
Abstract
Background:
Traditionally, the primary outcome in meniscal allograft transplantation (MAT) has been long-term survivorship; however, short-term clinically significant outcomes are necessary to fully evaluate patient improvement after surgery.
Purpose:
To (1) establish the minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS) with respect to patient-reported outcome measures (PROMs) and (2) evaluate preoperative and intraoperative variables correlated with achieving these threshold values.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
A prospectively maintained institutional registry was queried for all MATs performed between 1999 and 2017. The following PROM scores were collected: International Knee Documentation Committee (IKDC) score, Lysholm score, and Knee injury and Osteoarthritis Outcome Score (KOOS). Patients who completed preoperative and postoperative PROMs within a 1-month window were included to calculate the distribution-based MCID at this interval. An anchor question regarding satisfaction with surgery was asked at the same time point and was employed to determine the PASS using nonparametric receiver operating characteristic curve/area under the curve analysis. Multivariate regression analysis was performed to correlate patient demographics, medical history, and concomitant procedures to propensity in achieving the MCID and PASS.
Results:
A total of 98 patients who underwent MAT met the inclusion/exclusion criteria, of whom 10 underwent concomitant ligamentous procedures, 65 underwent concomitant cartilage procedures, and 7 underwent concomitant realignment procedures. The mean patient age was 29.4 ± 9.0 years, and the mean body mass index (BMI) was 26.8 ± 5.2 kg/m2. The distribution-based MCID and PASS were determined for the Lysholm score (12.3 and 66.5) and IKDC (9.9 and 36.0) as well as the KOOS Pain (9.9 and N/A ), Symptoms (9.7 and 73.0), Activities of Daily Living (9.5 and N/A), Sport (13.3 and N/A), and Quality of Life (14.6 and 53.0) subscales, respectively. A preoperative Short Form Physical Component Summary (SF PCS) score greater than 32.0 was predictive of postoperative satisfaction. Patients with work-related claims had a reduced likelihood of achieving the MCID for the IKDC and the PASS for the KOOS Symptoms. An increased BMI was also associated with failing to achieve the PASS for the KOOS Quality of Life (QOL).
Conclusion:
This study established the MCID and PASS for the Lysholm score, IKDC, and KOOS in patients undergoing MAT. Workers’ compensation and higher BMI were associated with failing to achieve clinically significant values. Lower preoperative Lysholm, IKDC, and KOOS scores were predictive of achieving the MCID, while higher preoperative SF PCS scores were associated with achieving satisfaction after MAT.
Keywords
Meniscal allograft transplantation (MAT) has been shown to restore force distribution lost by meniscus-deficient knees. 27,40 In appropriately selected candidates, MAT is a viable procedure for joint preservation, although future research will always be needed for methods to gain optimum results. 20,24,37 Given appropriate preliminary results, clinical practice guidelines must be constructed from research to provide the optimal methodology of MAT. An increasing focus is being placed on clinically significant results over statistically significant results to demonstrate clinical benefit. 15
Traditionally, outcomes in MAT studies have involved survivorship in delaying knee arthroplasty. In the short-term and midterm time frame, outcomes after MAT are heavily reliant on subjective outcome scores to evaluate patient improvement. As such, statistically significant differences between these subjective scores do not provide robust evidence of treatment efficacy from which to base practice guidelines. 15 The minimal clinically important difference (MCID), which is the most well-known clinical outcome threshold, reflects the threshold difference between preoperative and postoperative scores needed to differentiate patients who demonstrate no change after surgery from those who demonstrate minimal improvement after surgery. 25 This score is calculated through either a distribution- or anchor-based methodology and may be correlated with preoperative and intraoperative variables. The patient acceptable symptomatic state (PASS) reflects the postoperative score that is associated with patient satisfaction. 25 These clinically significant outcomes are critical to document patient improvement after surgery. By employing these measures, outcomes after surgery may be stratified into achieving a minimally improved state or satisfactory state. Further research regarding MAT may also employ these thresholds to sufficiently power trials, as the ability to achieve a minimal improvement would confer clinical significance. Additionally, in assessing outcomes by these threshold measures, clinicians may discuss with patients the reasons for not achieving these thresholds at shorter intervals and strategize alternative options.
Establishing these threshold scores specific to a procedure of interest allows physicians to reliably measure clinical improvements after surgery. 25 The “pay for performance” model of health care is trending to replace the “fee for service” model, and therefore, clinical outcomes will be further emphasized in the near future. 14 Therefore, subjective clinically reported outcome measures are important in demonstrating quality-based care, particularly because survivorship models cannot be used in the short term. A higher threshold is accomplished by clinically significant outcomes and should be preferred over statistical significance in optimizing techniques.
