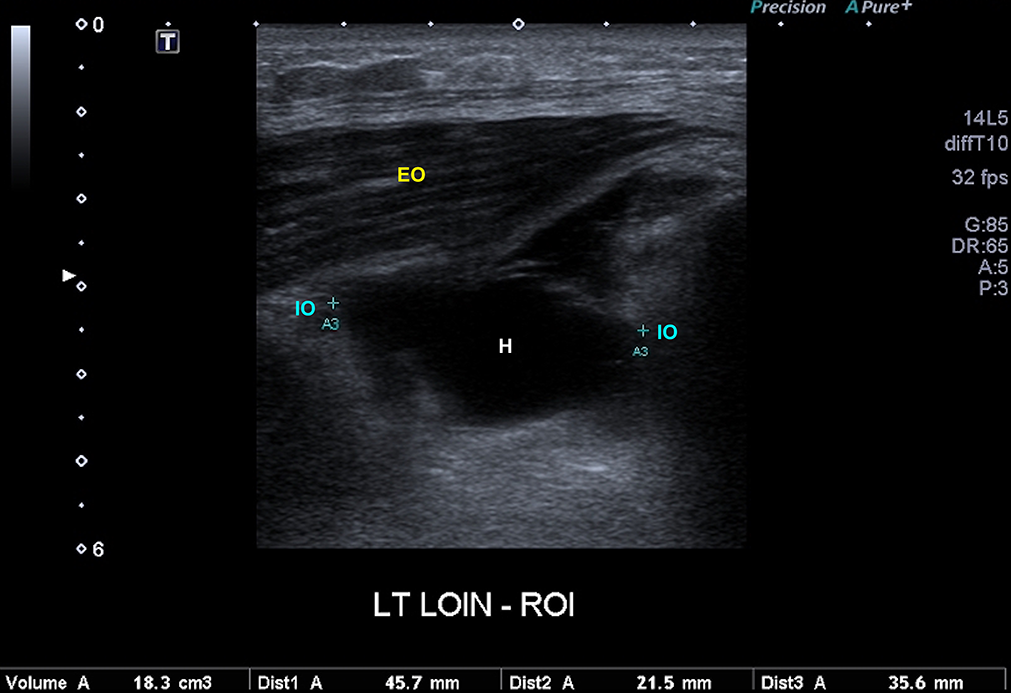
Day 4 ultrasonography results for athlete 1. EO, external oblique; H, hematoma; IO, torn internal oblique.
Seven days after the initial injury, a radiologist performed a pregame ultrasound-guided aspiration of 10 mL of blood and a subsequent injection of 15 mL of 0.75% ropivacaine along the middle one-third of the left iliac crest (Figure 4). This failed to control the athlete’s pain, and thereafter a further 15 mL was injected along the anterior left iliac crest. Athlete 1 played the entire game with only low-grade pain and dysfunction.

Match day ultrasound-guided aspiration and local anesthetic injection for athlete 1.
The primary rationale for aspirating the hematoma in the days after the injury and for injecting corticosteroid was to decrease the pain experienced by the athlete and thereby allow expeditious return to play.
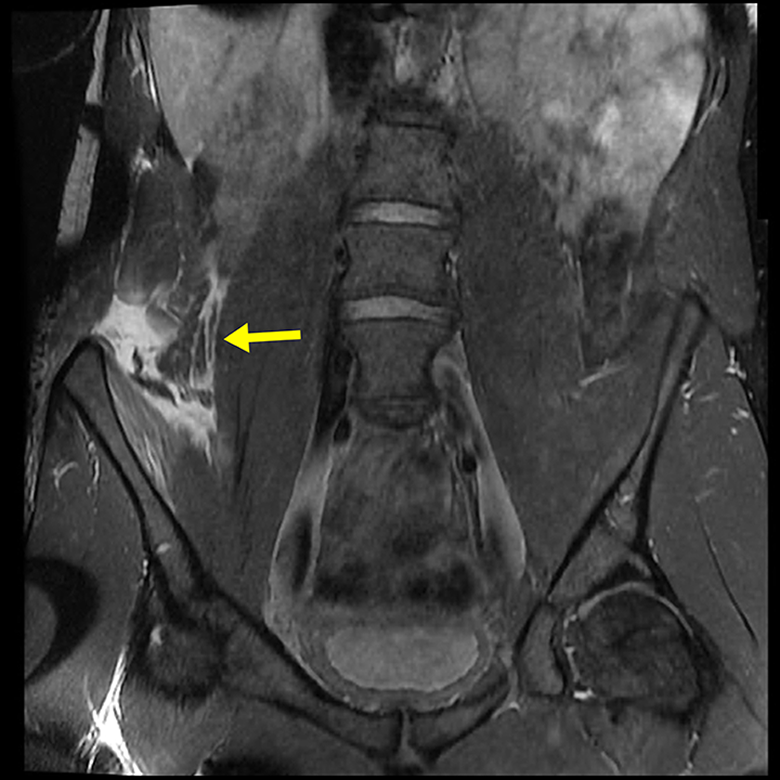
Nine days after the injury, the medical team decided to investigate the injury with a magnetic resonance imaging (MRI) examination of the left iliac crest and lower anterolateral wall (Figure 5). Day 9 coronal magnetic resonance image for athlete 1. Arrow points to internal oblique. EO, external oblique; H, hematoma; IO, internal oblique; TA, transversus abdominis.
