
Abstract
Background:
There is limited evidence regarding the patient-related factors that influence treatment outcomes after an acute Achilles tendon rupture.
Purpose/Hypothesis:
The purpose of this study was to determine the predictors of functional and patient-reported outcomes 1 year after an acute Achilles tendon rupture using a multicenter cohort and to determine patient characteristics for reporting within the top and bottom 10% of the Achilles tendon Total Rupture Score (ATRS) and heel-rise height outcomes. The hypothesis was that older age, greater body mass index (BMI), and female sex would lead to inferior outcomes.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients were selected by combining 5 randomized controlled trials from 2 different centers in Sweden. Functional outcomes were assessed using validated heel-rise tests (height, number of repetitions, total work, and concentric power) for muscular endurance and strength, and the relationship between injured and uninjured legs was calculated as the limb symmetry index (LSI). Patient-reported outcomes were measured using the ATRS. All outcomes were collected at the 1-year follow-up. Independent predictors included were patient sex, smoking, BMI, age, and surgical versus nonsurgical treatment.
Results:
Of the 391 included patients, 307 (79%) were treated surgically. The LSI of heel-rise height at the 1-year follow-up decreased by approximately 4% for every 10-year increment in age (beta, –3.94 [95% CI, –6.19 to –1.69]; P = .0006). In addition, every 10-year increment in age resulted in a 1.79-fold increase in the odds of being in the lowest 10% of the LSI of heel-rise height. Moreover, a nonsignificant superior LSI of heel-rise height was found in patients treated surgically compared with nonsurgical treatment (beta, –4.49 [95% CI, –9.14 to 0.16]; P = .058). No significant predictor was related to the ATRS. Smoking, patient sex, and BMI did not significantly affect the 1-year results for the LSI of the heel-rise tests.
Conclusion:
Older age at the time of injury negatively affected heel-rise height 1 year after an Achilles tendon rupture. Irrespective of age, a nonsignificant relationship toward the superior recovery of heel-rise height was seen in patients treated surgically. None of the factors studied affected patient-reported outcomes.
An Achilles tendon rupture is a common injury with an increasing incidence during the past decade. 10,11 The injury is more common in men than in women, with a ratio of 1:8 to 1:10, respectively. 14,18 Historically, the question of surgical or nonsurgical management has been the subject of debate. 6,33 A recent meta-analysis of randomized controlled trials (RCTs) 6 reported that the risk of reruptures is almost 3 times higher in nonsurgically treated patients (9.8%) compared with those treated surgically (3.7%). Regardless of treatment, the majority of patients will suffer from reduced function compared with their preinjury status and compared with the healthy side. 12,14,17,19 There is limited evidence in terms of the patient-related factors that influence treatment outcomes after an acute Achilles tendon rupture. Moreover, the reasons for the large variation in outcomes, in terms of both symptoms and functional deficits, after an acute Achilles tendon rupture are still largely unknown. 13,20
Previous studies investigating outcomes after an acute Achilles tendon rupture have been inconclusive in terms of predictors. 2,5,24,28 For instance, 1 study found worse function and greater symptoms in women 28 ; another reported male sex, older age, and deep venous thrombosis as predictors of poor outcomes 2 ; and a third found that high body mass index (BMI) and older age were strong predictors of poor patient-reported outcomes. 24 However, these previous studies were limited by small cohort sizes, implying the need for well-controlled studies with larger cohorts.
The purpose of this study was to determine the predictors of functional and patient-reported outcomes 1 year after an acute Achilles tendon rupture using a large cohort from 2 centers. The second purpose was to determine patient characteristics for reporting within the top and bottom 10% of the Achilles tendon Total Rupture Score (ATRS) and heel-rise height outcomes. The hypothesis was that older age, higher BMI, and female sex would lead to an inferior outcome.
Methods
Overall, 482 patients with an acute Achilles tendon rupture, from 5 RCTs at 2 different centers in Sweden, were included in this study. All of the RCTs were approved by regional ethical review boards in Sweden (Nos. 032-09, S617-03, 2013/1791-31/3, and 2009/2079-31/2). Of the 482 patients eligible from the different cohorts, 391 patients (83%) were included in the analysis, while 91 patients (17%) were excluded because of missing follow-up data. The results of these RCTs have been previously published. 1,7,8,21,26 The patient-related variables of interest were age, patient sex, smoking, treatment, and BMI. The best and worst 10% of patients for the 1-year ATRS and heel-rise height were further subanalyzed to study the predictors of their superior and inferior outcomes. A flow chart of the study is demonstrated in Figure 1.

Flowchart of included studies. ATRS, Achilles tendon Total Rupture Score.
