
Abstract
Background:
Baseline concussion assessments are advocated to provide an objective preinjury point of comparison for determining the extent of postconcussion neurological deficits and to assist with return-to-activity decision making. Many factors, including testing environment, proctor availability, and testing group size, can influence test accuracy and validity; however, it is unknown how self-reported fatigue affects test scores.
Purpose:
To investigate the influence of self-reported fatigue and patient sex on baseline concussion assessment scores.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Participants included 494 healthy Division I college student-athletes (221 women, 273 men; mean ± SD age, 20.0 ± 1.3 years). During preseason baseline testing, participants were asked to rate their fatigue on a scale from 0 to 100 based on how they normally feel and function each day (0, completely exhausted; 100, completely awake and alert). Each participant then completed a multimodal baseline concussion assessment, including a graded symptom checklist (number of symptoms endorsed and total symptom severity score), Standardized Assessment of Concussion (SAC), Balance Error Scoring System (BESS), and CNS Vital Signs computerized neurocognitive testing. Multiple linear regressions tested whether self-reported fatigue and sex predicted baseline concussion examination scores.
Results:
Athletes with higher self-reported fatigue levels (ß = –0.014, P < .01) and female athletes (ß = –0.216, P < .01) reported more total symptoms. Being male (ß = 0.856, P < .01) increased the likelihood of endorsing zero symptoms versus any symptoms by a factor of 2.40. Women also had significantly higher SAC scores (ß = 0.569, P < .001), BESS scores (ß = –2.747, P < .001), and CNS Vital Signs summary scores (ß = 4.506, P < .001). SAC, BESS, and CNS Vital Signs scores were not predicted by fatigue level (P > .05).
Conclusion:
Female athletes and fatigued athletes endorsed more symptoms and higher symptom severity at baseline. Using total symptom endorsement and total symptom severity scores as part of the postinjury management is a common practice. The current data suggest that levels of reported exhaustion can influence concussion assessment scores meant to represent a healthy baseline and likely would interfere with postinjury assessment scores.
An estimated 3.8 million concussions occur in sports and recreational activities each year, with 6.2% at the collegiate level. 22,40 Current guidelines recommend a multifaceted approach to evaluating and managing concussion that includes assessing self-reported symptoms, neurocognitive function, and motor control. 5 Deficits in these outcomes may last longer than typical recovery times and may lead to late-life consequences, including increased risk for depression and cognitive decline. 15,16 Additionally, suffering 1 concussion greatly increases one’s risk of sustaining a subsequent injury. 17 The potential for these negative outcomes has led clinicians to a more conservative approach to treating and managing concussion, including annual baseline testing and gradual return-to-play protocols. Baseline testing provides an individualized standard to which athletes with concussion can be compared following injury. Many factors can affect baseline test validity, thereby complicating postinjury comparisons.
Testing environment and administration time can influence baseline concussion testing results. Current guidelines recommend that health care professionals avoid administering these baseline tests during unusual times of the day or when the athlete may be physically or mentally fatigued. 5 Athlete fatigue may negatively affect baseline concussion assessment results. Given the growing demands of training schedules, 33 athletes typically obtain less sleep than nonathletes, 23 which can lead to increases in negative moods, stress, and physical illness. 24 Shorter total sleep times have also been associated with higher levels of reported fatigue, 33 which may affect neurocognitive function, 9 postural control, 5 and symptom reporting. 20,24,29
In addition to fatigue affecting baseline concussion evaluation performance, there are known sex differences among baseline concussion assessments. Female athletes typically report more total symptoms and greater aggregate symptom severities than do males. 4,9,37,39 Sex differences also exist in Standardized Assessment of Concussion (SAC) scores, in that females tend to score better than males. 35 While some authors have found that females performed better than males on the Balance Error Scoring System (BESS), 35 others have not observed these sex differences. 19 In neurocognitive testing, sex differences in visual and verbal memory domains have been observed 9,10,12 but not in the overall summary score. 18
Although baseline concussion assessments can differ between sexes, it is unclear how fatigue influences these already-varied scores. Therefore, the purpose of this study was to determine the influence of self-reported fatigue and sex on baseline concussion assessments. We hypothesized that increased fatigue would result in poorer scores across all assessments when controlling for sex. Additionally, when controlling for fatigue, we expected women to endorse more symptoms, higher symptom severity, higher SAC scores, and higher visual and verbal memory scores in CNS Vital Signs, in line with previous findings. 4,9,11,12,35,37,39 We did not anticipate sex-based differences in the BESS score or the CNS Vital Signs summary score.
