
Abstract
Background:
Regional nerve blocks are commonly used to manage postoperative pain after arthroscopic shoulder procedures. The interscalene brachial plexus block (ISB) is commonly used; however, because of the reported side effects of ISB, the use of a suprascapular nerve block (SSNB) has been described as an alternative strategy with fewer reported side effects.
Purpose:
To examine the efficacy of SSNB for pain control after shoulder arthroscopy compared with ISB as well as anesthesia without a nerve block.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
Three databases (PubMed, MEDLINE, and EMBASE) were searched on April 20, 2018, to systematically identify and screen the literature for randomized controlled trials (RCTs). A meta-analysis of standard mean differences (SMDs) was performed to pool the estimated effects of the nerve blocks.
Results:
The search identified 14 RCTs that included 1382 patients, with a mean age of 54 years (SD, 13 years). The mean follow-up time was 3 days (range, 24 hours to 6 weeks). Postoperative pain control was significantly more effective in the SSNB groups compared with the control groups within 1 hour (SMD, –0.76; 95% CI, –1.45 to –0.07; P = .03) and 4 to 6 hours (SMD, –0.81; 95% CI, –1.53 to –0.09; P = .03) postoperatively. However, pain control was significantly less effective in the SSNB groups compared with ISB within 1 hour (SMD, 0.87; 95% CI, 0.28 to 1.46; P = .004). No major complications were noted in the SSNB groups, and minor complications such as hoarseness and prolonged motor block were significantly less common for SSNB compared with ISB.
Conclusion:
Although not more efficacious than ISB in terms of pain control for patients undergoing shoulder arthroscopy, SSNB provides significantly improved pain control in comparison with analgesia without a nerve block. Moreover, few major and minor complications are associated with SSNB reported across the literature.
Shoulder arthroscopy is a commonly performed procedure that many providers prefer to open approaches because it involves less soft tissue dissection, shorter duration of hospital stay, and improved cosmesis. However, arthroscopic surgery of the shoulder can be associated with moderate to severe early postoperative pain that can interfere with recovery and rehabilitation. 9 Management of this pain is often accomplished by use of opioids; however, their use is often associated with side effects such as nausea, vomiting, respiratory depression, dysphoria, and hormonal effects including the levels of luteinizing hormone and testosterone. 32,45 Controlling postoperative pain while minimizing opioid administration is particularly important, because poor pain control is thought to be responsible for more than 60% of unplanned or prolonged hospitalizations. Additionally, achieving good pain control is an important factor in determining patient-reported postoperative satisfaction. 5
To manage postoperative pain, regional nerve blocks are commonly used. Among the various types of nerve blocks, the interscalene brachial plexus block (ISB) is considered the gold standard, as it has consistently been shown to significantly reduce postoperative pain. 18,29 Moreover, ISB can be used to provide surgical anesthesia, rather than just the postoperative anesthesia than is provided by other types of blocks. However, complications ranging from the serious (such as accidental epidural anesthesia, vertebral artery injection, paralysis of the phrenic nerve, pneumothorax, and brachial plexus injury) 26 to the unpleasant (such as extended motor block after the procedure) have been reported following the use of ISB. 11,31 Furthermore, ISB has relative contraindications; for example, it is contraindicated in patients with severe chronic obstructive pulmonary disease because of phrenic nerve issues. 11 Because of these issues with ISB, the use of a suprascapular nerve block (SSNB) has been described as an alternative strategy with fewer reported side effects. The suprascapular nerve is thought to innervate approximately 70% of the shoulder joint, capsule, subacromial space, acromioclavicular joint, and coracoacromial ligament, with the remaining 30% thought to be innervated by the lateral pectoral and axillary nerves. 10
The purpose of this systematic review and meta-analysis was to examine the efficacy of SSNB for analgesia outcomes after shoulder arthroscopy in adult patients and to identify the complication rate from such blocks. Secondarily, the study assessed the efficacy of SSNB compared with ISB and non–nerve block controls.
Methods
Search Strategy
The PubMed (MEDLINE), Ovid (MEDLINE), and EMBASE databases were searched for literature addressing the use of SSNB for shoulder arthroscopy from database inception until April 20, 2018. The search terms “nerve block,” “regional anesthesia,” “regional block,” “suprascapular,” “shoulder,” and “arthroscopy” were used (Appendix Table A1).