Cohort Descriptions
Nilsson-Helander et al. 21
A total of 97 patients from this trial were eligible for inclusion in the present study for the 1-year follow-up. The patients were originally randomized to either surgical or nonsurgical treatment; 42 patients were treated nonsurgically, and 47 patients were treated with open repair using resorbable Kessler sutures. A below-the-knee cast with the foot in the equinus position was used for 2 weeks and then replaced by an adjustable brace (DonJoy MaxTrax ROM Walker; DJO Global) for a further 6 weeks. Weightbearing as tolerated was allowed after 6 to 8 weeks. Patients were evaluated after 1 year. From this RCT, 87 patients were included in this study.
Olsson et al. 25
A total of 100 patients, randomized to surgical or nonsurgical treatment, were eligible for inclusion in the present study. Enhanced open surgical repair using semiresorbable sutures was performed. A walking brace was used for 6 weeks postoperatively, followed by accelerated rehabilitation. All patients were allowed immediate full weightbearing and started range of motion as well as strength training 2 weeks postoperatively after initial cast immobilization. The patients in the nonsurgically treated group used the same walking brace for 8 weeks and were also allowed full immediate weightbearing. Follow-ups were performed after 1 year. A total of 88 patients from the original cohort were included in the present study.
Domeij-Arverud et al. 8
A total of 40 patients were eligible. All patients in this RCT were treated with open surgical repair using a modified Kessler technique and were subsequently randomized to 2 different postoperative protocols. The control group (26 patients) received a below-the-knee plaster cast with the ankle in 30° equinus at the outpatient clinic after the completion of surgery and were nonweightbearing with crutches during the first 2 weeks. The intervention group (21 patients) received additional treatment with adjuvant intermittent pneumatic compression (IPC) under the plaster cast for a minimum of 6 hours a day (Covidien A-V Impulse; Orthofix Vascular Novamedix). IPC was discontinued after 2 weeks. At the 2-week visit, all patients were fitted with a lower leg brace for 6 weeks (DonJoy MaxTrax ROM Walker) and were instructed to start full weightbearing. From this study, 25 surgically treated patients were included in this predictor analysis.
Domeij-Arverud et al. 7
A total of 150 patients were eligible for inclusion from this study. All patients were treated with open surgical repair using a modified Kessler technique. Postoperatively, patients were randomized to either standard plaster cast treatment or IPC (VenaFlow Elite; DJO Global) beneath a walking brace (Aircast XP Walker; DJO Global). Patients were treated with a plaster cast in a 30° equinus position and were nonweightbearing during the first 2 postoperative weeks when crutches were used. The intervention group using the brace was instructed to apply bilateral IPC during the time when they were sedentary for a minimum of 6 hours per day. The device was applied under the brace with 3 wedges, and patients were allowed to bear weight as tolerated. IPC treatment was discontinued 2 weeks postoperatively. At the 2-week visit, all patients were fitted with a lower leg brace (Aircast XP Walker) and were instructed to bear weight fully during the 6 weeks when the brace was worn. A total of 119 surgically treated patients were included in this predictor analysis.
Svedman et al. 31
A total of 95 patients from this trial were eligible for inclusion in the present study for the 1-year follow-up. All patients were treated with open surgical repair using a modified Kessler technique, and they were postoperatively randomized to either direct postoperative weightbearing in a functional brace (VACOped; OPED) with full weightbearing for 6 weeks or to nonweightbearing plaster cast immobilization for 2 weeks, followed by a brace for a further 4 weeks. A total of 72 surgically treated patients from the original cohort were included in this study.
Patient-Reported Outcomes
The ATRS 22 is a validated and injury-specific outcome tool used for patients with acute Achilles tendon ruptures. 9 Patients answer 10 questions that are scored from 0 to 10. A score of 0 implies significant symptoms and difficulty with physical activity, while a score of 10 implies no difficulties. Responses to the 10 items are summed to produce a total score in which the maximum is 100 points and means no difficulties at all, comparable with full recovery.
Functional Outcomes
The functional tests were performed using a linear encoder by MuscleLab (Ergotest Innovation). The tests have been validated for examining functional outcomes in patients treated for acute Achilles tendon ruptures. 29,30
Height, Number of Repetitions, and Total Work
The heel-rise test was performed with the patient standing on a 20-cm flat box with a 10° incline. The patients were asked to begin with the healthy side. They were asked to perform as many repetitions as possible in which each repetition was supposed to be performed with maximum heel-rise height. A spring-loaded string was attached to the patient’s shoe to measure both height (in centimeters) and the number of repetitions. This string was in turn connected to a linear encoder unit, which recorded the measurements. The system used the patient’s weight to calculate the total amount of work (body weight × total distance [in Joules]). When the patient was no longer able to perform an adequate heel rise, the test was stopped by the examiner. The maximum height achieved on a heel rise was also documented.