Methods
Participants included 494 collegiate athletes from a National Collegiate Athletic Association (NCAA) Division I institution (221 women, 273 men; mean ± SD age, 20.0 ± 1.3 years; age range, 18-24 years). Our sample included athletes practicing and competing in the following activities during the 2015-2016 academic seasons: baseball, cheer, crew, football, field hockey, fencing, gymnastics, softball, swimming and diving, track and field, volleyball, and wrestling, as well as men’s and women’s basketball, lacrosse, soccer, and tennis. Additional descriptive statistics are reported in Table 1. All study participants signed informed consent forms approved by the university’s institutional review board.
Demographic Variables and Baseline Concussion Evaluations a
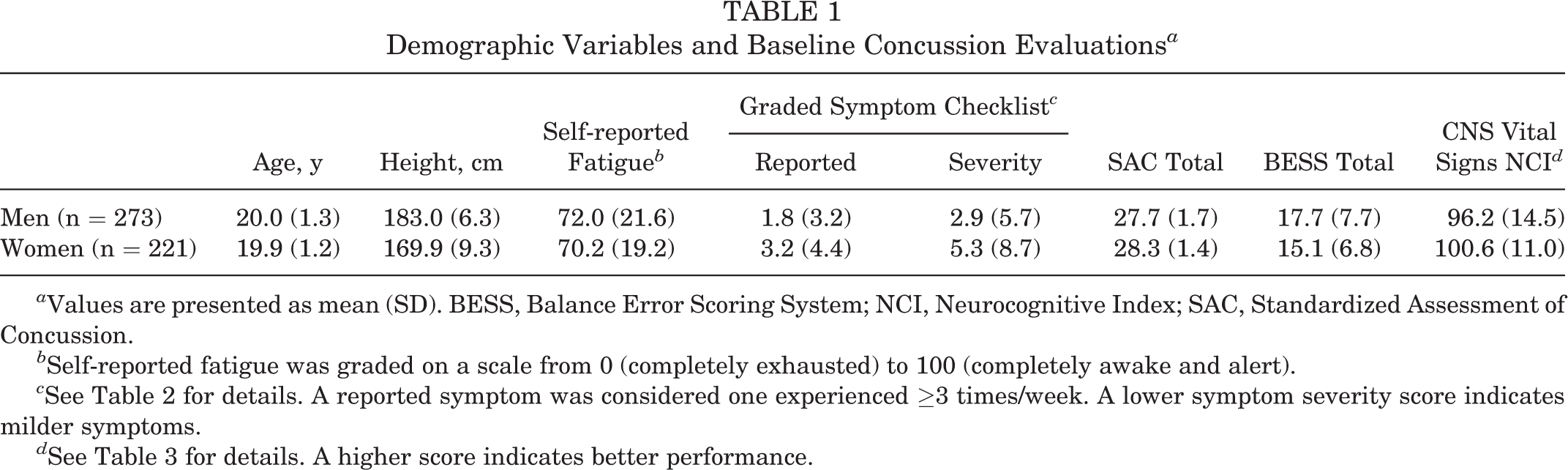
a Values are presented as mean (SD). BESS, Balance Error Scoring System; NCI, Neurocognitive Index; SAC, Standardized Assessment of Concussion.
b Self-reported fatigue was graded on a scale from 0 (completely exhausted) to 100 (completely awake and alert).
c See Table 2 for details. A reported symptom was considered one experienced ≥3 times/week. A lower symptom severity score indicates milder symptoms.
d See Table 3 for details. A higher score indicates better performance.