Study Screening
Two reviewers (J.K., M.M.) independently screened the titles, abstracts, and full-text version of the articles. Any disagreements were discussed between reviewers and the senior author (O.R.A.) to determine study inclusion when necessary. The references of the included studies were then screened for additional articles that may have eluded the initial search strategy.
Assessment of Study Eligibility
The research question and eligibility criteria were determined a priori. The inclusion criteria included therapeutic studies written in English, studies evaluating live human participants, studies evaluating the use of SSNB (either alone or in combination with an axillary nerve block), and randomized controlled trials (RCTs) that reported any outcomes, including pain, opioid consumption, length of hospital stay, and cost. Commentaries, cadaveric studies, animal studies, conference papers, book chapters, review articles, and technical reports were excluded.
Data Abstraction
Two reviewers collected data in duplicate and recorded them in a Microsoft Excel spreadsheet (version 2007). Data regarding year of publication, author, location of study, procedures undergone by the patients, type of block used, study design, age, sex, sample size, pain scores, opioid consumption (expressed as morphine equivalents), side effects and complications (nausea, pneumothorax, prolonged motor block, phrenic nerve palsy, and hoarse voice), patient satisfaction and hospital length of stay, and level of evidence were recorded. An attempt was made to contact the authors of any study whose article contained insufficient data.
Quality Assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was used to assess the methodological quality of the included studies. 12 The GRADE method begins by initially assigning RCTs as high-quality evidence. Thereafter, the studies are evaluated for 5 factors related to the quality of evidence: risk of bias, inconsistency, indirectness, imprecision, and publication bias. 3,17 Risk of bias assesses the limitations of the included studies on the basis of randomization, allocation concealment, blinding, incomplete outcome reporting, selective reporting, and other biases. 17 Inconsistency refers to the level of similarity of results throughout the included studies by assessing variation in the intervention groups and the point estimates and, if meta-analyses are performed, the amount of overlap in CIs, the magnitude of I 2, and statistical tests for heterogeneity. 13 Indirectness assesses the relevance of study outcomes and the applicability of the studies to the interventions and populations of interest. 14 Imprecision assesses the sample size of the analysis as well as certainty of the effect estimate. 15 Publication bias refers to the cumulative assessment of the direction of findings in each study, as well as funding sources, funnel plot analysis for each outcome, and study sample sizes. 16 Ultimately, the final overall body of literature on the topic is scored and reported as high, moderate, low, or very low quality, and this score relates to the overall confidence in the pooled effect estimate.
Assessment of Agreement
To assess the interreviewer agreement, a kappa (κ) statistic was calculated for the title, abstract, and full-text screening stages. Agreement was categorized a priori as follows: κ of ≥0.61 was considered substantial agreement; 0.21 to 0.60, moderate agreement; and ≤0.20, slight agreement. 28
Statistical Analysis
Descriptive statistics including means, proportions, ranges, 95% CIs, standard deviations, and κ values were calculated by use of Minitab statistical software (version 17). Given the nonuniform nature of reporting for opioid consumption, length of stay, and patient satisfaction in the studies included in this systematic review, the results for these secondary outcomes are presented as a narrative summary.
A meta-analysis was conducted evaluating postoperative pain in order to compare the use of SSNB with ISB and with controls. A decision was made a priori that a minimum of 3 trials would be needed for any outcome to be pooled. Standardized mean differences (SMDs) were used to account for differences in pain outcome scales. Pooled analyses were performed by use of the Review Manager (RevMan) software 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, 2012). P < .05 was considered to be significant. The I 2 test was used to assess heterogeneity across the reported results of the included studies. The proportions were then combined using a random effects model (I 2 < 30%, which was considered as low statistical heterogeneity). 33 A sensitivity analysis was conducted to account for differences with respect to block technique, specifically to account for studies that used a combination of axillary nerve blocks with SSNB.