Concentric Power
The heel-rise test was performed with the patient standing in a weight training machine and performing a single-leg heel rise. With knee flexion restricted to within 20°, patients were instructed to raise their heel as quickly and forcefully as possible. This test was repeated 3 times initially, with the patient’s body weight plus 13 kg. Another 10 kg was added sequentially when an increase in power was measured, and the test was finished when a decrease in power output was noted. The maximum power (in watts) was recorded as the result. Similar to the other heel-rise test, a linear encoder was attached to the patient’s shoe, and standardized equipment was used to record the test.
Statistical Analysis
Data analysis was performed using SAS/STAT version 14.2 (SAS Institute). Continuous variables were described as mean, standard deviation, median, and range, and categorical variables were described as count (n) and proportion (%). The results from the tests of muscle function were reported as the limb symmetry index (LSI), defined as the ratio between the involved limb score and the uninvolved limb score and expressed as a percentage (result of involved/result of uninvolved × 100 = LSI). For comparisons between included and excluded patients, the Fisher exact test (lowest 1-sided P value multiplied by 2) for dichotomous variables and the Mann-Whitney U test for continuous variables were performed. Distributions of outcomes were checked with box plots. In cases of nonlinear distribution, Spearman rho was used to determine correlations between predictors and outcomes. In addition, outcomes were compared with the Mann-Whitney U test stratified by the dichotomous predictor. Linear regression modeling was performed to analyze the effect of patient demographics on the LSI of the different tests of muscle function.
The results of linear regression were reported as beta estimates, 95% CIs, and P values. The R 2 value was given as a measurement of the goodness-of-fit model. The likelihood of reporting in the top or bottom 10% of the ATRS and LSI of heel-rise height was analyzed with binary regression modeling. Patient demographics and treatment were used as independent variables. The results of the binary regression models were presented as odds ratios (ORs), 95% CIs, and P values. An OR was expressed for every unit increase in the predictor variable. All significance tests were 2-sided and conducted at the 5% significance level. Forward stepwise multivariate regression modeling was planned in cases in which more than 1 predictor was found to be significant.
Results
The mean age of the 391 patients included in this study was 40.4 years (range, 18-71 years), 17% were women, and 79% of the cohort was treated with surgery. No differences in baseline demographics were found between the included and excluded patients (Table 1).
Demographics of Eligible Participants

Achilles Tendon Total Rupture Score