The goal of this study was to establish the MCID and PASS with respect to patient-reported outcome measures (PROMs) for MAT and to evaluate preoperative and intraoperative variables correlated with achieving these threshold values. The hypothesis of this study was that specific differences between preoperative and postoperative scores are accurately able to predict patient perception of improvement and satisfaction after MAT.
Methods
Study Design
The present study was a retrospective review of prospectively collected patient-reported outcomes. An institutional registry was queried for all patients who underwent MAT between 1999 and 2017 with a minimum 1-year follow-up. Patients were included in the study regardless of concomitant procedures. Patients were excluded if they failed to complete their patient-reported outcome questionnaire within 1 month of receiving it, to ensure that captured improvement was reflective of the 1-year time interval. Each patient received an electronic copy of the questionnaire every 5 days for a period of 1 month. The questionnaire was not extended beyond 1 month, to prevent heterogeneity of the outcomes. Outcomes were recorded via an electronic data collection service (Outcome Based Electronic Research Database; Universal Research Solutions). Institutional review board approval was acquired before initiation of this study.
Patient-Reported Outcome Measures
A total of 3 outcome scores were collected during the included time frame: The subjective International Knee Documentation Committee (IKDC) score, 12 Lysholm score, 23 and Knee injury and Osteoarthritis Score (KOOS). 36 The KOOS is stratified into 5 separate subscales: Pain, Symptoms, Activities of Daily Living (ADL), Sport, and Quality of Life (QOL). These outcome scores were collected preoperatively and at 1-year follow-up.
Anchor Questions
An additional anchor question regarding satisfaction was instituted in 2010. Patients were asked the following: “In retrospect, would you still proceed with the meniscus transplant having now experienced the entire process?” This anchor question was used in the calculation of the PASS and also as a binary outcome metric to establish satisfaction with the procedure.
Patient Selection
Inclusion criteria for MAT included age <40 years, an absent or nonfunctional meniscus, and pain with activity. Exclusion criteria included uncorrected varus/valgus malalignment, uncorrected knee instability, diffuse arthritic changes, bony architecture changes, inflammatory arthritis, and synovial disease. Concomitant distal femoral osteotomy, high tibial osteotomy, and cartilage restoration were performed only when indicated to give the transplant the best chance of success. High tibial osteotomy was indicated in patients with varus alignment with no ligamentous instability and good range of motion but was not performed in those who had severe articular damage, tricompartmental arthrosis, or patellofemoral arthrosis. Distal femoral osteotomy was indicated in patients with a valgus deformity >12° to 15°, joint line obliquity >10°, flexion of at least 90°, and <15° of flexion contracture. Osteochondral allograft transplantation was reserved for patients with isolated, full-thickness chondral lesions >1 cm in diameter to the ipsilateral side of the transplant that were recalcitrant to nonoperative therapy. All concomitant procedures were performed at the time of MAT.
Surgical Technique and Rehabilitation Protocol
The senior author’s (B.J.C.) preferred technique for MAT has been previously published. 5,6,26 When present, associated abnormalities (cartilage defects, anterior cruciate ligament [ACL] insufficiency, varus/valgus malalignment) were treated concomitantly. All MAT procedures were performed with a bridge-in-slot technique for either the medial or lateral side, with the exception of patients undergoing concurrent ACL reconstruction, in which case the bone slot was modified to facilitate ACL graft placement. 5,9 Cartilage defects were treated utilizing a previously described algorithm. 7 In all cases, the meniscal allograft was sized according to a previously published protocol. 42 Fresh-frozen, nonirradiated meniscal allografts were used.
The postoperative rehabilitation protocol has been previously described, 5 with 6 to 8 weeks of protected heel-touch weightbearing, locked flexion of 0° to 90°, heel slides, quadriceps sets, and straight-leg raises. The patient was advanced to full weightbearing, closed chain strengthening, and cycling by 12 weeks. Progression to sport-specific activities and full training was permitted by 20 weeks postoperatively, with alterations to account for concomitant procedures as necessary.
Data Collection
In total, 98 patients met the inclusion/exclusion criteria and completed both preoperative and postoperative questionnaires in the time window (Table 1). Baseline demographics were compared between patients lost to follow-up and included study patients to account for selection bias. Medical records were retrospectively reviewed for all preoperative and intraoperative variables, including sex, workers’ compensation status, smoking status, body mass index (BMI), age, concomitant procedures, number of cartilage defects and corresponding Outerbridge classification, focal cartilage lesion area (cm2), number of prior surgeries, and medial versus lateral transplant. All variables were reviewed with respect to outcome measures.