Given that we had never diagnosed this particular sports medicine injury, a surgical opinion was sought from a general surgeon specializing in abdominal wall hernias. All imaging was reviewed by this surgeon and the case was discussed clinically, where it was determined that surgical intervention was not indicated. It was the surgeon’s opinion that surgery posed a risk of introducing infection and that the injury would heal.
Eleven days after the injury, athlete 1 had a further 25 mL of hemoserous fluid aspirated and, on this occasion, 6 mL of autologous platelet-rich plasma (PRP) was injected in an effort to enhance healing. After this, no clinic-based aspirations or injections were performed.
Following the injury, athlete 1 underwent a staged rehabilitation under the care of the physical therapy and strength and conditioning team. This entailed an initial anti-inflammatory phase involving rest, ice, compression, and analgesic medication in the days after the injury combined with the ultrasound-guided aspirations and injections outlined above. Five days after the injury, he underwent a fitness test during training that involved participating in a full team training activity that simulated competition, 2 days before match day, and he passed this test. He did, however, avoid contacts and collisions at training. He provided consent for match day ultrasound-guided local anesthetic, in combination with a thermoplastic shield guard over his left iliac crest, to enable him to play.
Athlete 1 played a further 4 games (all finals) in season 2016, culminating in the grand final, whereby before each game he underwent ultrasound-guided aspiration of the hematoma and injection of ropivacaine to be able to play. During this entire time, he was involved in a graded strengthening program for his lumbopelvic region, initially focusing on isometric co-contractions and progressing to more challenging exercises involving planking and side planking to strengthen and remodel the damaged anterolateral abdominal wall. In the later stages of his rehabilitation, he performed dynamic strengthening of the thoracolumbar region, using gym equipment (free weights, pulleys, and clinical Pilates).
Athlete 1 recovered during the off season (8 weeks) and made a complete pain-free recovery, having normal strength on his return. After 18 months, a follow-up MRI (sagittal imaging only) was conducted and showed complete resolution of the hematoma related to the internal oblique muscle strain at the iliac crest with some scarring and fatty change in the muscle defect. The MRI revealed no anatomic reattachment of the internal oblique muscle to the iliac crest but rather an area of fibrosis (Figure 6).

Follow-up magnetic resonance image of athlete 1 at 18 months postinjury.
Athlete 2
Athlete 2, who is a 204-cm-tall ruckman, right foot–dominant kicker, was injured during competition by the same mechanism as outlined above. As with athlete 1, athlete 2 left the field of play for immediate assessment and was found to be disabled by severe, poorly localized pain to his right iliac crest and anterolateral abdominal wall. He was assessed in the medical rooms, where it was immediately suspected that a disruptive injury to the lower anterolateral abdominal wall was the most likely diagnosis. Athlete 2 presented in a very similar way to athlete 1, but with more significant pain and dysfunction. A palpable defect was clinically apparent upon examination of the insertion of the lower anterolateral abdominal wall along a distance of more than 5 cm on the superior aspect of the right iliac crest. Thorough abdominal and pelvic examinations were performed and, as with athlete 1, was found to be normal. At this stage, it was highly suspected clinically that athlete 2 had sustained an injury similar to that of athlete 1.