The mean 1-year ATRS was 81.3 ± 18.9. Because of the nonlinear distribution of the ATRS, regression analysis was not considered appropriate. No significant correlations were found between the 1-year ATRS and baseline demographics. In addition, no significant differences in patient-reported or functional outcomes were found for BMI, between sexes, smokers and nonsmokers, or type of treatment.
Heel-Rise Height
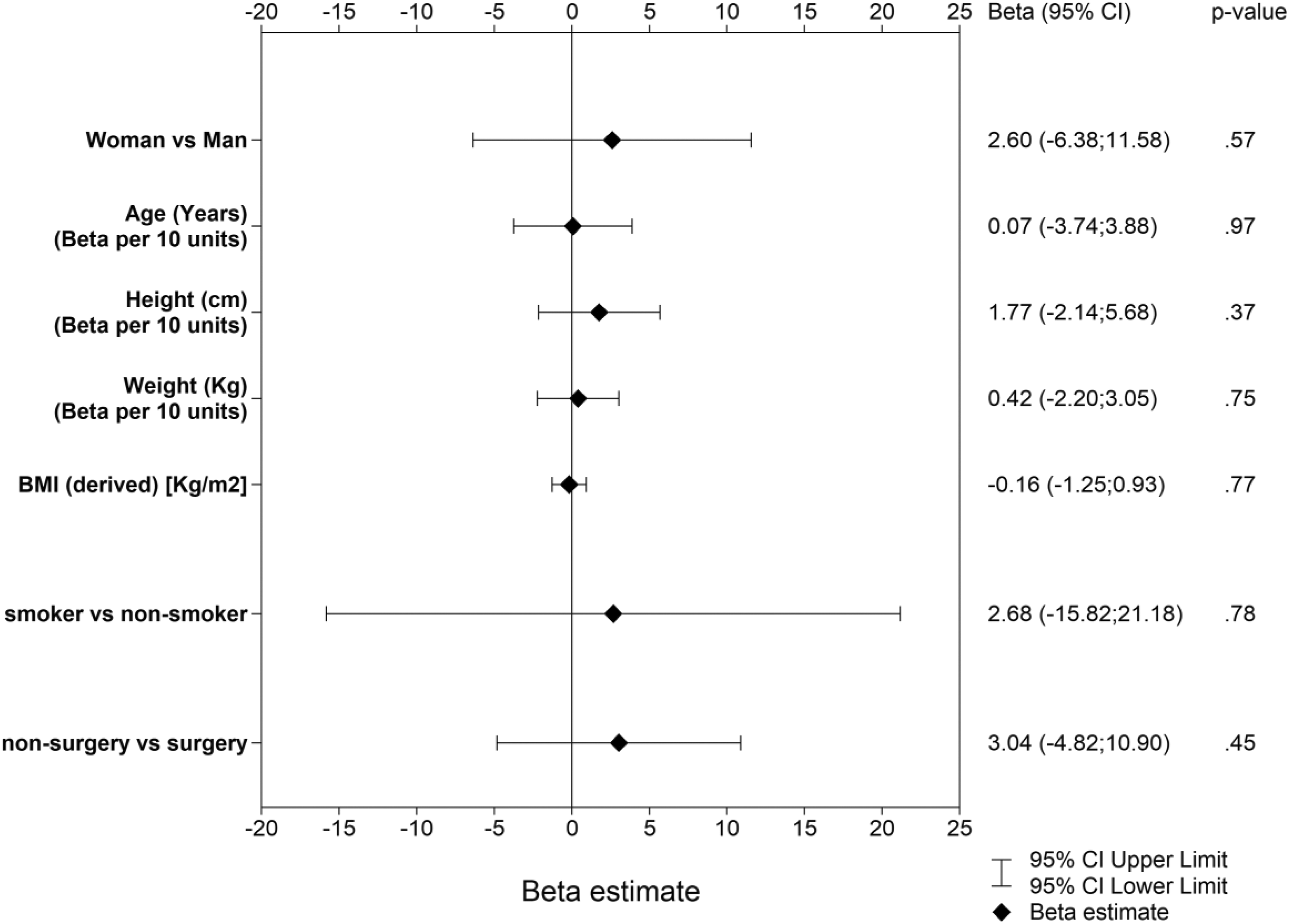
The mean 1-year LSI of heel-rise height was 83% ± 19%. At 1 year postoperatively, the LSI of heel-rise height decreased by around 4% for every 10-year increment in age (beta, –3.94 [95% CI, –6.19 to –1.69]; P = .0006). In addition, a nonsignificant relationship toward a superior LSI of heel-rise height was found in patients treated with surgery compared with nonsurgical treatment (beta, –4.49 [95% CI, –9.14 to 0.16]; P = .058) (Appendix Table A1 and Figure 2).

Linear regression models, odds ratios, and 95% CIs for the limb symmetry index of heel-rise height. BMI, body mass index.
Concentric Power
The mean 1-year LSI of concentric power during the heel-rise test was 83.3% ± 31.9%. No variable was found to be significant when attempting to predict the 1-year LSI of concentric power from the heel-rise test (Appendix Table A2 and Figure 3).
Linear regression models, odds ratios, and 95% CIs for the limb symmetry index of concentric power. BMI, body mass index.
Total Work
The mean LSI of total work during the heel-rise test was 73.6% ± 32.1%. No variable was found to be significant when attempting to predict the 1-year LSI of total work from the heel-rise test (Appendix Table A3 and Figure 4).

Linear regression models, odds ratios, and 95% CIs for the limb symmetry index of total work. BMI, body mass index.
Number of Repetitions
The mean 1-year LSI of number of repetitions was 89.4% ± 23.5%. No variable was found to be significant when attempting to predict the 1-year LSI of total number of repetitions from the heel-rise test (Appendix Table A4 and Figure 5).

Linear regression models, odds ratios, and 95% CIs for the limb symmetry index of number of repetitions. BMI, body mass index.
Top 10% of the ATRS
No variable was found to be significant when attempting to predict reporting in the top 10% of the ATRS 1 year after an Achilles tendon rupture (Appendix Table A5 and Figure 6).

Logistic regression models, odds ratios (ORs), and 95% CIs for patients in the top 10% of the Achilles tendon Total Rupture Score. BMI, body mass index.
Bottom 10% of the ATRS
No variable was found to be significant when attempting to predict reporting in the bottom 10% of the ATRS 1 year after an Achilles tendon rupture (Appendix Table A6 and Figure 7).

Logistic regression models, odds ratios (ORs), and 95% CIs for patients in the bottom 10% of the Achilles tendon Total Rupture Score. BMI, body mass index.
Top 10% of Heel-Rise Height
No variable was found to be significant when attempting to predict reporting in the top 10% of the LSI of heel-rise height 1 year after an Achilles tendon rupture (Appendix Table A7 and Figure 8).
