
Abstract
Background:
Shoulder arthroscopy is a commonly performed, critical component of orthopaedic residency training. However, it is unclear whether there are additional risks to patients in cases associated with resident involvement.
Purpose:
To compare shoulder arthroscopy cases with and without resident involvement via a large, prospectively maintained national surgical registry to characterize perioperative risks.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The prospectively maintained American College of Surgeons National Surgical Quality Improvement Program registry was queried to identify patients who underwent 1 of 12 shoulder arthroscopy procedures from 2005 through 2012. Multivariate Poisson regression with robust error variance was used to compare the rates of postoperative adverse events and readmission within 30 days between cases with and without resident involvement. Multivariate linear regression was used to compare operative time between cohorts.
Results:
A total of 15,774 patients with shoulder arthroscopy were included in the study, and 12.3% of these had a resident involved with the case. The overall rate of adverse events was 1.09%. On multivariate analysis, resident involvement was not associated with increased rates of any aggregate or individual adverse event. There was also no association between resident involvement and risk of readmission within 30 days. Resident involvement was not associated with any difference in operative time (P = .219).
Conclusion:
Resident involvement in shoulder arthroscopy was not associated with increased risk of adverse events, increased operative time, or readmission within 30 days. The results of this study suggest that resident involvement in shoulder arthroscopy cases is a safe method for trainees to learn these procedures.
Keywords
Shoulder arthroscopy is one of the most commonly performed orthopaedic interventions, with rates increasing significantly since the early 1980s as many formerly open procedures are transitioning toward less invasive means. 21,28 It is the second-most common procedure performed by candidates taking the part II examination of the orthopaedic boards. 10 In addition to the frequency in which it is performed, shoulder arthroscopy is well tolerated by most patients, with an overall low complication rate at around 1.0% by some reports. 26 With these factors in mind, the Accreditation Council for Graduate Medical Education has included shoulder arthroscopy as one of the core competency procedures for orthopaedic residents in training. 7
Surgeons involved with resident trainees are tasked with balancing often-complex patient care with the mission of teaching operative skills as residents try to become competent orthopaedic surgeons. The pressures of operative efficiency, cost-efficacy, and minimization of risks to patients can make this role as a resident educator particularly demanding and concerning to some patients and practitioners alike. To better assess and understand the impact of resident involvement on intra- and postoperative morbidity and mortality, several recently published studies have utilized large public databases to compare complications based on resident participation in general orthopaedic surgical procedures, spinal surgery, and joint arthroplasty. 8,13,14,18,24
Currently, no similar large database studies exist that examine the effect of resident involvement exclusively for shoulder arthroscopy in terms of intra- and postoperative variables. The purpose of the current study was to use the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to compare perioperative risks in shoulder arthroscopy cases with and without resident involvement. Our hypothesis was that operative time, adverse events, and readmissions would not significantly differ in shoulder arthroscopy cases based on the inclusion of a resident orthopaedic surgeon.
Methods
Data Source
The ACS-NSQIP database, used for this study, collects data including demographics, comorbidities, operative characteristics, and postoperative complications from over 300 hospitals. The full methodology of the data collection process used by the ACS-NSQIP is described elsewhere. 1 Briefly, clinical data were collected from patients who were identified prospectively and randomly sampled at eligible hospitals. Patients were evaluated postoperatively for 30 days, and adverse events and readmission events were collected, including after the patient was discharged from the hospital.
Data Collection
Current Procedural Terminology codes 29806, 29807, 29819, 29820, 29821, 29822, 29823, 29824, 29825, 29826, 29827, and 29828 were used to identify patients in the ACS-NSQIP database who underwent arthroscopic shoulder surgery from 2005 through 2012. These codes were based on the precedent of previous studies of shoulder arthroscopy in the ACS-NSQIP data set. 19 Patients with mini-open or open shoulder procedures were excluded. Patients with missing perioperative data or those who underwent nonelective surgery were also excluded from this study.
The ACS-NSQIP database includes sex, age, height, and weight. Body mass index was calculated from each patient’s height and weight. History of smoking was defined as the use of cigarettes within the past year. Hypertension was defined as a chart diagnosis of hypertension with the patient currently taking antihypertensive medication. History of diabetes is recorded as 1 of 3 groups in the database: insulin-dependent diabetes mellitus, non–insulin dependent diabetes mellitus, or no diabetes. American Society of Anesthesiologists class ≥3 corresponds to severe systemic disease. History of chronic obstructive pulmonary disease, congestive heart failure, and the number of operative levels were also available in the database.