The gravity of the suspected injury was discussed with athlete 2. Consent was given for local anesthetic injection, and the player understood that attempting to continue play could aggravate his injury and affect his recovery. Because the injury occurred early in the game, a trial of local anesthetic injection (ropivacaine 0.75%, 25 mL) was performed along the area of maximal tenderness over the superior margin of the right iliac crest. The athlete returned to the field of play for a further 10 minutes, until the half-time break. A further 10 mL of local anesthetic was injected at half-time because of ongoing severe pain and dysfunction. Given that the game was closely contested and the athlete played in a key position, he attempted to play for a further 25 minutes but was troubled by significant pain and dysfunction and eventually left the field of play. Unlike athlete 1, athlete 2 developed pain referring into his right hip flexor and right groin, and his running gait and kicking ability were grossly impaired.
Athlete 2 required more analgesic medication in the days after his injury. Given the high index of suspicion for a disruptive injury of the anterolateral abdominal wall, similar to athlete 1, he was investigated promptly with an MRI 3 days after the injury (Figure 7). The MRI showed an acute tear of the internal oblique at its iliac crest insertion extending over an 80-mm anteroposterior length as well as muscle retraction measuring approximately 25 mm craniocaudally. The site of the focal tear was filled with liquefying hematoma, analogous to athlete 1. An ultrasonography of the right anterior abdominal wall was conducted, where 5 mL of 1% xylocaine was infiltrated before aspiration of 15 mL of frank blood, and thereafter 5 mL of PRP was infiltrated into the region. PRP was used rather than cortisone for several reasons, the primary reason being that athlete 2 had a more significant and disruptive injury compared with athlete 1 and we wanted to shorten the rehabilitation time compared with athlete 1; as described above, athlete 1 appeared to respond favorably to PRP when this treatment was used. The rationale for repeated aspiration and PRP injection was to evacuate the hematoma, oppose the soft tissues, facilitate healing of the defect, and expedite an early return to play.
Day 3 magnetic resonance image of athlete 2 with arrow indicating area of muscle retraction and hematoma.
On day 5, the ultrasonographic procedure was repeated, with 3 mL of frank blood aspirated and a further 5 mL of PRP injected. On day 7, 25 mL of hemoserous fluid was aspirated and 5 mL of PRP injected. On day 9, 40 mL of hemoserous fluid was aspirated; at this stage, fluid was sent for pathological analysis and no further injections of PRP were administered. No remarkable findings were reported on pathological analysis; in particular, the cell count and culture demonstrated no infection. A follow-up MRI on day 13 demonstrated a persistent seroma measuring 3.2 × 3.5 × 4.7 cm, with persistent detachment of the internal oblique from the iliac crest. On day 14, a further 20 mL of hemoserous fluid was aspirated. Serial ultrasonography performed thereafter demonstrated resolution of the seroma and partial healing of the internal oblique avulsion.
Although it was hoped that the PRP injections would facilitate healing, athlete 2 had a much more prolonged rehabilitation compared with athlete 1 and returned to play 6 weeks after initial injury. Given the knowledge of the injury that the medical team had acquired from managing athlete 1, athlete 2 was rehabilitated in a very similar fashion, with an initial period of anti-inflammatory measures, followed by a staged strengthening and remodeling phase. Compared with athlete 1, athlete 2 experienced more severe pain and dysfunction, which prolonged his rehabilitation. In particular, athlete 2 was greatly troubled by right hip flexor pain and weakness, associated with his hematoma/seroma gravitating through the tissue planes from his iliac crest into the hip flexor and iliac fossa region, profoundly affecting gait and kicking capacity.
Unlike athlete 1, athlete 2 did not require local anesthetic injections to play on his return. Both athletes used thermoplastic guards over their injured iliac crest to minimize further trauma. As with athlete 1, athlete 2 made a pain-free return to full function during the off-season period.
Athlete 2 had a follow-up MRI (sagittal imaging only) 6 months after injury, and this demonstrated findings identical to those of athlete 1 (Figure 8). The difference in the time to follow-up MRI between athletes 1 and 2 was attributed to circumstance. In neither athlete was a clinical or radiological hernia seen.

Follow-up magnetic resonance image of athlete 2 at 6 months postinjury.