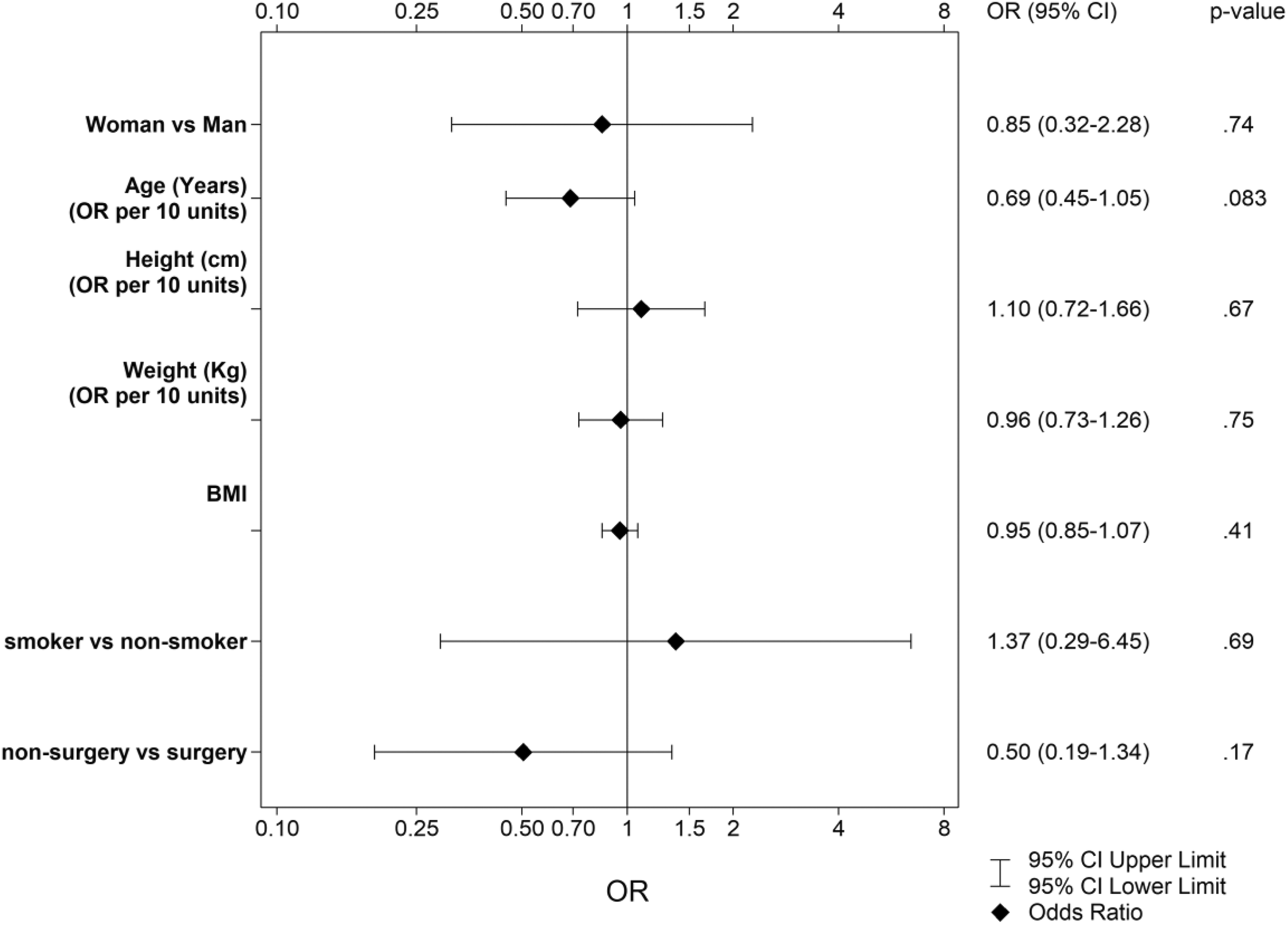
Logistic regression models, odds ratios (ORs), and 95% CIs for patients in the top 10% of the limb symmetry index of heel-rise height. BMI, body mass index.
Bottom 10% of Heel-Rise Height
A 1.79-fold increase in the odds of being in the bottom 10% of the LSI of heel-rise height 1 year after an Achilles tendon rupture was found for every 10-year increment in age (P = .0026) (Appendix Table A8 and Figure 9).