Baseline Patient Characteristics of All Patients Undergoing Meniscal Allograft Transplantation a
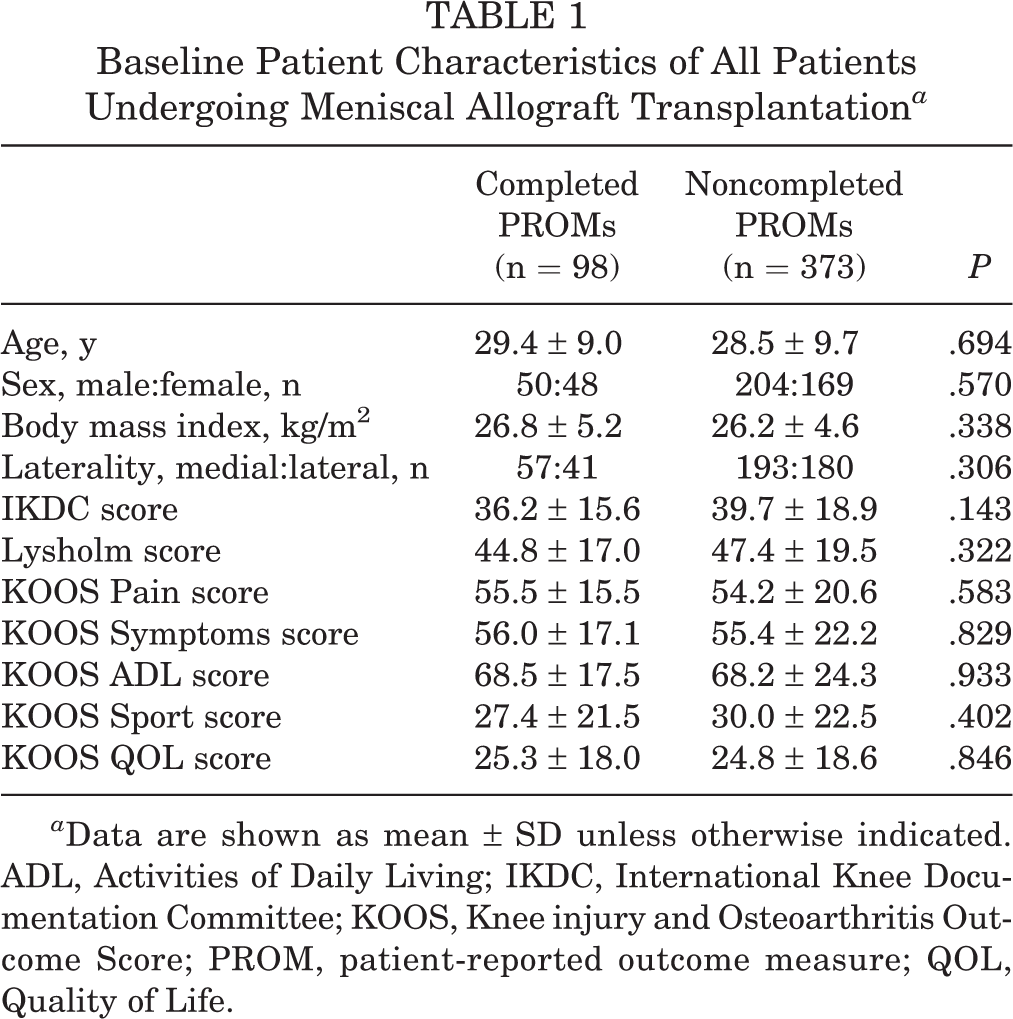
a Data are shown as mean ± SD unless otherwise indicated. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PROM, patient-reported outcome measure; QOL, Quality of Life.
Statistical Analysis
Statistical analysis was performed using RStudio software version 1.0.143 (RStudio). The distribution-based method was used to calculate the MCID, as the standard deviation of the difference between preoperative and postoperative scores was halved. Previous literature supports the reliability of this method in establishing the MCID. 2,4,32,33,35,47 Available satisfaction scores were used to calculate the PASS using the anchor-based methodology. The postoperative PROM scores from unsatisfied patients were compared with those of satisfied patients, and receiver operating characteristic (ROC) curve/area under the curve (AUC) analysis was used to determine the appropriate threshold in postoperative PROMs to differentiate between satisfied and unsatisfied patients. An acceptable predictive value was defined if the AUC was >0.7 and excellent if >0.8. 1,2 The Youden index was then used to calculate the threshold at which sensitivity and specificity were maximized. The MCID and PASS were calculated for the Lysholm score, IKDC, and all subscales of the KOOS. Last, univariate and multivariate analyses were performed to determine which factors were correlated to achieving the MCID or PASS. Variables were included in multivariate regression analysis if univariate analysis found significance of P < .15. Odds ratios (ORs) with respect to all variables included in multivariate analysis were determined. Preoperative baseline outcome scores were also correlated with future satisfaction with surgery by ROC/AUC analysis.