Results
Search Strategy
The initial search of the 3 databases resulted in 1564 total studies. Of these, 569 studies were removed as duplicates, resulting in 995 studies. A systematic screening approach resulted in 14 available full-text articles for review (Figure 1). Substantial agreement was achieved among reviewers at the title (κ = 0.90; 95% CI, 0.82 to 0.98), abstract (κ = 0.93; 95% CI, 0.79 to 1.00), and full-text (κ = 1.00; 95% CI, 1.00 to 1.00) screening stages.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of the search strategy for articles assessing the use of suprascapular nerve block for pain control after shoulder arthroscopy. NB, nerve block; RCT, randomized controlled trial.
Study Characteristics
The present review of 14 RCTs included a total of 1382 patients, with a mean age of 53.8 years (SD, 13.1 years). The mean follow-up time was 3.1 days (range, 24 hours to 6 weeks) (Table 1). Every study investigated SSNB; 11 studies additionally investigated ISB, and 3 studies examined a combined axillary nerve block and SSNB (Table 2).
Characteristics of Included Studies and Patients a

a ISB, interscalene block; NR, not reported; SSNB, suprascapular nerve block.
b Age expressed as mean (range).
Details of the Nerve Blocks and Anesthesia Used a
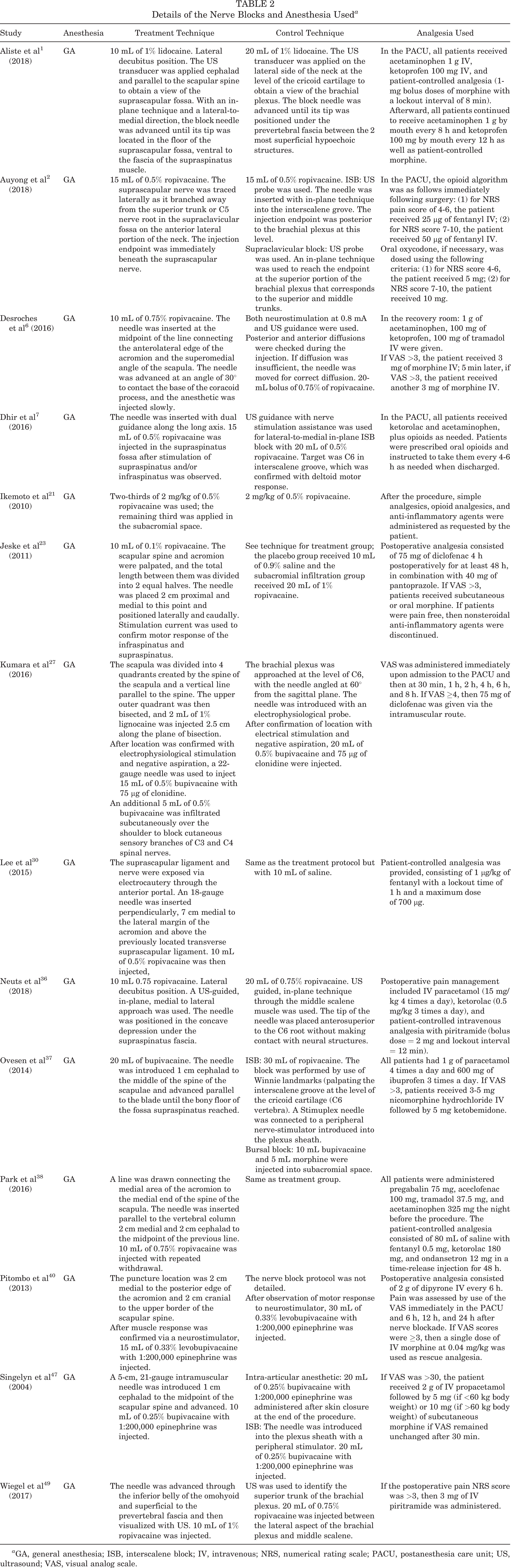
a GA, general anesthesia; ISB, interscalene block; IV, intravenous; NRS, numerical rating scale; PACU, postanesthesia care unit; US, ultrasound; VAS, visual analog scale.
Study Quality
Overall, study quality as assessed with the GRADE criteria was moderate. 12 Blinding of the patients or the outcome assessors was not consistently practiced in the studies. Additionally, selective reporting was an issue with several studies. Details of potential bias in each study are presented in Figure 2.