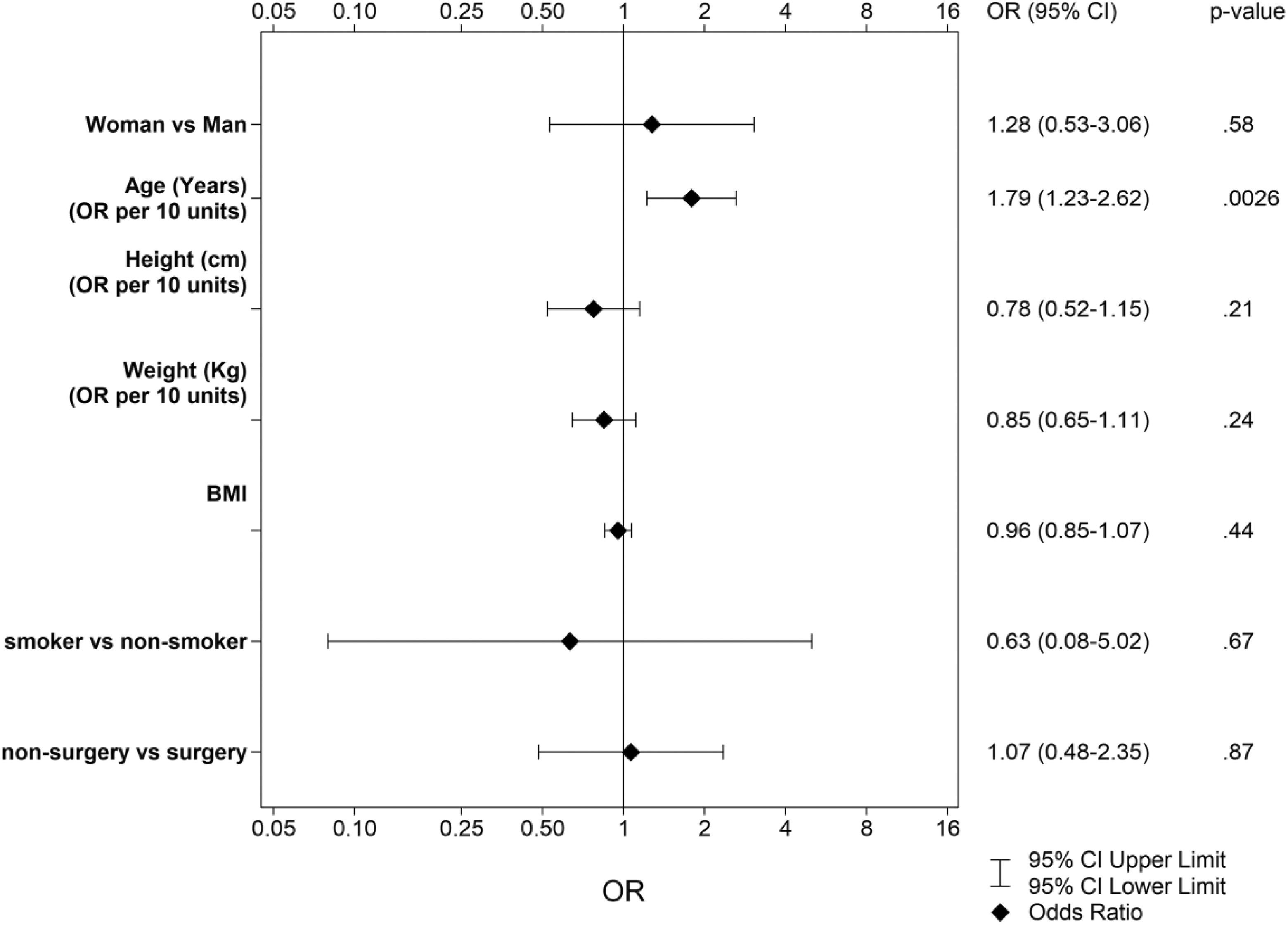
Logistic regression models, odds ratios (ORs), and 95% CIs for patients in bottom 10% of the limb symmetry index of heel-rise height. BMI, body mass index.
Discussion
The most important finding of this study is that older age at the time of injury predicted a poorer 1-year functional outcome after an acute Achilles tendon rupture; that is, the odds of achieving a more symmetrical heel-rise height became progressively worse with increasing age at the time of injury. There was also a nonsignificant relationship for surgically treated patients to experience greater recovery of heel-rise height in comparison with nonsurgically treated patients. No differences in functional outcomes could be identified between the sexes or in patients with a higher BMI. None of the studied factors were seen to significantly affect patient-reported outcomes.
The finding in the present study of a poorer functional outcome related to aging is in agreement with previous predictor studies of patients after acute Achilles tendon ruptures. 2,24 The decrease in heel-rise height found among older patients may be explained by degenerative changes related to age and changes in collagen synthesis, leading to increased stiffness. 32 The mechanisms suggested to contribute to tendon changes with age are the formation of advanced glycation end-product crosslinks, an aging stem cell population, reactive oxygen species, and cellular senescence. 4
Patient age was, however, not a risk factor for inferior results in the ATRS, which suggests that despite poorer recovery of the patients’ heel-rise height, this outcome did not imply poorer subjective recovery. It can be hypothesized that as patients grow older, they lower their expectations and reduce their demands for lower limb function, which might be reflected by their ATRS.
Older age at the time of an Achilles tendon rupture was a strong negative predictor of inferior heel-rise height in the present study, but it was not able to predict a poorer outcome for any of the other studied functional variables or for the patient-reported ATRS. Because age is a nonmodifiable factor, it might be especially important to thoroughly evaluate the optimal treatment regimen in the older patient population. Each patient’s expectations and functional demands should therefore be incorporated in the treatment algorithm, including surgical repair and postoperative rehabilitation.