Results
Demographics
During the study period, 471 MATs were performed. Ninety-eight patients (20.7%) completed all questionnaires within the required time window at 1-year follow-up. The mean age of the cohort was 29.4 ± 9.0 years. There were 50 male and 48 female patients. Baseline preoperative PROM scores were collected and were equivalent to those of patients who were unable to complete their questionnaires within the allotted time window (Table 1). Concomitant procedures were performed in 82 of 98 patients, and several patients received combinations of ligamentous, realignment, and cartilage procedures (Table 2).
Concomitant Procedures Performed With Meniscal Allograft Transplantation a
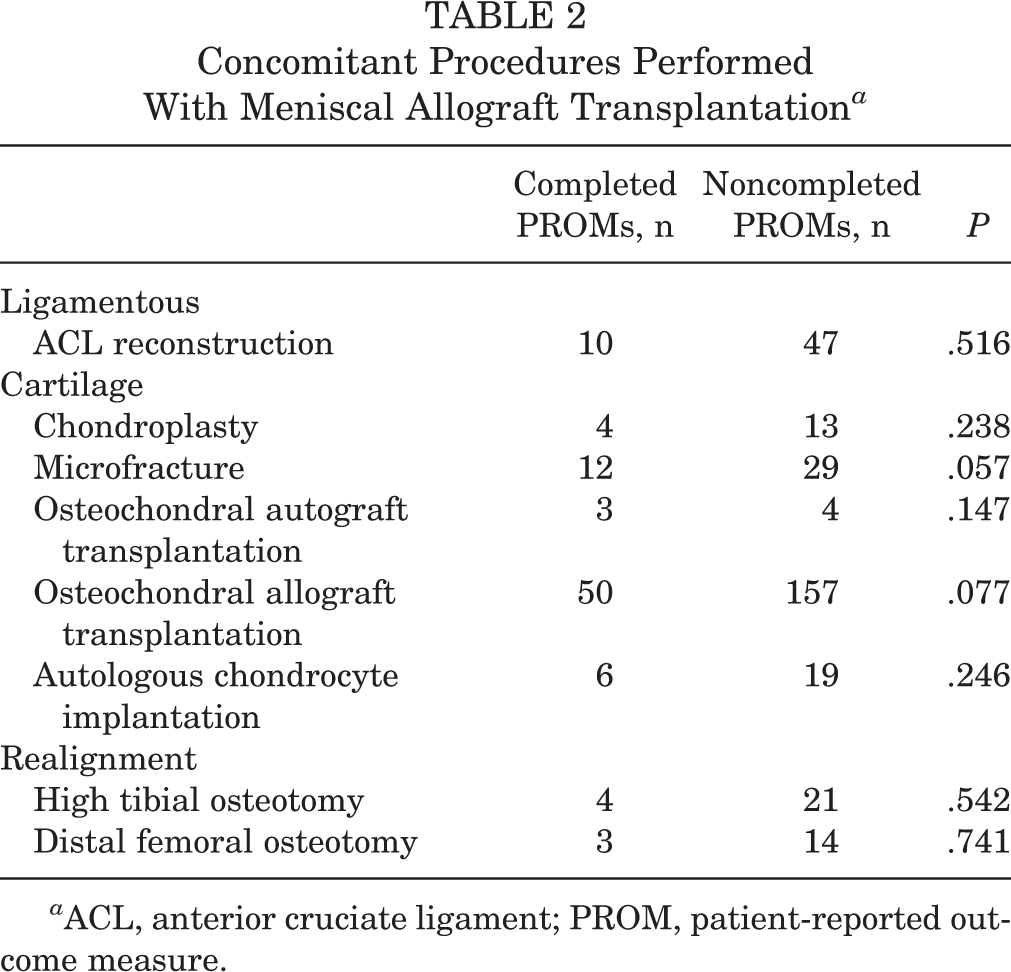
a ACL, anterior cruciate ligament; PROM, patient-reported outcome measure.