Risk of bias assessment summary: suprascapular nerve block for pain control after shoulder arthroscopy. Green “+” circles indicate low risk of bias, empty cells indicate unclear risk of bias, and red “−” circles indicate high risk of bias.
Pain Scores
Every study reported on postoperative pain scores and outcomes associated with the various nerve blocks. Eight studies reported postoperative pain using visual analog scale (VAS) scores, a continuous scale comprising a horizontal or vertical line, 10 cm (100 mm) in length. 20 Five studies reported postoperative pain scores using numerical rating scale (NRS) scoring, a numeric version of the VAS in which the patient selects the whole number (0-10) best reflecting the intensity of his or her pain 20 (Table 3).
Outcomes a

a ANB, axillary nerve block; ISB, interscalene block; IV, intravenous; NRS, numerical rating scale; PACU, postanesthesia care unit; PCA, patient-controlled analgesia; SSNB, suprascapular nerve block; VAS, visual analog scale.
SSNB Versus Control
Six studies 21,23,30,37,38,47 assessed the efficacy of SSNB in controlling pain postoperatively compared with a control group that did not involve nerve blocks. Three of these studies 23,38,47 found significantly reduced postoperative pain scores in the SSNB group compared with controls, while the remaining 3 studies 21,30,37 reported no significant difference. Pain control within 1 hour postoperatively was compared in 5 studies, 21,30,37,38,47 with significantly reduced pain identified in the SSNB groups (SMD, –0.76; 95% CI, –1.45 to –0.07; P = .03; I 2 = 84%) (Figure 3A). Five studies 21,30,37,38,47 compared pain control between 4 and 6 hours postoperatively, reporting significantly improved pain control in the SSNB groups (SMD, –0.81; 95% CI, –1.53 to –0.09; P = .03; I 2 = 85%) (Figure 3B). At 24 hours postoperatively, no significant difference was noted in pain control between patients who received SSNB versus controls (SMD, –0.20; 95% CI, –0.60 to 0.20; P = .32; I 2 = 61%) (Figure 3C). 21,23,30,37,38,47 These results indicate that SSNB is efficacious at improving pain control compared with control treatments in the early postoperative period; however, the effect may abate beyond 24 hours postoperatively.

Forest plots of standard mean difference between suprascapular nerve block (SSNB) group and control group for pain scores (A) within 1 hour (B), at 4 to 6 hours, and (C) at 24 hours postoperatively.
SSNB Versus ISB
Ten studies compared SSNB versus ISB. # All 10 studies reported pain scores while patients were recovering in the postanesthesia care unit (PACU). Pooled VAS and NRS scores from these studies revealed significantly less effective pain control in the SSNB group compared with the ISB group (SMD, 0.87; 95% CI, 0.28 to 1.46; P = .004; I 2 = 94%) (Figure 4A). Six studies 1,27,36,37,47,49 compared postoperative pain control at 3 to 4 hours postoperatively, with no significant difference found between the SSNB and ISB groups (SMD, 0.70; 95% CI, –0.23 to 1.62; P = .14; I 2 = 96%) (Figure 4B). Postoperative pain at 6 to 8 hours was compared in 6 studies, 1,6,7,21,27,36 with no significant difference found between the SSNB and ISB groups (SMD, 0.57; 95% CI, –0.02 to 1.16; P = .06; I 2 = 85% ) (Figure 4C). Pain at 24 hours postoperatively was reported in all 10 studies, with no significant difference found between SSNB and ISB (SMD, –0.04; 95% CI, –0.33 to 0.24; P = .76; I 2 = 74%) (Figure 4D).

Forest plots of standard mean difference between suprascapular nerve block (SSNB) group and interscalene brachial plexus block (ISB) group for pain scores (A) while patients were recovering in the postanesthesia care unit and (B) 3 to 4 hours, (C) 6 to 8 hours, and (D) 24 hours postoperatively.
Opioid Use
Twelve studies examined opioid use postoperatively.