Instrumentation
Fatigue Scale
Participants rated their fatigue on a scale from 0 to 100 based on how they normally feel and function each day (0, completely exhausted; 100, completely awake and alert). Although the psychometric properties of single-item measures have been questioned, 21 we believe that such a measure is an acceptable metric in this instance, as single-item measures have convergent and discriminant validity when used to assess fatigue. 36
Graded Symptom Checklist
A 22-item symptom checklist was employed in this study (Table 2). 28 Participants were asked to rate their symptoms on a Likert scale ranging from 0 (not endorsing the symptom) to 1 (mild) to 6 (severe). At baseline, participants were asked to rate symptom severity only if they normally experienced the symptom ≥3 times per week for whatever reason. The total symptom frequency endorsed and the total symptom severity score (computed by adding all symptom severity ratings) were computed and retained for our analyses. A lower score indicated better outcomes for the graded symptom checklist (GSC).
Graded Symptom Checklist Symptoms a

a Participants were asked to rate the severity of any symptom experienced ≥3 times/week on a scale from 1 (mild) to 6 (severe). The total symptom severity score was computed by adding all symptom severity ratings.
Balance Error Scoring System
The BESS is a commonly employed postconcussion balance assessment protocol. It involves 3 stances (double-legged, single-legged, and tandem) and 2 surfaces (firm and foam). For balance in the single-legged stance, patients were instructed to stand as still as possible, with hands on iliac crests and eyes closed, while maintaining balance on the nondominant limb with the dominant limb in approximately 20° of hip flexion and 45° of knee flexion. For balance in the tandem stance, patients were instructed to stand heel-to-toe with the nondominant limb in back, hands on the iliac crests, and eyes closed. Leg dominance was defined as whichever leg the patient would use to kick a soccer ball for maximum distance. Participants were instructed to complete each of these six 20-second trials by remaining in the test position with their eyes closed to the best of their ability. Meanwhile, the clinician observed and documented the error frequency (to a maximum of 10 per trial). Errors could include the following: moving the hands off of the iliac crests; opening the eyes; stepping, stumbling, or falling out of test position; hip abduction or flexion >30°; lifting the forefoot or heel off the testing surface; or remaining out of the proper test position for >5 seconds. Moderate to high intraclass correlation coefficients for intertester reliability (0.57-0.96) have been noted in scoring BESS errors. 13,32 The BESS total error score was retained for our analyses. A lower score indicated better performance for the BESS.
Standardized Assessment of Concussion
The SAC is a brief cognitive screening tool designed to immediately assess concussion in athletes. The SAC was designed per the neuropsychological research literature addressing the domains of neurocognitive function most sensitive to the effects of mild brain injury and concussion (orientation, immediate recall, attention/concentration, and delayed recall) 7 and the tests best suited to measure those functions among patients with brain injury. 8 Extensive research 3,25 –27 demonstrated that the SAC is a sensitive and specific means to detect mild concussion and is a sensitive and specific measure of postconcussive recovery. The SAC total score was retained for our analyses, with a higher score indicating better performance.
CNS Vital Signs
Computerized neurocognitive testing was conducted with CNS Vital Signs 14 and took approximately 25 minutes to complete on desktop computers. Supervised testing occurred in a quiet, secluded room. Thorough descriptions of the neurocognitive domains, as well as all subtests used to calculate each domain standard score, are available in Table 3. Concussion baseline administrators instructed participants to read all directions carefully prior to each test module. A higher score indicated better performance for the CNS Vital Signs Neurocognitive Index (NCI) and each CNS Vital Signs domain standard score.
Domain Calculations and Descriptions for CNS Vital Signs

a These domain scores are averaged to derive the NCI (Neurocognitive Index) which was used for our analyses.
Procedures
Participants completed all assessments in a single session and were tested in small groups after providing informed consent. Test order was determined by scheduling matrices to maximize the number of participants whom we could evaluate in a given time frame and to minimize the amount of contact time with the student-athletes. All data were manually recorded (BESS and SAC) or collected digitally and exported (GSC and CNS Vital Signs) for analysis.
Statistical Analysis
Descriptive statistics were calculated for demographic variables, self-reported fatigue, and each baseline concussion assessment score. Self-reported fatigue was mean-centered prior to analysis. Due to the presence of zeros and extremely positively skewed distribution of GSC total scores, we used a zero-inflated Poisson regression model to test the effects of self-reported fatigue and sex on GSC total score. We similarly used a generalized linear model with a Poisson distribution to model effects of fatigue and sex on GSC severity to properly account for the measure’s extremely positively skewed distribution. Multiple linear regressions were used to determine the relationship of self-reported fatigue and sex on BESS total score, SAC total score, and CNS Vital Signs NCI. Alpha was set to 0.05 a priori.