Discussion
Australian rules football is a collision sport. Players are particularly at risk of contact in marking contests, in which athletes commit to marking a ball overhead and during which numerous players may collide (see Figure 1).
The iliac crest is essentially subcutaneous, and blunt trauma to it can result in significant hematoma formation and subperiosteal bleeding, in what has been termed a hip pointer injury. 1,5 The contusion can be located anywhere along the crest, from the anterior superior iliac spine to the posterior superior iliac spine, and can be located inferiorly at the gluteal musculature insertion or superiorly along the anterolateral abdominal wall insertion on the crest. The anterolateral abdominal wall, which consists of the external oblique, internal oblique, and transversus abdominus, is illustrated in Figure 9 and described in anatomic texts. 6 The internal oblique originates from the iliac crest, thoracolumbar fascia, and inguinal ligament and inserts into the inferior borders of the 10th to 12th rib and the linea alba. All 3 muscles of the anterolateral abdominal wall protect the abdominal viscera while allowing for flexion and rotation of the trunk.

Anatomic features of the anterolateral abdominal wall showing (A) superficial, (B) middle, and (C) deep layers. Reprinted with permission from Stensby J, Baker J, Fox M. Athletic injuries of the lateral abdominal wall: review of anatomy and MR imaging appearance. Skeletal Radiol. 2015;45(2):155-162.
Numerous reports in the literature have described indirect injury to the internal oblique muscle proximal origin over 1 or more costal cartilages. This injury has been named a “side strain.” 3 Radiological studies 9 on the above-mentioned severe variant of hip pointer have been reported, but only 1 case report 7 has described an indirect injury to the internal oblique distally, and no clinical case reports are available on “direct” traumatic injury to the insertion of the internal oblique.
The assessment of routine hip pointers usually does not involve radiological investigation, and most of these injuries are managed clinically. 5 The athlete’s symptoms and clinical signs are well localized to the iliac crest. It is common practice in professional athletes to treat pain with a guided or unguided local anesthetic injection to enable them to return to play on the same day or subsequent days to weeks. Although uncommon, iliac crest fractures can occur in collision sports, and an inability to return to play after a local anesthetic injection would warrant radiography to rule out a fracture.
This case report describes a more serious variant of the hip pointer mechanism of injury, whereby a traumatic glancing blow (by a knee, elbow, etc) causes an internal avulsion injury of 1 or more layers of the anterolateral abdominal wall. In both patients in this study, similar to the small number of studies published to date, 7,9 a partial avulsion of the distal anterolateral abdominal wall was documented on ultrasonography and MRI. Both cases involved a variable avulsion of the internal oblique muscle insertion along the iliac crest. A more significant disruption in both the anterior to posterior and craniocaudal planes resulted in a significantly longer rehabilitation time for athlete 2. Athlete 2 had less retraction (25 mm) than athlete 1 (35 mm); hence, we believe that the length of the avulsed muscle may be more predictive of the severity than the amount of retraction. The athletes described severe pain over a variable distance over their iliac crest on the superior aspect and a variable distance of pain radiating into the nearby anterolateral abdominal wall. If the disruption of the anterolateral abdominal wall is significant, pain and dysfunction can involve not only the abdominal wall but also the ipsilateral hip flexor region, as seen in athlete 2.
A useful clinical test, not only to initially diagnose the injury but also to track recovery, is the “resisted oblique sit-up test”; this maneuver entails stressing the involved anterolateral abdominal and assessing pain and strength, while palpating for a palpable defect or tenderness (Figure 10).

Athlete 2 performing a resisted oblique sit-up test.
Given the limited discussion of traumatic partial avulsion of the anterolateral abdominal wall in the literature—1 review in the radiological 9 literature, without clinical details, and a single case report of 1 athlete with a “noncontact indirect” avulsion injury 7 —we have named this injury the “Franklin-Naismith lesion” in honor of athletes 1 and 2, respectively. Naming this injury after the athletes gives recognition for their dedication to sport and research, as previously done with the naming of the Tommy John surgery.