SSNB Versus ISB
Ten studies ** assessed the difference in opioid consumption in patients with SSNB compared with ISB. Three of these studies 6,40,47 assessed the consumption in terms of percentage of patients requiring opioids. Two studies 6,40 reported a higher percentage of PACU patients requiring morphine in the SSNB group (39% and 53%) compared with the ISB group (12% and 12%) (P = .03 and P = .009). Conversely, no significant difference was found in patients requiring morphine at 24 hours postoperatively in the SSNB group (4% and 15%) compared with the ISB group (20% and 41%) (P = .08 and P = .16). Two studies 36,49 assessed the use of postoperative piritramide. One study 36 identified higher consumption in the SSNB compared with the ISB group within 8 hours of surgery (P = .004); however, there was no difference at 24 hours (P = .30). The other study 49 found no difference in the percentage of patients in the SSNB or ISB groups who required opioids in the PACU (7.3% and 7.3%, not significant). Three studies 2,7,47 assessed the quantity of opioids required in the PACU. Dhir et al 7 and Singelyn et al 47 reported significantly less morphine consumption by the ISB group (mean of 5.82 ME [morphine equivalents] and 0.5 ± 1.5 mg, respectively) compared with the SSNB group (mean of 13.97 ME and 4 ± 5 mg, respectively) (P < .001). In contrast, Auyong et al 2 found no significant difference in PACU opioid consumption between the SSNB group (0.52 ± 0.59 mg) and the ISB group (0.51 ± 0.85 mg).
SSNB Versus Placebo
Three studies 21,30,37 examined opioid use in SSNB compared with control groups. Lee et al 30 compared SSNB and placebo injection, reporting that significantly fewer fentanyl boluses were required for the SSNB group. Ikemoto et al 21 and Ovesen et al 37 similarly compared consumption of opioids in control groups (1.2 ampoules of opioids and 5.67 ± 10.46 mg of morphine, respectively) and SSNB groups (1.0 ampoule of opioids and 3.65 ± 7.71 mg of morphine, respectively); however, the differences did not meet the threshold of significance.
Length of Stay
There were 3 studies 2,6,30 that assessed length of stay outcomes. No significant difference was found in length of stay between the SSNB, ISB, and control groups.
Patient Satisfaction
A total of 7 studies 1,2,7,23,36,47,49 reported on patient satisfaction. Two studies, using a numeric rating scale from 0 to 100, found that ISB resulted in higher satisfaction at 6 hours (92 ± 14 vs 78 ± 2.7; P = .02) 7 and 24 hours (87 ± 12 vs 82 ± 17; P = .01) postoperatively. 47 Another study 49 reported higher satisfaction in the SSNB group, with 91% satisfied or highly satisfied with the block, compared with 79% of patients who received the ISB (P = .01). One study 23 found that when compared with placebo, SSNB resulted in significantly higher patient satisfaction at 48 hours (97 ± 5 vs 83 ± 12; P < .001) and at 14 days (95 ± 6 vs 79 ± 13; P = .001) postoperatively. Three other studies 1,2,36 reported no significant difference in patient satisfaction between the SSNB and ISB groups at 24 hours postoperatively.
Complications
Twelve studies †† reported on complications and side effects arising from the use of SSNB. Out of 257 cases for which the presence or absence of pneumothorax was reported, no cases of pneumothorax were associated with SSNB, whereas 1 case of pneumothorax was reported with the use of ISB (0.39%). 6 No other major complications, such as neurovascular impairment, cardiovascular collapse, or seizure, were reported following the use of SSNB. ISB was associated with increased rates of hoarseness (identified in a combined rate of 24/338 cases [7.1%]) and Horner syndrome (identified in a combined rate of 34/338 cases [10%]) when compared with SSNB (combined rates of 5/262 [1.9%] and 5/262 [1.9%], respectively). 49 Prolonged motor block (deficits in motor function of the hand and wrist at 24 hours) was also a concern with ISB (combined rate of 29/199 [14.6%]), with significantly higher rates than SSNB (combined rate of 3/198 [1.5%]). 7,40,49 Motor block at 24 hours was assessed by use of a 0 to 2 scale (0, complete; 1, incomplete; 2, none) in 2 of the studies, 7,40 whereas 1 study 49 used grip strength as the surrogate for motor block and used the Modified Medical Research Council Scale to measure hand muscle strength. 43
Three studies 37,40,47 compared symptoms of nausea and vomiting between SSNB and ISB. One study 47 found that the incidence of nausea and vomiting was lower in the ISB group, whereas the other 2 studies 37,40 identified no significant difference. One study 30 compared nausea and vomiting associated with SSNB and placebo and found no significant difference.
