
Abstract
Background:
The axillary nerve is at risk during repair of a humeral avulsion of the glenohumeral ligament (HAGL).
Purpose:
To measure the distance between the axillary nerve and the free edge of a HAGL lesion on preoperative magnetic resonance imaging (MRI) and compare these findings to the actual intraoperative distance measured during open HAGL repair.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 25 patients with anterior instability were diagnosed as having a HAGL lesion on MRI and proceeded to open repair. The proximity of the axillary nerve to the free edge of the HAGL lesion was measured intraoperatively at the 6-o’clock position relative to the glenoid face. Preoperative MRI was then used to measure the distance between the axillary nerve and the free edge of the HAGL lesion at the same position. Distances were compared using paired t tests and Bland-Altman analyses.
Results:
The axillary nerve lay, on average, 5.60 ± 2.51 mm from the free edge of the HAGL lesion at the 6-o’clock position on preoperative MRI, while the mean actual intraoperative distance during open HAGL repair was 4.84 ± 2.56 mm, although this difference was not significant (P = .154). In 52% (13/25) of patients, the actual intraoperative distance of the axillary nerve to the free edge of the HAGL lesion was overestimated by preoperative MRI. In 36% (9/25), this overestimation of distance was greater than 2 mm.
Conclusion:
The observed overestimations, although not significant in this study, suggest a smaller safety margin than might be expected and hence a substantially higher risk for potential damage. We recommend that shoulder surgeons exercise caution in placing capsular sutures in the lateral edge when contemplating arthroscopic repair of HAGL lesions, as the proximity of the nerve to the free edge of the HAGL tear is small enough to be injured by arthroscopic suture-passing instruments.
Keywords
A humeral avulsion of the glenohumeral ligament (HAGL) lesion is a relatively rare but significant cause of recurrent glenohumeral instability. 3 The prevalence of HAGL lesions has been reported to be as high as 9% in patients with instability but may be even higher in older patients and young athletes participating in contact sports. 3,13 The anterior band of the inferior glenohumeral ligament (IGHL) is avulsed in 93% of HAGL lesions, 3,4,6 whereas the posterior band of the IGHL is involved in 7% of cases. 3 Both the open and the arthroscopic management of HAGL lesions require manipulation of capsular tissue, including the IGHL complex. Several authors have found that the axillary nerve has an intimate association with the inferior aspects of the glenoid and shoulder joint capsule, which may place it at risk during HAGL repair. 1,12,16
The axillary nerve is reported to be one of the most commonly injured nerves during shoulder surgery. Injuries to the axillary nerve make up 6% to 10% of all brachial plexus injuries. 7,8,11,15 As there are no large case series of surgical outcomes for HAGL repair, a definite incidence of nerve injuries has not been documented, but anecdotal discussions with colleagues indicate that there are sporadic cases of nerve injuries seen after HAGL repair but not reported in the literature.
The importance of protecting the axillary nerve during surgery to repair HAGL lesions cannot be overemphasized. Because of its extra-articular position, it remains out of the surgeon’s visual field, especially during shoulder arthroscopic surgery. Although the exact incidence of iatrogenic axillary nerve injuries during HAGL repair has not been reported, shoulder surgeons have long known that the nerve is vulnerable to damage during surgery to repair HAGL lesions. Simple attention to the potential variations in the origin and course of the axillary nerve, as well as precise knowledge of its relationship to the avulsed glenohumeral ligament, may prevent this devastating complication.
Magnetic resonance imaging (MRI) is recommended to assess the IGHL complex, the labrum, and the rotator cuff preoperatively. With a HAGL lesion, MRI demonstrates irregularity of the humeral capsular attachment on both axial and coronal oblique scans. Additional specificity is provided with magnetic resonance arthrography (MRA), which demonstrates extravasation of contrast material through the region of the capsular avulsion from the humeral neck with an expanded axillary pouch on coronal scans. 14
The aim of this study was to measure the distance between the axillary nerve and the free edge of a HAGL lesion at the 6-o’clock position on preoperative MRI and compare these findings to the actual intraoperative distance measured during open HAGL repair. This information could then be used by surgeons planning arthroscopic or open HAGL repair to minimize any potential iatrogenic damage to the axillary nerve at the time of surgery.