Calculating Clinically Significant Outcomes (MCID and PASS)
Of the 98 patients who completed the PROMs, 34 completed satisfaction questionnaires. The mean change in scores was 20.0 ± 19.7 for the IKDC, 20.3 ± 24.5 for the Lysholm score, 15.3 ± 19.8 for KOOS Pain, 13.6 ± 19.4 for KOOS Symptoms, 13.7 ± 19.0 for KOOS ADL, 18.5 ± 26.5 for KOOS Sport, and 16.0 ± 28.9 for KOOS QOL. From this, the MCID with the distribution-based methodology was established (Table 3). There were 28 patients satisfied with their surgery and 6 patients who were unsatisfied. There were statistically significant differences in postoperative outcome scores between satisfied and unsatisfied patients for the Lysholm score, IKDC, KOOS Pain, KOOS Symptoms, KOOS ADL, KOOS Sport, and KOOS QOL (P = .035, P = .006, P = .011, P = .005, P < .001, P = .007, and P = .015, respectively). ROC/AUC analysis was performed to determine the threshold postoperative score that best reflected satisfied patients. The Youden index was used to select the threshold score that maximized sensitivity and specificity (Table 4).
Distribution-Based MCID a

a ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; QOL, Quality of Life.
Anchor-Based PASS a
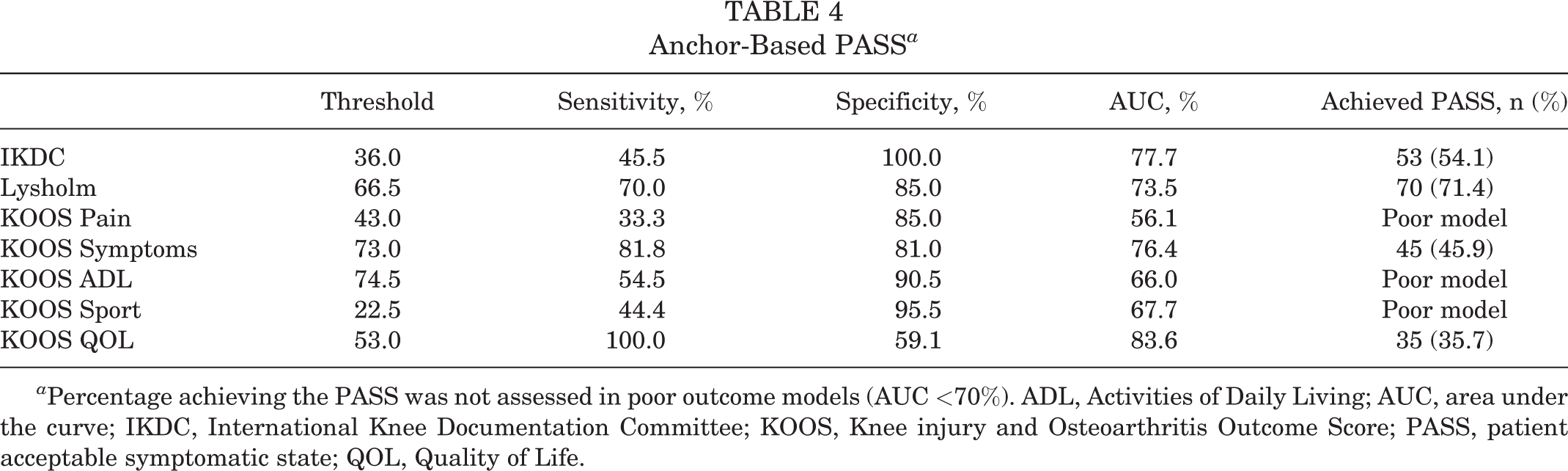
a Percentage achieving the PASS was not assessed in poor outcome models (AUC <70%). ADL, Activities of Daily Living; AUC, area under the curve; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PASS, patient acceptable symptomatic state; QOL, Quality of Life.
Variables Associated With Clinical Significance
Preoperative baseline scores were analyzed to determine if any preoperative score was associated with future satisfaction with surgery. Only the Short Form Physical Component Summary (SF PCS) was predictive of future satisfaction. Patients with SF PCS scores higher than 32.0 had a better likelihood of being satisfied after surgery than those with less than the score. Post hoc analysis demonstrated that patients who were satisfied had a mean SF PCS score of 12.1 ± 17.0 while those who were not satisfied had a mean SF PCS score of 1.5 ± 25.2 (Table 5).