Discussion
The most significant finding of the present systematic review is that SSNB resulted in significantly improved pain control in the first 24-hour postoperative period compared with non–nerve block control groups. However, patients who received SSNB demonstrated significantly greater pain and increased opioid consumption compared with patients receiving ISB in the early postoperative period. SSNB may be associated with fewer major (pneumothorax, Horner syndrome) and minor (prolonged motor block, hoarseness) complications than ISB. The studies included in this review were from Asia, Europe, South America, and Canada.
As discussed, ISB has historically been considered the gold standard for regional pain blocks for pain control following shoulder arthroscopy. As well as providing postoperative anesthesia, ISB can be used to provide surgical anesthesia for patients undergoing shoulder arthroscopy. This may explain the improved pain control in the immediate postoperative period in patients receiving ISB. However, SSNB has been investigated recently given its theoretical efficacy along with the possibility of a reduced complication risk. The present meta-analysis of RCTs found that up to 24 hours postoperatively, SSNB significantly reduced pain in patients undergoing shoulder arthroscopy compared with those who received no nerve block. However, SSNB provided inferior pain control compared with ISB, particularly in the short-term period (within 6 hours postoperatively). At 24 hours postoperatively, no difference was found in pain control between the SSNB and the ISB groups. The 30% of the joint and capsule that is innervated by the lateral pectoral and axillary nerves rather than the suprascapular nerve may explain this imperfect early pain control in the SSNB groups. Moreover, the suprascapular nerve rarely has cutaneous innervation, and therefore the SSNB does not provide analgesia for the pain from skin incisions.
It is thought that the 30% of the shoulder joint that is not innervated by the suprascapular nerve is likely mostly innervated by the axillary nerve. 41 It has therefore been hypothesized that the combination of an SSNB with an axillary nerve block would provide patients with effective pain control postoperatively. 7 The axillary nerve block in combination with SSNB was found to provide improved postoperative pain control compared with SSNB alone in 1 study. 38 Dhir et al 7 found that the combination of axillary and suprascapular nerve blocks provided improved pain control, even compared with ISB, at 24 hours postoperatively; however, ISB was superior immediately postoperatively when the patients were still in the PACU. Although effective, the combination of both SSNB and an axillary nerve block has the disadvantage of taking twice as much time as a single nerve block and would therefore only be practical in centers that have dedicated “block rooms” outside the operating room.
The SSNB can be guided by use of anatomic landmarks alone (blind) or with the assistance of modalities for a guided approach. 19,22 Electrophysiology-guided SSNB has been shown to provide more effective blocks than blind techniques. 24,50 Ultrasound guidance has been reported to improve the accuracy and efficacy of suprascapular nerve blocks by allowing the provider to visualize the suprascapular nerve with high-resolution transducers. 39 The technique for SSNB reported in the studies we reviewed typically involved identification of the midpoint of the spine of the scapula with the patient in lateral decubitus position. The needle was then introduced approximately 1 cm cephalad to this landmark and advanced parallel to the blade until the floor of the supraspinatus fossa was reached. Anywhere from 10 to 20 mL of lidocaine, ropivacaine, or bupivacaine was then injected. One study 25 that compared the blind SSNB with both the electrophysiology-guided SSNB and the ultrasound-guided block found that the latter two guided blocks may provide improved pain relief over the blind techniques. Furthermore, the anterior approach to the suprascapular nerve was uniquely used by 1 study included in this review. 49 Such an approach would not have been possible before the availability of ultrasound guidance. Another unique approach was described in the study by Lee et al, 30 who used an arthroscopically guided approach to the suprascapular nerve. Such approaches must be considered when interpreting the results from these studies.