The ACS-NSQIP includes a variable in each surgical case specifying whether a resident was scrubbed. This variable was used to determine resident involvement for the purposes of this study. Notably, the database does not indicate the specific role of a resident during the surgical procedure but rather specifies if a resident was scrubbed and present as an assistant in some capacity during the procedure.
Outcomes
The ACS-NSQIP records intra- and postoperative data in a standardized fashion, including operative time, the occurrence of postoperative adverse events within 30 days, and readmission within 30 days. 1
Operative time was the number of minutes from the opening incision to the end of wound closure. A serious adverse event was defined as the occurrence of any of the following: death, coma >24 hours, ventilator >48 hours, unplanned intubation, stroke/cerebrovascular accident, thromboembolic event (deep venous thrombosis or pulmonary embolism), cardiac arrest, myocardial infarction, acute renal failure, sepsis, septic shock, return to the operating room, deep surgical site infection, or organ/space infection. A minor adverse event was defined as superficial surgical site infection, urinary tract infection, pneumonia, progressive renal insufficiency, or wound dehiscence. Any adverse event was defined as the occurrence of any serious adverse event or minor adverse event. Groups were compared in terms of any adverse event, serious adverse events, minor adverse events, and individual adverse events.
Readmission was defined as when a patient had an unplanned hospital admission to the index facility or another facility after the initial postoperative discharge. As the ACS-NSQIP began collecting readmission data beginning in 2011, only patients who underwent surgery from 2011 and 2012 were included in the readmission analysis.
Analysis
Statistical analyses were conducted with Stata (v 13.1; StataCorp LP). Chi-square analysis was used to compare all demographic and comorbidity variables between procedures with and without resident involvement. Operative time, a continuous variable, was compared between groups with bivariate and multivariate linear regression to control for patient characteristics. Adverse events and readmission were compared between groups with bivariate and multivariate Poisson regression with robust error variance and are reported in terms of relative risk. 12,22 Bivariate analysis was incorporated to determine if associations were present without controlling for baseline differences in resident versus no-resident cases and not to identify significant variables to include in a multivariate analysis. Given multiple statistical comparisons, a Bonferroni correction was used for the results of bivariate and multivariate analyses, yielding a cutoff for statistical significance at P < .004.
Results
A total of 15,774 patients with shoulder arthroscopy were included in the study, and 12.3% of these had a resident involved with the case (Table 1). A comparison of patient demographics and comorbidities between cases with and without resident involvement yielded no statistically significant differences between groups. The most common procedure was rotator cuff repair (36.5%), followed by subacromial decompression (27.5%) and SLAP (superior labrum anterior and posterior) repair (8.9%) (Table 2).
Comparison of Patient Characteristics for Shoulder Arthroscopy Cases With and Without a Resident Present a

a ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease.
b Statistical significance was set at P < .05.
Procedure Type a

a CPT, Current Procedural Terminology; SLAP, superior labrum anterior and posterior.
The overall rate of adverse events was 1.09% (Table 3). The most common adverse event was a return to the operating room (0.33%), followed by surgical site infection (0.20%). Among all patients with shoulder arthroscopy, 0.89% were readmitted within 30 days. On multivariate analysis (Table 4), resident involvement was not associated with increased rates of any aggregate or individual adverse event. There was also no association between resident involvement with a case and risk of 30-day readmission. Resident involvement was not associated with any difference in operative time (P = .219) (Table 5).
Resident Involvement and 30-Day Adverse Events and Readmission After Shoulder Arthroscopy a

a CPR, cardiopulmonary resuscitation; DVT, deep vein thrombosis; PE, pulmonary embolism.