Preoperative Scores Predictive of Satisfaction a
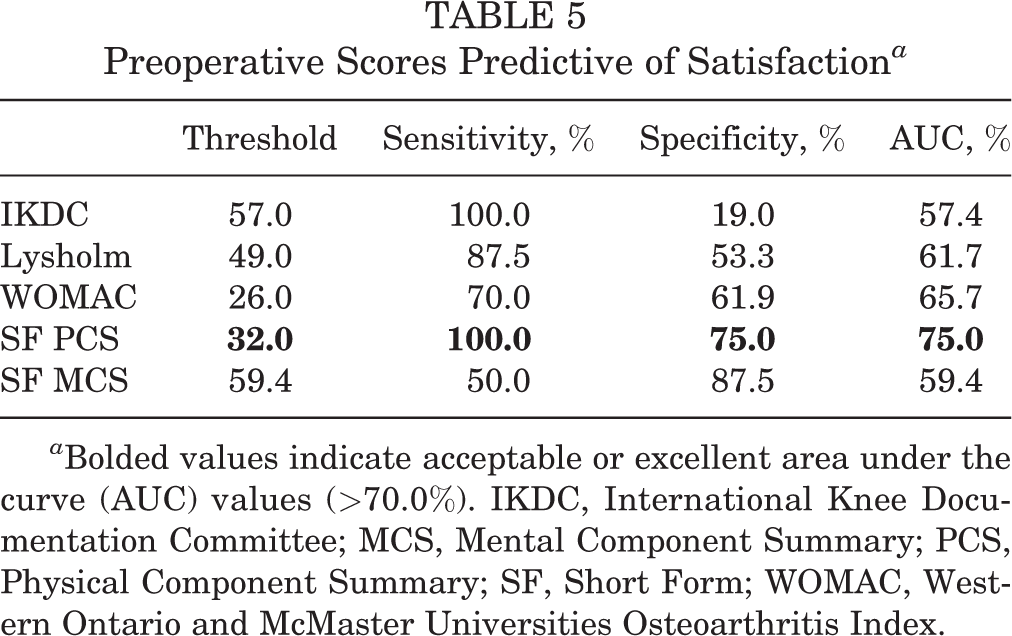
a Bolded values indicate acceptable or excellent area under the curve (AUC) values (>70.0%). IKDC, International Knee Documentation Committee; MCS, Mental Component Summary; PCS, Physical Component Summary; SF, Short Form; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Multivariate logistic regression was performed for all preoperative and intraoperative variables related to achieving the MCID. Achieving the MCID for the Lysholm score was only associated with reduced preoperative scores (OR, 0.956 [95% CI, 0.926-0.987]). A higher preoperative score (OR, 0.816 [95% CI, 0.666-0.990]) and workers’ compensation status (OR, 0.002 [95% CI, 0.000-0.765]) were associated with reduced odds of achieving the MCID for the IKDC. A higher preoperative score was associated with reduced odds of achieving the MCID for KOOS Pain (OR, 0.921 [95% CI, 0.874-0.970]), KOOS Symptoms (OR, 0.946 [95% CI, 0.905-0.988]), KOOS ADL (OR, 0.903 [95% CI, 0.843-0.966]), and KOOS QOL (OR, 0.925 [95% CI, 0.871-0.981]). Additionally, a history of meniscal debridement was associated with greater odds of achieving the MCID for KOOS QOL after MAT (OR, 9.871 [95% CI, 1.537-63.381]) (Table 6).
Logistic Regression of Variables Associated With Achieving the MCID a

a Bolded values indicate statistical significance upon multivariate regression (P < .05). ADL, Activities of Daily Living; BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; QOL, Quality of Life.
b No concomitant procedures with meniscal allograft transplantation.
c Concomitant chondroplasty, microfracture, autologous chondrocyte implantation, or osteochondral allograft transplantation.
Lower preoperative Lysholm scores had reduced odds of achieving the PASS for the Lysholm score (OR, 0.937 [95% CI, 0.884-0.994]). No variable was associated with achieving the PASS for the IKDC. Workers’ compensation status had reduced odds of achieving the PASS for KOOS Symptoms (OR, 0.088 [95% CI, 0.008-0.990]). A higher BMI indicated reduced odds of achieving the PASS for KOOS QOL (OR, 0.553 [95% CI, 0.348-0.880]) (Table 7). The remainder of the KOOS subscales did not accurately model patient satisfaction, and thus, multivariate regression was not performed.
Logistic Regression of Variables Associated With Achieving the PASS a

a Bolded values indicate statistical significance upon multivariate regression (P < .05). BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; N/A, not available; PASS, patient acceptable symptomatic state; QOL, Quality of Life.
b No concomitant procedures with meniscal allograft transplantation.
c Concomitant chondroplasty, microfracture, autologous chondrocyte implantation, or osteochondral allograft transplantation.
d Concomitant anterior cruciate ligament reconstruction.