The technique for ISB reported in the studies we reviewed involved introduction of the needle through the middle of the scalene muscle at the level of C6 with or without ultrasound guidance and/or neurostimulation. Anywhere from 10 to 20 mL of lidocaine, ropivacaine, or bupivacaine was then injected. Whereas ISB can provide excellent postoperative pain control after arthroscopic shoulder surgery, 46 1 study 34 found that 16% of patients reported immediate block side effects, with more than 4% reporting persistent neurological complications. The rates of persistent neurological complications following ISB ranged from to 2.5% to 4.2% in other large trials. 4,48 Moreover, a rebound phenomenon of increased pain after 12 hours postoperatively has been reported following ISB. 35 While increased pain and prolonged neurological deficits are important complications to consider, the major complications such as cardiac arrest, pneumothorax, respiratory distress, phrenic nerve palsy, and central nervous toxicity are key factors that cause surgeons and anesthesiologists to consider other modalities for postoperative pain control. 34,42 Another group of patients who may not receive complete benefit from ISB includes those with obesity. In a study of 528 patients receiving ISB, Schroeder et al 44 found that those with an increased body mass index required longer times to complete the block and reported inferior pain control postoperatively. SSNB has been proposed as a safe and efficacious alternative to ISB for postoperative pain control following shoulder surgery. 8 Similarly, the present review found that fewer instances of major complications such as pneumothorax, moderate complications including Horner syndrome, and minor complications such as hoarseness and prolonged motor block occur in patients receiving SSNB compared with ISB.
Strengths and Limitations
Strengths of this systematic review include the assessment of RCTs, which inherently have less bias. Additionally, the GRADE system was used for assessment of study quality, considering a range of quality measures to ensure the accurate and comprehensive assessment of the overall body of evidence. However, this systematic review was limited to the quality of the individual studies included. The most significant source of bias identified was related to the selective and incomplete reporting of outcomes. For example, studies that assessed multiple time intervals and reported only those that entailed significant results contributed to an overestimation of the overall effect of an intervention. Other bias inherent to the present review relates to the inability to blind the operator or clinician to the technique being performed because of the nature of the interventions. Techniques to blind the outcome assessors, such as concealment of the block sites, were used in some studies but not all. 7 Furthermore, heterogeneity was found across the included studies in terms of nerve block techniques as well as outcome measures and timing of assessment, which precluded the pooling of many of the secondary outcomes.
Another limitation relates to the techniques with which the blocks were performed in the individual studies, particularly the strategies used for landmarking. In 1 of the studies 6 included in this review, ultrasound guidance was used to perform the ISB, but landmarks alone were used for SSNB. In another study, 6 ISB was carried out via neurostimulation, whereas SSNB was performed using only a landmark-based technique. Such differences in landmarking may have contributed to differences noted between blocks within the individual studies. Further, we could not account for the potential differences in the skill level of the anesthesiologists performing the nerve blocks across the included studies. We excluded non–English language studies, and this may have left out some studies that would have changed the results. We found significant statistical heterogeneity across studies, measured using the I 2 statistic for several of the assessed SMDs which reduced our confidence in the pooled results. However, we combined the rates using a random-effects model in a meta-analysis of proportions to account for these differences. All nerve blocks and studies assessing them should have a reported failure rate to allow proper assessment of the success of the block. Failure rates were poorly defined across the included studies, with only 1 study 49 reporting the criteria used to categorize a block failure. Further large-scale RCTs comparing the efficacy and complication rates of SSNB and ISB are indicated in order to elucidate definitive conclusions.