Methods
This study was reviewed and approved by the Macquarie University Human Research Ethics Committee (Medical Sciences). Between June 2011 and October 2015, a total of 25 consecutive patients with anterior instability were diagnosed as having a HAGL and were operated on by a senior fellowship-trained surgeon (D.J.B.). All patients underwent advanced imaging (with or without contrast) and then proceeded to open reconstruction via a single surgeon (D.J.B.) with repair of the HAGL lesion as well as any concurrent abnormalities found at the time of surgery. Data on whether imaging was performed with or without gadolinium and the presence of a Bankart lesion were collected.
Preoperative MRI scans were then analyzed to measure the distance between the axillary nerve and the free edge of the HAGL lesion at the 6-o’clock position relative to the glenoid face. This was done by marking the 6-o’clock position of the glenoid face on the sagittal MRI slices relative to the superior and inferior glenoid tubercles. This anatomic landmark was then utilized to identify the appropriate coronal slice at the 6-o’clock position on the glenoid face. Using this corresponding coronal slice on preoperative MRI, the distance between the free edge of the HAGL lesion and the axillary nerve was measured and recorded (Figure 1).

Magnetic resonance imaging showing the position of the capsular edge of the humeral avulsion of the glenohumeral ligament and the axillary nerve at the 6-o’clock position. (A) An example of the technique for measurements performed using OsiriX. Here, the distance measured was 4.6 mm. (B) Sagittal view of the same patient demonstrating the position of the axillary nerve as it passes adjacent to the inferior capsular tear.
At the time of surgery, the patient was positioned supine, and the arm was placed in 30° of abduction and neutral rotation. A deltopectoral approach was undertaken with detachment of the subscapularis from the anterior capsule. The inferior portion of the subscapularis often demonstrated scarring within the inferior muscle fibers at the site of the capsular avulsion. The axillary nerve was identified with minimal disturbance of its position as a precaution to reduce injuries. The free edge of the avulsed IGHL was dissected, and the proximity of the axillary nerve to the free edge of the capsule was then measured at the 6-o’clock position relative to the glenoid face with the use of a sterile ruler as well as a segment of suture (Figure 2). This intraoperative distance was then recorded.
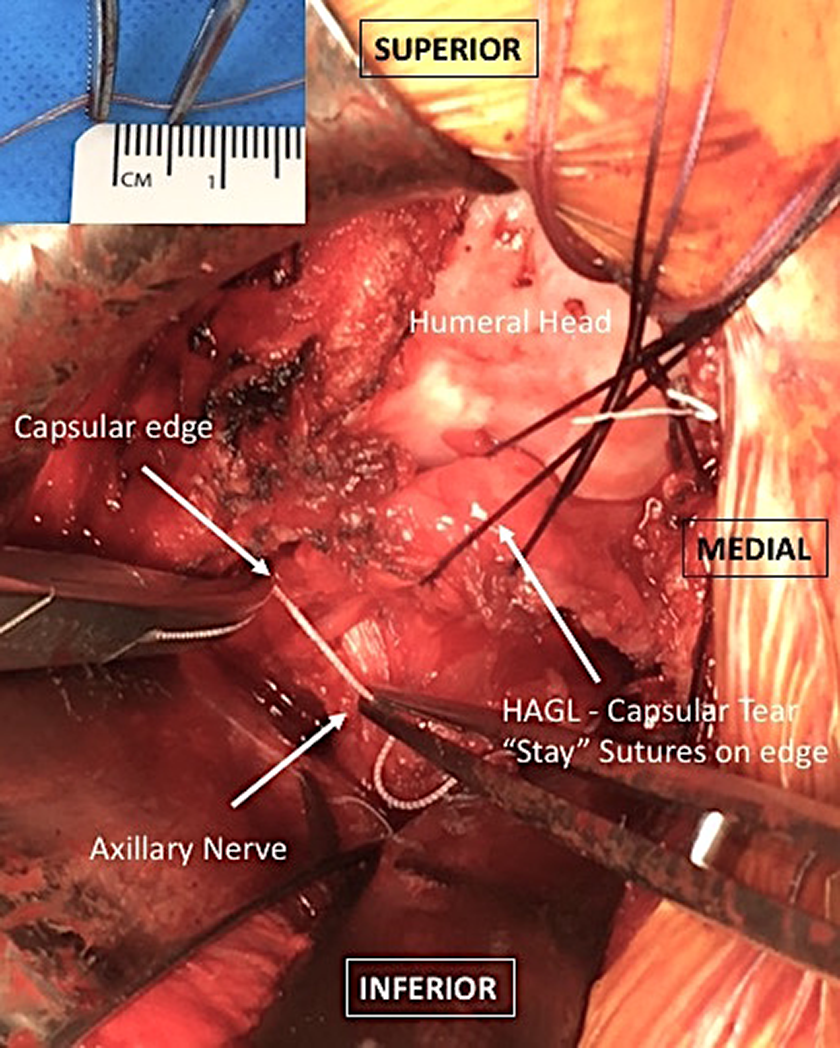
Intraoperative photograph demonstrating the technique used to measure the proximity of the axillary nerve to the capsular edge of the humeral avulsion of the glenohumeral ligament (HAGL) in the right shoulder. The free edge of the avulsed inferior glenohumeral ligament was routinely dissected during open HAGL repair. Care was taken to identify the nerve before freeing up the lateral edge of the capsule and minimize any disruption of the tissue between the nerve and capsular edge to obtain an accurate measurement of the distance between the 2 structures. The proximity of the axillary nerve to the free edge of the HAGL lesion was then measured at the 6-o’clock position relative to the glenoid face with the use of a sterile ruler and a segment of suture.