Association of Resident Involvement With 30-Day Adverse Events and Readmission After Shoulder Arthroscopy a
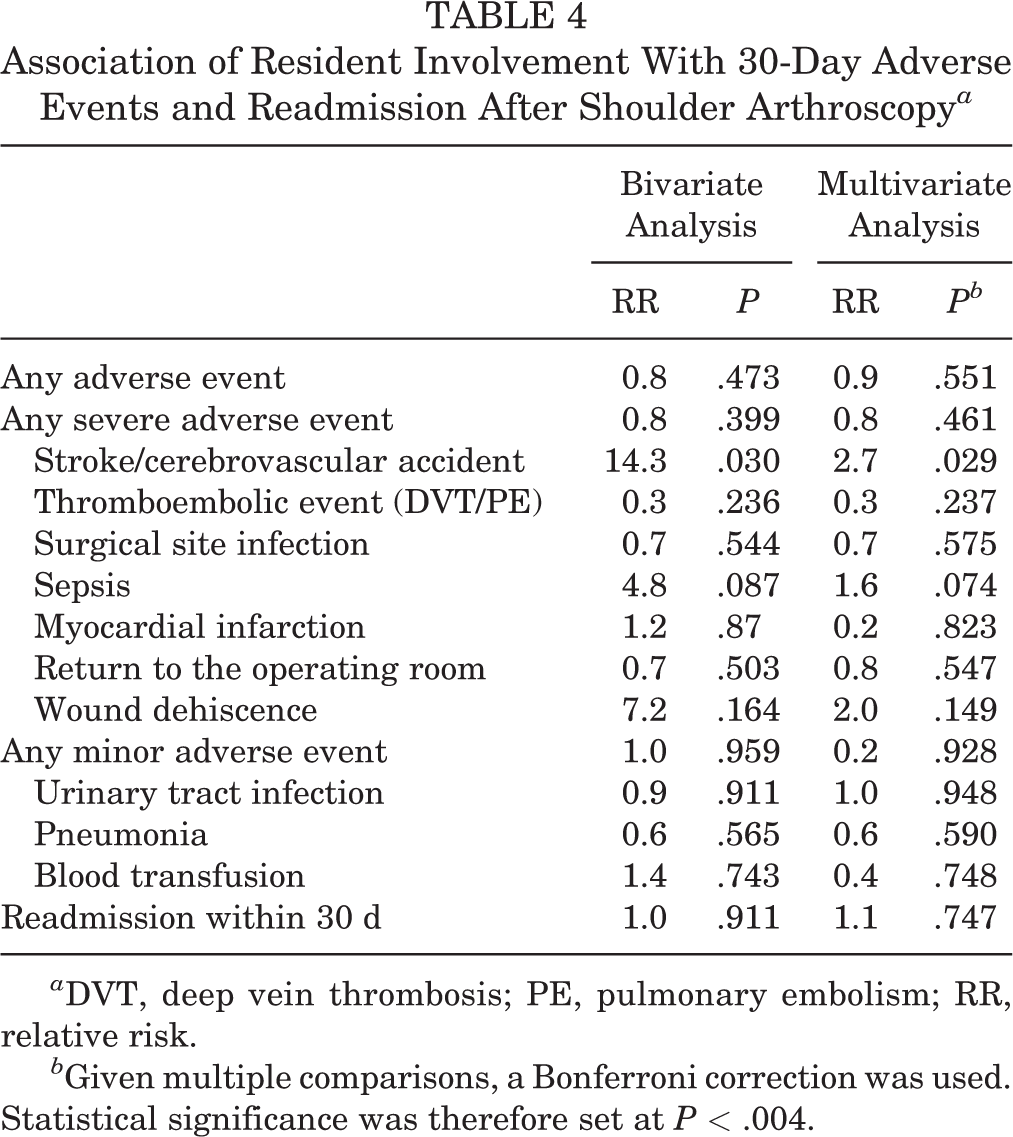
a DVT, deep vein thrombosis; PE, pulmonary embolism; RR, relative risk.
b Given multiple comparisons, a Bonferroni correction was used. Statistical significance was therefore set at P < .004.
Association of Resident Involvement With Operative Time

a Statistical significance was set at P < .002.
Discussion
The results of this study with the ACS-NSQIP database suggest that resident involvement in shoulder arthroscopy procedures does not significantly alter operative times, short-term adverse events, or readmission rates. In fact, in this large national database study of more than 15,000 shoulder arthroscopy procedures, resident involvement altered average operative time by no more than 1 minute. In terms of adverse events and readmissions, it is not unexpected that the overall rates of such occurrences were low (1.09% and 0.89%, respectively) given the safety profile of shoulder arthroscopy in general. Resident involvement did not correlate with any adverse outcome measure or the need for readmission. Furthermore, when we specifically examined wound dehiscence, surgical site infection, and return to the operating room (3 adverse event categories often perceived to be related to trainee involvement), we found no significant correlation between resident involvement and the occurrence of these events.