Trauma over the pelvis and greater trochanter can result in subcutaneous degloving injuries, where a large hematoma or seroma develops subcutaneously and is bounded internally by the fascia (eg, the Moral-Lavallee lesion). These significant injuries are often complicated by infection and the need for surgical evacuation and repair. 4 Complete avulsion of all 3 layers of the anterolateral abdominal wall has been described 9 and most often results from high-energy trauma (motor vehicle accidents). These injuries have been associated with significant complications, including prolonged pain, dysfunction, and the development of lumbar hernia, requiring surgical intervention. 9
Injury to the proximal attachment of the anterolateral abdominal wall has been well described 3,9 and is usually associated with a noncontact eccentric muscular contraction, a mechanism of injury associated with racquet sports, particularly tennis, as well as fast bowling in cricket.
As described, we sought the opinion of a specialist surgeon, who recommended nonsurgical treatment. It is unknown whether surgical repair would have resulted in a better or worse final outcome or would have altered the period of disability. Possible complications that were anticipated included infection of the hematoma/seroma (in particular iatrogenic infection from multiple aspirations and injections), lumbar hernia 9 (usually associated with disruption of all 3 layers of the anterolateral abdominal wall) (Figure 9), nerve entrapment, intra-abdominal or intra-pelvic injury, prolonged and/or recurrent pain, weakness, and dysfunction. The risk of complications such as lumbar hernia is unknown for this sports-related disruptive injury of the anterolateral abdominal wall but is thought to be low.
Given the paucity of knowledge and publications regarding the injury, the medical team treated this injury on first principles. In the context of professional sports medicine, a safe and expeditious return to play is paramount. For this reason, we decided to drain the associated hematoma/seroma on multiple occasions for both athletes and also to use corticosteroid and PRP injection into the hematoma/seroma after drainage in an attempt to expedite recovery, reduce pain, oppose the soft tissues, and improve healing. It is possible that steroid injection may have delayed healing of muscle-tendon units, hence our reasoning to follow with PRP injection. We believed the combination of aspiration, steroid injection, and PRP injection would relieve pain and minimize swelling and hematoma. However, we recognize that no reliable evidence exists for the use of PRP in muscle avulsion injuries, and our clinical reasoning was based on first principles. Given that this series included only 2 athletes, it is difficult to ascertain the correct treatment algorithm for this injury in terms of the use of PRP and/or cortisone injections. It remains unknown whether this intervention is better than a more conservative approach with no guided aspirations or injections. Corticosteroid injection may possibly inhibit healing and delay recovery, and therefore we do not recommend this treatment for this particular injury.
On the day of injury, both athletes used protective guards over their iliac crest and were injected with ultrasound-guided local anesthetic. Athlete 1 continued with local anesthetic injections when he returned to play on subsequent match day, whereas athlete 2 did not require local anesthetic injections on match day upon his return. Ropivacaine, given its safer toxicity profile (in particular cardiotoxicity and neurotoxicity), was used on match day, whereas bupivacaine was used during the week for therapeutic aspiration and injection. The ethics of local anesthetic injection in professional athletes is contentious, and it remains unproven whether the athletes’ morbidity and recovery were adversely affected by this approach. However, no short-term complications, such as infection, occurred from our use of local anesthetic injections.
As mentioned above, the recognition of the Franklin-Naismith lesion was immediate in athlete 2 based on the experience of athlete 1. Prompt identification of the injury allowed earlier focused treatment. This, however, did not improve the second athlete’s return to play. In the future, strategies that could decrease hematoma formation (rest, compression, thrombotic agents, etc) might allow for a more rapid recovery for these injuries.
No universally accepted rehabilitation protocol or timeline is available for these rare injuries. First principles were adopted by the physical therapy team in a step-by-step approach that included rest, mobilization, strengthening, and gradual return to play.
Conclusion
It is our hope that medical practitioners will be able to clinically recognize the Franklin-Naismith lesion and to differentiate this injury from an uncomplicated hip pointer injury. This will enable early recognition, early investigation, and the prompt care of the patients. Further studies with larger numbers of patients are recommended to facilitate greater knowledge on how to best manage this injury.
Footnotes
Acknowledgment
The authors thank Dr Phil Lucas, PRP Imaging Group, Moore Park, Sydney; Dr David Samra and Dr Matt Cameron of the Physiotherapy and Rehabilitation Team at Sydney Swans Football Club; Mr Lance Franklin, Mr Sam Naismith, and Mr Anthony Cahill, Sydney Swans Football Club; and Dr Riza Gultekin.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.