Results
All analyzed data originated from 508 participants who completed baseline concussion assessments. Thirteen participants were removed for incomplete baseline assessments. One participant was removed because of an invalid fatigue rating of 0. The fatigue scale defines 0 as being completely exhausted, yet this participant reported being completely asymptomatic; therefore, we judged this response to be invalid because of either a misunderstanding of the question or a data entry error. The final sample used for all analyses comprised 494 participants.
There was a significant main effect of self-reported fatigue on GSC total score (ß = –0.014, P < .001) such that for every 1-point increase in the mean level of self-reported fatigue, the expected total symptom frequency endorsed would increase 1.01, when sex was held constant. Additionally, there was a significant main effect of sex on GSC total score (ß = –0.216, P = .002) such that women have a predicted increase in symptoms by a factor of 0.81, controlling for fatigue. Regarding the probability of a student-athlete reporting zero symptoms versus any symptoms, being a male increased the odds of endorsing zero symptoms by a factor of 2.40 (ß = 0.856, P < .001). Additionally, every 1-point decrease in the mean level of self-reported fatigue increased the odds of endorsing zero symptoms by a factor of 1 (ß = 0.033, P < .001).
There was a significant main effect of self-reported fatigue on GSC severity score (ß = –0.029, P < .001) such that for every 1-point increase in the mean level of self-reported fatigue, the expected severity score would increase by a factor of 0.97. Additionally, there was a main effect of sex on GSC severity score (ß = –0.491, P < .001) such that women would have higher expected severity scores by a factor of 0.61.
For the additional clinical outcomes, there were main effects of sex on SAC total scores (ß = 0.569, P < .001), BESS total score (ß = –2.747, P < .001), and CNS Vital Signs NCI (ß = 4.506, P < .001). Women had higher SAC total scores, fewer BESS errors, and higher CNS Vital Signs NCI. Specifically, women scored significantly higher than men on executive functioning (ß = 4.790, P < .001), processing speed (ß = 4.372, P < .001), cognitive functioning (ß = 5.017, P < .001), reaction time (ß = 5.342, P < .001), and verbal memory (ß = 5.240, P < .001), while men performed better on motor speed (ß = –2.586, P = .036); all analyses controlled for fatigue. When controlling for sex, self-reported fatigue did not predict SAC total scores (ß = 0.000, P = .911), BESS total score (ß = –0.032, P = .115), or CNS Vital Signs NCI (ß = 0.038, P = .302).
To compare our findings with those of the existing literature in this area, we performed a post hoc regression analysis to determine if participant height was a predictor for BESS performance. 19 Women in our sample were significantly shorter than men (t 492 = –16.84, P < .01), and height (F 2,491 = 23.56, P < .01) significantly predicted BESS total score when holding sex constant, such that for every 1-inch increase in height, BESS errors increased by 0.5.
Discussion
The most important finding in this study is the effect of self-reported fatigue and sex on GSC total symptom frequency and total symptom severity score. Critically, we found that men were significantly more likely than women to report zero symptoms on the GSC total score. The results of the current study suggest that baseline symptom assessments may vary widely according to sex and athlete fatigue. Although fatigue is a self-reported measure, it suggests that levels of reported exhaustion can influence concussion assessment scores meant to represent a healthy baseline and will likely interfere with postinjury assessment scores.
Sex-based differences in self-report variables are widely acknowledged in the health care literature. Notably, females tend to endorse not only more severe symptoms but a greater total number regarding physical 4,37,38 and psychological health. 2 Unsurprisingly, we found that women reported more symptoms and more severe symptoms on a concussion-specific symptom scale. Current literature theorizes that higher symptom endorsement by females may be due to several factors, including hormonal systems, 6 selective attention to bodily cues, and more willingness to endorse symptoms. 37 Additionally, males are less likely to disclose symptoms related to mental health, owing to self-stigmatization. 31
Increased self-reported fatigue was associated with greater GSC total symptom endorsement and greater GSC symptom severity score. As fatigue itself is a symptom, increased total symptom endorsement and symptom severity score were not surprising. However, as fatigue is only 1 symptom on the 22-item GSC, the increased scores cannot solely be explained by this. We used fatigue as a unidimensional construct via a single-item survey, as supported in previous literature. 36 Fatigue has been argued to be a multidimensional construct that encompasses mental and physical fatigue, 27 and it may be further divided into subsets of physical exertion, physical discomfort, lack of motivation, sleepiness, and lack of energy. 1 If fatigue is a multidimensional construct, this could contribute to the overall increase in GSC total symptom endorsement and GSC symptom severity score.