Attending-level surgeons are often tasked with balancing the delivery of safe and effective patient care with the expectation of hands-on resident education. 2,7,16 This fine balance of care versus education is complicated by additional external pressures from the health care system as well as from the patient and patient’s family. 7 There is increasing pressure from hospital administration and the health care system to increase productivity while limiting cost; at the same time, patients and their families are increasingly aware of trainee involvement. One solution to assuage some of these pressures has been an increasing emphasis on resident education through arthroscopic simulation and laboratory practice prior to hands-on intraoperative education. 20,27 In separate studies, Martin et al 20 and Waterman et al 27 implemented shoulder simulators to demonstrate proficiency and safety improvements in shoulder arthroscopy. Nonetheless, graduated responsibility must be granted, and there is no substitute for intraoperative decision making to train the next generation of safe and effective surgeons. Therefore, it is important to illustrate to surgeons, health care administrators, and patients alike that resident involvement in the operating room for shoulder arthroscopic procedures is cost neutral and safe.
There is conflicting evidence in the orthopaedic literature on the degree to which resident involvement affects operating room time. Green et al 11 reported on the sources of variation in operating room time for rotator cuff surgery and found that resident involvement, surprisingly, decreased surgical times. The authors reasoned that resident familiarity with the procedure and the routine nature of rotator cuff repairs were responsible for this finding. 11 It is possible that attending surgeon cases that are performed without residents are often done without assistance or with the assistance of a physician assistant or other first-assist personnel. It may also be that surgeons associated with resident training programs have more focused shoulder practices and are therefore more efficient at performing cuff repairs. Other studies of operative times in orthopaedic surgical procedures have not reproduced these results. Farnworth et al 9 reported that cases of anterior cruciate ligament reconstruction where a resident was involved were >40 minutes longer than cases with an attending surgeon alone, thereby contributing to a significantly increased cost burden. The evidence in nonorthopaedic surgical procedures is similarly conflicting. Bridges and Diamond 5 noted that in general surgery residency training programs, there were 46 case categories where resident operative times were longer than faculty times and 16 categories where resident times were shorter. In this context, it is unclear what factors may be contributing to the present study’s inability to detect a difference in operating room time.
Prior studies have utilized the ACS-NSQIP database to investigate the impact of resident involvement on adverse events and readmissions following orthopaedic surgery 6,8,14,17,18,24 ; however, these studies have largely been focused on spine surgery 8,17,18 and total joint arthroplasty. 6,14 The results of these studies have thus far been mixed in terms of the effects of resident involvement on outcomes and readmissions. Kothari et al 18 used the database to evaluate the effects of resident involvement on deformity correction with spinal fusion. These authors found that resident involvement was an independent predictor of overall morbidity but not mortality. In the arthroplasty literature, Haughom et al 14 demonstrated that resident involvement did not increase 30-day complication rates following primary total hip arthroplasty. Similarly, resident involvement in shoulder arthroplasty did not affect 30-day complications among the over 1300 patients analyzed from the ACS-NSQIP database. 6 Last, Edelstein et al 8 evaluated more than 30,000 orthopaedic procedures within the ACS-NSQIP database, which included procedures of various levels of adverse event risk, and they found that resident involvement was associated with a lower risk of perioperative complications and mortality.
These mixed results in the context of known varying complication rates for orthopaedic procedures suggest that further study of the impact of resident involvement must be performed on a surgical technique basis rather than by grouping multiple techniques. The current study examined shoulder arthroscopy and found that operative times, adverse event profiles, and readmission rates were not significantly altered with the involvement of orthopaedic trainees. These findings are particularly meaningful for all stakeholders, as cost neutrality is maintained without compromising patient outcomes, while patients and their families are reassured that they are receiving low-risk quality care. The results also suggest that residents are not being asked to perform surgical skills beyond their levels of competence. Most important, a teaching environment provides comprehensive surgical assistance and generally promotes up-to-date and informed decision making that is evidence based, which can sometimes become stagnant outside a teaching environment, where some of the more difficult medical problems are managed.