Discussion
This study established values for the MCID and PASS for patients undergoing MAT with respect to the Lysholm score (12.3 and 66.5) and IKDC (9.9 and 36.0) as well as the KOOS Pain (9.9 and N/A), Symptoms (9.7 and 73.0), ADL (9.5 and N/A), Sport (13.3 and N/A ), and QOL (14.6 and 53.0) subscales, respectively. Workers’ compensation status was associated with failing to achieve the MCID for the IKDC, while workers’ compensation and higher BMI were both associated with failing to achieve the PASS for the KOOS subscales. Preoperative Lysholm (lower score associated with achieving the MCID and higher score associated with achieving the PASS), IKDC, and KOOS scores were predictive of achieving clinically significant outcomes, while a preoperative SF PCS score greater than 32.0 indicated a better likelihood of being satisfied after MAT. These results are important in helping surgeons counsel patients preoperatively about their likelihood of achieving clinically significant results after MAT.
Defining outcomes and success after MAT is particularly complex, as its benefit can be difficult to quantify and there is a lack of agreement on the most appropriate expected outcome. 39 While many studies have focused on graft survivorship using secondary surgery such as meniscectomy or conversion to total knee arthroplasty as clinical endpoints, data from long-term studies must be interpreted with caution, as techniques have evolved tremendously since the first MAT procedure performed. § Early studies published by Verdonk et al 44 involved an open technique detaching the collaterals and have been shown to be biomechanically inferior to current fixation methods by in vitro tibiofemoral joint contact pressures. 29 On the other hand, the current standard of care involves an arthroscopic-assisted technique with a variety of soft tissue and bony fixation options and a combination of all-inside and inside-out sutures to affix the meniscus to the periphery. 9 Our current understanding of survivorship, despite mixed techniques, is approximately 80% survivorship at 10 years and 30% to 50% at 20 years. ∥ Nevertheless, it is understood that MAT does not prevent the progression of osteoarthritis and will inevitably fail despite techniques.
The concept of quality “time gained” has thus surfaced as a surrogate outcome for success. 39 The majority of MAT clinical case series have categorically demonstrated strong improvements in function and quality of life via statistically significant changes in PROM scores. 3,20,21 However, only a minority of studies have addressed the concept of clinically significant outcomes and have used non–MAT-specific values in their analyses. Previous measures of knee function have considered clinical failure to be a postoperative Lysholm score less than 65 or the need for a revision procedure. 8,48 However, this cutoff was determined for all knee procedures and does not consider differences in abnormalities. Harris et al 16 used the MCID and minimal detectable change values of 11.5 for the IKDC and 5 to 12 for the KOOS, respectively, associated with general “knee injuries” and the minimal detectable change value of 8.9 for the Lysholm score in the setting of ACL reconstruction. These values are slightly different from the values calculated from our study, corroborating the notion that clinically significant outcomes such as the MCID are both diagnosis and intervention specific. 31,32 Additionally, our study was able to define other metrics of clinically significant outcomes, namely the PASS, to provide a spectrum of meaningful outcomes that may be used to gauge operative benefit after MAT.
We also found that lower preoperative PROM scores were associated with achieving the MCID, while higher preoperative SF PCS scores were associated with patient satisfaction. These results suggest that patients with lower preoperative function have more room to reach clinically meaningful improvement, which is similar to the majority of orthopaedic studies utilizing these clinically significant metrics. 10,11,18,22,31,32,34,46 On the other hand, higher preoperative physical function was the only metric associated with achieving satisfaction after surgery. This result suggests that patients must have a baseline level of function or physical well-being before undergoing MAT to achieve the PASS postoperatively.
The fact that patients insured under workers’ compensation had a lower probability of achieving the MCID is not surprising. Saltzman and colleagues 38 reported in a cohort of 40 patients undergoing combined ACL reconstruction and MAT that patients with workers’ compensation had a higher chance of graft failure. Other cartilage restoration procedures have also demonstrated inferior outcomes in patients involved with workers’ compensation. McCulloch et al 28 reported in a cohort of 25 consecutive patients undergoing fresh osteochondral allograft transplantation of the femoral condyle that patients insured under workers’ compensation had statistically significantly lower KOOS Sport scores at final follow-up compared with their non–workers’ compensation counterparts, despite similar baseline scores. 38 Our results demonstrate that these statistically inferior outcomes widely expressed in the literature are also clinically inferior based on their association with failure to achieve the MCID and PASS. While the exact cause to explain outcome differences in patients with workers’ compensation insurance claims remains unknown, other authors have suggested that perhaps the process of making a claim may be leading to worse outcomes or that these claims may be associated with other unidentified factors. 17 For example, secondary gain may be an important variable, although difficult to isolate. Although we have yet to isolate the exact underlying cause of worse outcomes for workers’ compensation patients undergoing MAT, it is important for patients and clinicians alike to be aware of these findings when making the decision about whether to pursue this procedure.