It is not known whether differences in postoperative rehabilitation or modifications in the surgical techniques employed could be attributed to the observed age-related poor heel-rise height. However, a clear trend toward a more symmetrical heel-rise height was shown for surgically treated patients in this study compared with nonsurgically treated patients. This is possibly because surgically treated tendon ruptures may have less of a likelihood of elongation, as the surgeon has the opportunity to appose the ends of the ruptured tendon closely at the time of surgery; however, this has yet to be proven in the literature. Elongation of the tendon is known to lead to poorer outcomes, and an elongated tendon is related to a lower heel-rise height. If surgery is able to predict a better heel-rise height, it may then be important for patients with high physical demands to be surgically treated to maximize the chance of a better outcome.
Fortunately, smoking is rare in patients who sustain an Achilles tendon rupture. The injury mainly affects active men between the ages of 35 and 45 years, and the prevalence of smoking in this group is very low. 21 This explains why only 17 smokers were included in the present analysis. Data on smoking were, however, missing in 90 patients, as this was not part of the study protocol, and it may have influenced the proportion of smokers found in the cohort and the results of the analyses. It is surprising that smoking did not predict a poorer outcome in any of the analyzed measures, as it is often reported to be a negative predictor of outcomes for other orthopaedic injuries, such as rotator cuff ruptures and spinal surgery. 11,15,27
The question of whether patient sex plays a role in outcomes after an acute Achilles tendon rupture has been much debated, as previous predictor studies have reported conflicting results. 2,3,24,28 To the best of our knowledge, no previous predictive model has included as many women as the present study. This is likely because of the nature of the incidence of this injury, which primarily affects male patients. In this study, patient sex did not predict any of the 4 tested outcomes, nor did it influence the analyses of superior and inferior outcomes. This finding is important, as it can provide insight into why previous results are conflicting, and it is likely that patient sex should not be regarded as a predictor of outcomes.
The finding in this study that BMI did not affect outcomes is in disagreement with earlier studies. 16,23 Olsson et al 24 concluded that a high BMI predicted a worse ATRS at both 6 and 12 months, but no correlation was found with heel-rise height.
As the optimal treatment is still very much open to debate, it is important to evaluate predictors that can help to guide the physician in deciding a management strategy. Including goodness-of-fit analysis in the study adds additional strength compared with previous predictor studies of acute Achilles tendon ruptures. However, it should be emphasized that the regression models in this study were limited by the overall poor capacity of the models to predict the dependent outcome because none of the R 2 values was higher than 0.03 and results from area under the receiver operating characteristic curve analyses were no better than chance. This implies that there are other important aspects of treatment that affect the outcomes in these patients. There has been an increased focus on individualized treatment after acute Achilles tendon ruptures in recent years, which requires a deeper understanding of factors contributing to variations in outcome. Potentially, the current outcome measures are not sensitive enough to provide us with the answers necessary for improving therapy. For instance, there is a considerable ceiling effect for the ATRS. 22 A further limitation of the present study is the multiple univariate regression analyses that were performed, which results in a risk of mass significance and questions the small number of significant findings in this study. Unfortunately, no multivariate models could be performed because of the small number of factors that affected outcomes. The use of multivariate models would have allowed for a more in-depth analysis in which explicit subgroups of patients could have been studied. Finally, this study is limited by the fact that the patients were included from previous RCTs, with different surgical methods and rehabilitation protocols, which entails a risk of transfer bias.
Conclusion
Older age at the time of injury negatively affected heel-rise height 1 year after an Achilles tendon rupture. Irrespective of age, a nonsignificant relationship toward the superior recovery of heel-rise height was seen in patients treated surgically. None of the factors studied affected patient-reported outcomes.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics review boards in Gothenburg and Stockholm.