While our study was highly powered with a large sample size, the results must be interpreted with caution. Given the safety profile of arthroscopic shoulder procedures, it may be difficult to determine if resident involvement alone will lead to measurably increased 30-day complication rates. With limited arthroscopic portals and well-vascularized tissue flaps and in an outpatient surgical setting, the morbidity of shoulder arthroscopy is uniquely attributable to the global health status of the patient and surgical duration. These themes were consistently conveyed in prior series of complication rates based on ACS-NSQIP data. 3,4,15,23,25 However, the most common complications seen in shoulder arthroscopy (eg, recurrent cuff tears, recurrent instability, continued pain, stiffness) are not captured by the ACS-NSQIP database.
The current study is not without limitations. The ACS-NSQIP database is designed to evaluate 30-day adverse events and readmissions; therefore, longer-term complications and the role of resident involvement on those complications could not be studied. While unplanned return to the operating room was included as an adverse event, the ACS-NSQIP is unable to provide the reason for such a return. Similarly, the ACS-NSQIP is unable to conclusively capture readmissions (eg, deep vein thrombosis, poor pain control) at another facility. Furthermore, there are possible adverse events or complications that might not be captured by ACS-NSQIP data.
Ostensibly, resident involvement or a larger role in surgery could contribute to undetected sources of postoperative morbidity, such as persistent pain, worse patient-reported function, iatrogenic soft tissue damage (cartilage, tendon, labrum), or missed pathology. This would presumably correlate with patient-reported outcome measures at longer-term follow-up, which are, unfortunately, not reported by the ACS-NSQIP database. In addition, the ACS-NSQIP denotes only the presence or absence of a resident in each case, and there are no data on the degree of involvement, which can vary considerably by institution, complexity of the surgical procedure, and physician and family preferences. Resident involvement may range from acting as the primary surgeon in a procedure to simply being present in a case for observation and/or assisting with visualization.
It is important to remember that residents’ acquisition of surgical skills is needed for the care of future generations of orthopaedic patients. Still, despite the large sample size reported in the present study, it may be underpowered for certain outcomes, given the generally low rate of adverse events associated with shoulder arthroscopy. Nonetheless, we believe that the large sample, rigorous data curation, prospective data collection, and availability of resident involvement make the ACS-NSQIP data set uniquely suited to answer the study question. Last, there is inherent bias in the shoulder arthroscopy procedures involving a resident, as these cases are presumptively performed largely at academic centers, while those cases without a resident are largely performed at private centers. Currently, there is no way to control for the difference in surgical center, attending-level surgeon case volume or skill level, fellow trainee involvement, or trainee training level within the ACS-NSQIP system—all factors that may influence the data analysis.
Conclusion
Overall, resident involvement in shoulder arthroscopy was associated with no increase in operative time, increase risk of adverse events, or increase rate of readmission within 30 days. The results of this study suggest that resident involvement in shoulder arthroscopy cases is a safe method for trainees to learn these procedures.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.B. has received hospitality payments from Smith & Nephew. A.A.R. receives royalties from, is a consultant for, and has received hospitality payments from Arthrex. N.N.V. is a paid speaker/presenter for Pacira Pharmaceuticals and receives royalties from, is a consultant for, and receives hospitality payments from Smith & Nephew. B.J.C. receives research support from Aesculap/B. Braun, Arthrex, Geistlich, Medipost, the National Institutes of Health (National Institute of Arthritis and Musculoskeletal and Skin Diseases and National Institute of Child Health and Human Development), Norvartis, Sanofi-Aventis, and Zimmer; is a consultant for Anika Therapeutic, Arthrex, Bioventus, Flexion, Genzyme, Regentis, Pacira Pharmaceuticals, Smith & Nephew, Zimmer, and Vericel; has stock/stock options in Aqua Boom, Biomerix, Giteliscope, Ossio, and Regentis; receives royalties from Arthrex, DJ Orthopaedics, Encore Medical, and Saunders/Mosby-Elsevier; is a paid speaker/presenter for Carticept and Pacira Pharmaceuticals; has received hospitality payments from DePuy, Genzyme, and Lifenet Health; and receives other financial/material support including compensation for travel and lodging or food/beverages from Athletico, JRF Ortho, Smith & Nephew, and Tornier. A.E.W. receives royalties from Smith & Nephew; receives educational support from Arthrex; is a consultant for Smith & Nephew; and receives hospitality payments from Smith & Nephew, Arthrex, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.