Conclusion
Although not more efficacious than ISB in terms of pain control, the use of SSNB provides patients undergoing shoulder arthroscopy with significantly improved pain control compared with patients receiving analgesia without a nerve block. Moreover, SSNB is a safe procedure with few major and minor complications reported.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: G.A. receives royalties from ConMed Linvatec, Inspace Orthospace, Exactech, and Wright Medical. O.R.A. is part of the speakers’ bureau for ConMed and the Arthroscopy Association of Canada. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
Detailed Search Strategy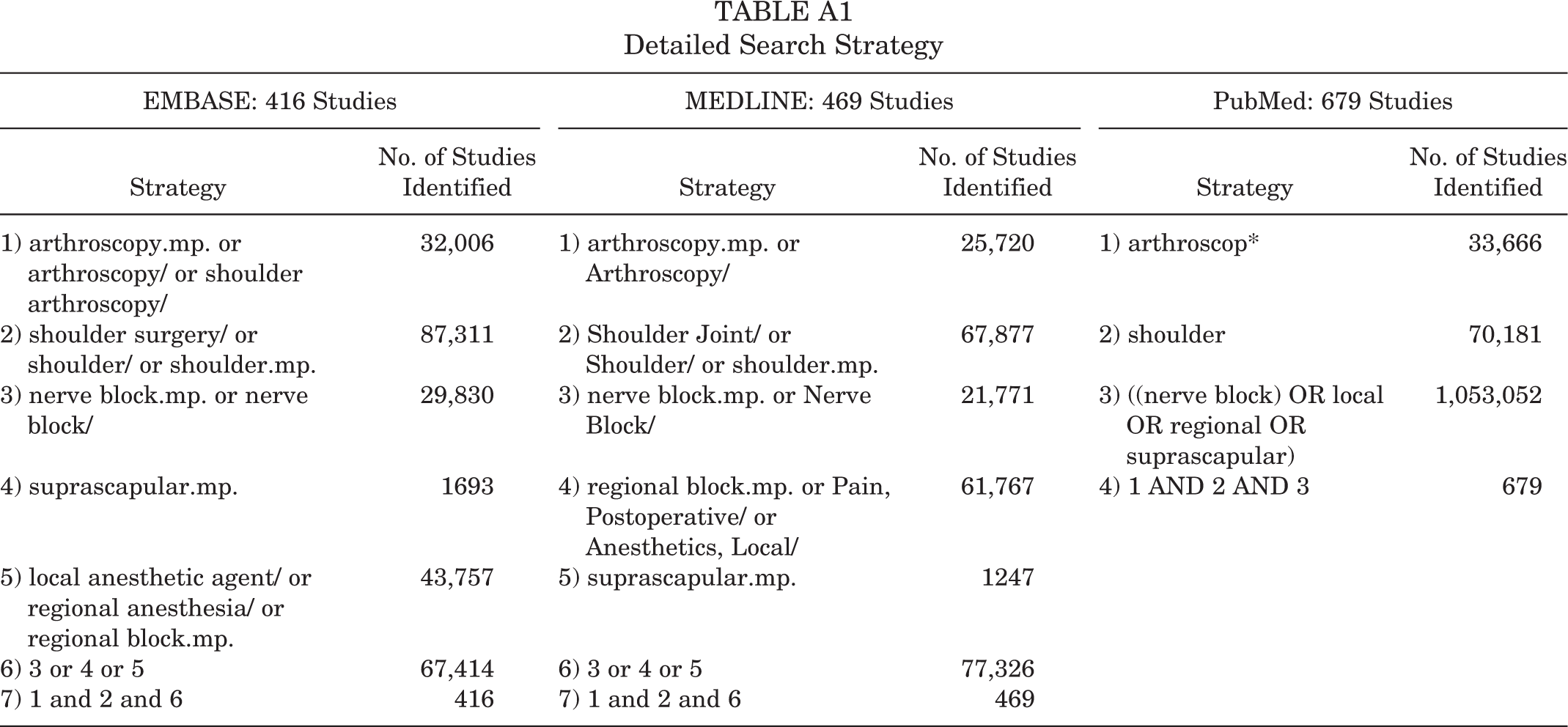
EMBASE: 416 Studies
MEDLINE: 469 Studies
PubMed: 679 Studies
Strategy
No. of Studies Identified
Strategy
No. of Studies Identified
Strategy
No. of Studies Identified
1) arthroscopy.mp. or arthroscopy/ or shoulder arthroscopy/
32,006
1) arthroscopy.mp. or Arthroscopy/
25,720
1) arthroscop*
33,666
2) shoulder surgery/ or shoulder/ or shoulder.mp.
87,311
2) Shoulder Joint/ or Shoulder/ or shoulder.mp.
67,877
2) shoulder
70,181
3) nerve block.mp. or nerve block/
29,830
3) nerve block.mp. or Nerve Block/
21,771
3) ((nerve block) OR local OR regional OR suprascapular)
1,053,052
4) suprascapular.mp.
1693
4) regional block.mp. or Pain, Postoperative/ or Anesthetics, Local/
61,767
4) 1 AND 2 AND 3
679
5) local anesthetic agent/ or regional anesthesia/ or regional block.mp.
43,757
5) suprascapular.mp.
1247
6) 3 or 4 or 5
67,414
6) 3 or 4 or 5
77,326
7) 1 and 2 and 6
416
7) 1 and 2 and 6
469