Additionally, sex was a significant predictor for SAC total score, BESS score, and CNS Vital Signs NCI. Women in our study performed better than men on the SAC. This finding is similar to that of Shehata et al, 34 who found that females scored higher on cognitive testing than males. While the evidence for sex differences on the BESS test is unclear, 34,35 we found that women scored significantly fewer errors than men. Iverson et al 19 looked at height as a potential predictor for BESS scores, as lower centers of gravity may contribute to better balance, but they found no relationship between height and BESS scores. Our results contrast those reported by Iverson et al, 19 as we found that every 1-inch increase in height was associated with a 0.5-error increase in BESS when controlling for sex.
Computerized neurocognitive assessments are currently being used in the concussion literature to examine overall cognitive function, with domains including visual and verbal memory, executive function, and processing speed. Our results indicated sex-based differences on several domains as well as on the summary NCI score. Current literature has found varying evidence for sex differences in the individual domains of CNS Vital Signs. Covassin et al 12 found that females performed significantly better on verbal memory and males performed significantly better on visual memory, while Iverson et al 18 found no significant sex differences in the domain standard scores. Our results may differ because of the use of a narrower sample age range or the use of a different computerized neurocognitive test. Although statistically significant, the explanatory power of self-reported fatigue and sex for SAC total score (R 2 = 0.038), BESS score (R 2 = 0.051), and CNS Vital Signs NCI (R 2 = 0.039) in the current study was small and therefore may not be a clinically meaningful result. Sex differences in general may not be as clinically relevant, owing to the use of the baseline test as an individualized standard with which to compare an injured athlete back with oneself, but they should be considered when interpreting baseline concussion assessment results.
The use of a single-item question to assess self-reported fatigue has varying evidence related to validity as compared with multiple-item measures of fatigue. Kim and Abraham 21 showed that a single-item measure of fatigue was not comparable with a more comprehensive measure that included multiple questions to address each specific domain, while van Hooff et al 36 showed a single-item measure to be a valid assessment. Despite conflicting evidence with single- versus multi-item questionnaires, single-item measures have been validated for unidimensional concepts such as fatigue. 36 Additionally, there are several logistic advantages to using single-item measures, including ease of administration, 30 cost-efficiency, and face validity. 36 Therefore, we determined that this measure was appropriate for the purpose of our study.
Conclusion
We found that fatigue and sex significantly predicted total baseline symptom endorsement and aggregate symptom severity and that men were more likely to endorse zero symptoms on GSC total score. We also found main effects for sex on all remaining assessment scores. As sex-based differences are evident in concussion literature, clinicians should be aware of these differences when evaluating athletes after an injury. Our results suggest that fatigue may be associated with a decrease in balance and neurocognitive performance, although these relationships may not be clinically meaningful. Future research should evaluate ideal times and environments for student-athletes to complete baseline concussion assessments to elicit the most valid and accurate baseline results free from fatigue.
Footnotes
Acknowledgment
The authors acknowledge the academic faculty, research staff, and trainees in the Matthew Gfeller Center at the University of North Carolina at Chapel Hill for their assistance with various aspects of this project.
The opinions, interpretations, conclusions, and recommendations in this article are those of the authors and are not necessarily endorsed by the Department of Defense (Defense Health Program funds).
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was funded with support from the Grand Alliance Concussion Assessment, Research, and Education Consortium, funded in part by the National Collegiate Athletic Association and the Department of Defense. The US Army Medical Research Acquisition Activity is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Psychological Health and Traumatic Brain Injury Program (award NO W81XWH-14-2-0151). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of North Carolina at Chapel Hill Office of Human Research Ethics.