Interestingly, higher BMI decreased the likelihood of achieving the PASS for the KOOS QOL subscale. Intuitively, a higher BMI would place more stress across the joint, which may not be as well dissipated in the presence of meniscus transplantation. These patients may be more symptomatic and less satisfied after their MAT surgery. Nevertheless, there has been a dearth of literature to support the effects of higher BMI on outcomes after MAT, perhaps because the majority of prior investigations involving MAT use obesity as an exclusion criterion (although an exact BMI cutoff has not been proposed in the literature). Zaffagnini and colleagues 48 did not find a difference in survivorship of their MATs in patients with BMIs >25 kg/m2 versus <25 kg/m2 (designated as this was the mean of this population), although the BMI range in their study was relatively narrow (18.9-35.9 kg/m2 in 175 patients), making it difficult to determine a true relationship. In our study, the fact that only 1 KOOS subscale demonstrated significance in relation to BMI may be related to the indications of the senior author steering patients with elevated BMIs away from MAT. Nevertheless, this subtle result does provide some limited evidence to demonstrate that higher BMI is associated with clinically inferior outcomes.
Limitations
A significant limitation of this study is the possibility of selection bias, as only 21% of patients during the study’s time period were compliant with both preoperative and postoperative PROMs. However, the baseline demographics between compliant and noncompliant patients were equivalent, and responses were time specific (see Table 1). Compliance for the satisfaction questionnaire was even lower (7%) and may be further prone to selection bias. To this end, the calculated PASS was found to be equivalent to the baseline preoperative score. It is also important to note that preoperative PROM scores were generally low, which affected achievement of the MCID, even though this may be reflective of the population undergoing MAT. While the study did establish clinically significant outcomes, these outcomes were only demonstrated at short-term follow-up (1 year). The persistence of clinical improvement in the long term is unknown. Patients may start to experience a relapse of symptoms and worsening functional outcomes well before the need for subsequent procedures such as meniscectomy or arthroplasty. The incidence and timing of worsening outcomes or clinical failure of MAT are outside the scope of the present study.
Additionally, there was a wide range of concomitant procedures, and the resultant heterogeneity could certainly have influenced outcomes and calculated values. Graft failure has been previously associated with knee malalignment, chondral defects, and ligamentous instability. Concomitant procedures were performed to give the graft the best chance at succeeding in patients. Yet, isolated and combined procedures were still felt to be comparable because there was no change in the postoperative rehabilitation course, and a recent meta-analysis has demonstrated equivalence in outcomes between isolated MAT and that combined with other procedures. 20 Additional heterogeneity may arise because of the inclusion of both medial- and lateral-sided transplantation, although this was not found to influence outcomes on multivariate analysis. Because of the lengthy inclusion time from 1999 to 2017, improved surgeon experience and skill over time may also have biased the results. This time period was felt to be necessary because of the infrequency of this operative procedure. Further, bias was limited because of the consistent surgical technique from a single surgeon. Given the low number of concomitant procedures, subanalyses accounting for these variables could not be performed.
Conclusion
This study established the MCID and PASS for the Lysholm score, IKDC, and KOOS in patients undergoing MAT. Workers’ compensation and higher BMI were associated with failing to achieve clinically significant values. Lower preoperative Lysholm, IKDC, and KOOS scores were predictive of achieving the MCID, while higher preoperative SF PCS scores were associated with achieving satisfaction after MAT.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.Y. has received hospitality payments from Stryker, Organogenesis, Arthrex, Ceterix Orthopaedics, Aastrom Biosciences, and Smith & Nephew; receives research support from Arthrex and MedWest; is a consultant for Aastrom Biosciences; and has received educational support from Arthrex and Smith & Nephew. B.J.C. is a consultant for Arthrex, Geistlich Pharma, Smith & Nephew, Bioventus, Vericel, Zimmer Biomet, Anika Therapeutics, Pacira Pharmaceuticals, and Isto Technologies; receives royalties from Arthrex, DJO, and Encore Medical; is a paid speaker/presenter for Arthrex, LifeNet Health, Carticept Medical, and Pacira Pharmaceuticals; has received educational support from Arthrex and Pacira Pharmaceuticals; and has received hospitality payments from Arthrex, Geistlich Pharma, LifeNet Health, GE Healthcare, Vericel, Aesculap Biologics, DePuy Synthes, Genzyme, and Pacira Pharmaceuticals. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Rush University Medical Center Institutional Review Board.