APPENDIX
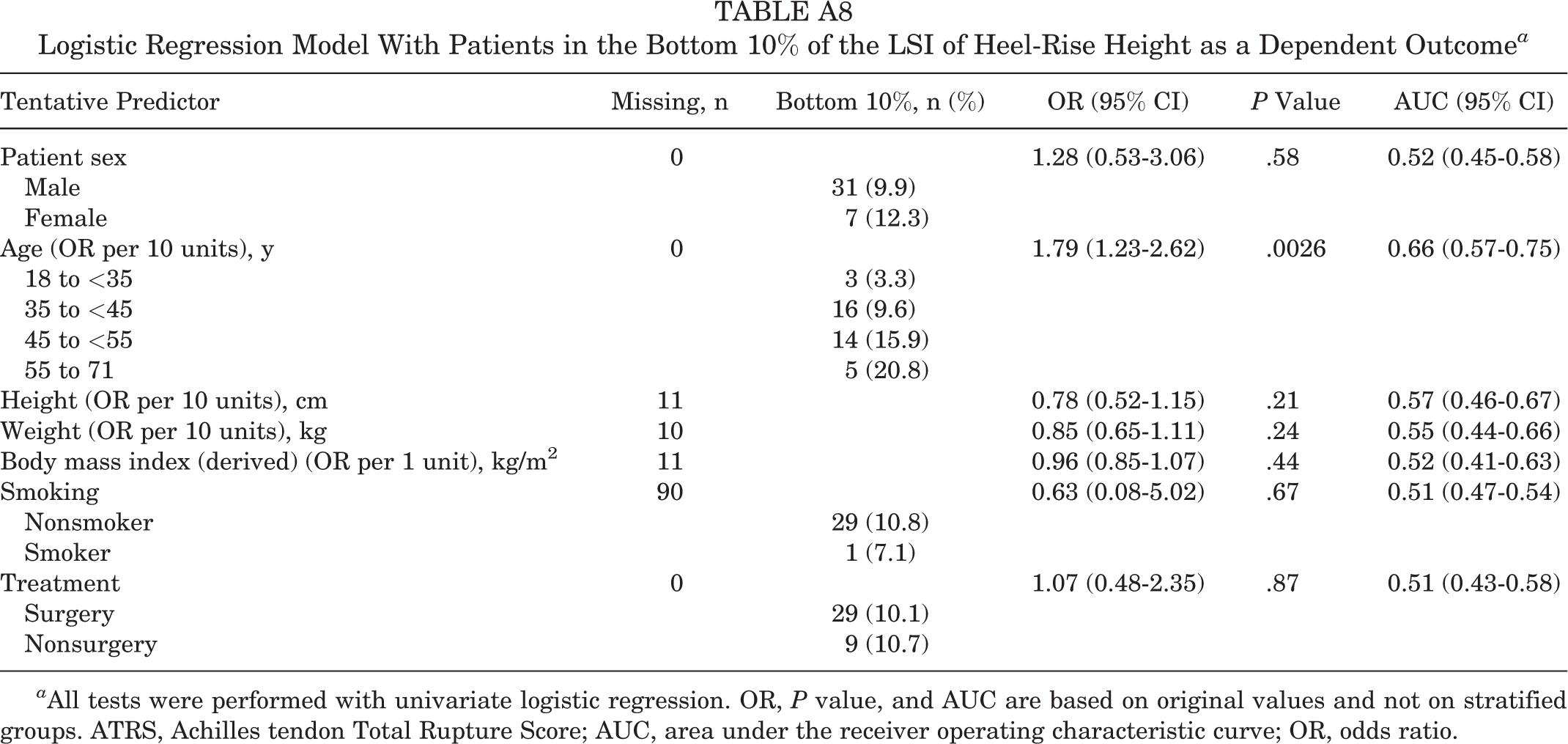
Logistic Regression Model With Patients in the Bottom 10% of the LSI of Heel-Rise Height as a Dependent Outcome a
| Tentative Predictor | Missing, n | Bottom 10%, n (%) | OR (95% CI) | P Value | AUC (95% CI) |
|---|---|---|---|---|---|
| Patient sex | 0 | 1.28 (0.53-3.06) | .58 | 0.52 (0.45-0.58) | |
| Male | 31 (9.9) | ||||
| Female | 7 (12.3) | ||||
| Age (OR per 10 units), y | 0 | 1.79 (1.23-2.62) | .0026 | 0.66 (0.57-0.75) | |
| 18 to <35 | 3 (3.3) | ||||
| 35 to <45 | 16 (9.6) | ||||
| 45 to <55 | 14 (15.9) | ||||
| 55 to 71 | 5 (20.8) | ||||
| Height (OR per 10 units), cm | 11 | 0.78 (0.52-1.15) | .21 | 0.57 (0.46-0.67) | |
| Weight (OR per 10 units), kg | 10 | 0.85 (0.65-1.11) | .24 | 0.55 (0.44-0.66) | |
| Body mass index (derived) (OR per 1 unit), kg/m2 | 11 | 0.96 (0.85-1.07) | .44 | 0.52 (0.41-0.63) | |
| Smoking | 90 | 0.63 (0.08-5.02) | .67 | 0.51 (0.47-0.54) | |
| Nonsmoker | 29 (10.8) | ||||
| Smoker | 1 (7.1) | ||||
| Treatment | 0 | 1.07 (0.48-2.35) | .87 | 0.51 (0.43-0.58) | |
| Surgery | 29 (10.1) | ||||
| Nonsurgery | 9 (10.7) |
a All tests were performed with univariate logistic regression. OR, P value, and AUC are based on original values and not on stratified groups. ATRS, Achilles tendon Total Rupture Score; AUC, area under the receiver operating characteristic curve; OR, odds ratio.