Statistical Analysis
Paired t tests were used to examine the difference between the actual intraoperative and preoperative MRI distances (ie, within-group tests). Welch 2-sample t tests were used to examine differences between covariate groups. Results are presented as count with percentage for categorical variables and mean with standard deviation for continuous variables. Bland-Altman method comparison techniques, comprising the bias (mean difference between measurement methods) and 95% limits of agreement (LOA), were used to assess the agreement between the preoperative MRI distance and the actual intraoperative distance. 2
For all analyses, a P value of <.05 was deemed statistically significant. The statistical software package R Version 3.4.3 was used for all analyses.
Results
Overall, 25 patients were included in this study, comprising 22 male and 3 female patients. The mean age at injury was 22.9 ± 10.5 years, and they had sustained a mean of 3.4 ± 3.8 dislocations before surgery. The mean time between the initial instability event and surgery was 32.7 ± 48.4 months. Of these patients, 96% (24/25) were right-shoulder dominant, with 72% (18/25) of the injuries occurring on the nondominant shoulder. At the time of surgery, 60% (15/25) were noted to have anterior labral tearing consistent with a Bankart lesion, and 12% (3/25) had a rotator cuff tear. Two of these patients underwent staged repair, with the rotator cuff undergoing initial repair using a superior approach without disturbing the region of the HAGL/axillary nerve and stabilization surgery performed approximately 6 months later, and 1 patient had the rotator cuff tear repaired at the time of HAGL surgery. Fifteen patients (60%) underwent MRA with intra-articular gadolinium.
Table 1 presents the mean difference between actual intraoperative and preoperatively imaged distances. The surgically observed distances were, on average, 0.76 ± 2.59 mm smaller than imaged measurements, although this difference was not significant (P = .154) (Table 1). Furthermore, there was no significant difference between the actual intraoperative distance and the preoperatively imaged distance in patients who underwent plain MRI (P = .566) and those who underwent MRA with gadolinium (P = .133). The mean surgically observed distance was significantly smaller than the imaged measurement for those without a concurrent Bankart lesion (P = .031) but was not significantly different for those with a Bankart lesion (P = .902).
Difference Between Actual Intraoperative Distance and Preoperatively Imaged Distance a

a LOA, limits of agreement; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging.
b Significant difference (P < .05).
Table 2 presents the mean intraoperative distance between the axillary nerve and the free edge of a HAGL lesion at the 6-o’clock position as well as the distance measured using preoperative imaging to compare MRI with MRA with gadolinium or Bankart lesion with no Bankart lesion using 2-sample t tests. There was no difference between preoperatively imaged distances using MRI versus MRA with gadolinium (P = .842) or between actual intraoperative distances for patients who underwent MRA versus MRI (P = .695). There was no statistically significant difference in the intraoperative distance (P = .236) or MRI distance (P = .549) between participants with and without a Bankart lesion.
Actual Intraoperative Distance Between the Axillary Nerve and the Free Edge of a HAGL Lesion at the 6-o’clock Position Compared With the Preoperatively Imaged Distance a

a HAGL, humeral avulsion of the glenohumeral ligament; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging.
Bland-Altman analysis using all participants is shown in Figure 3, with the bias (mean difference) and 95% LOA shown in Table 1. The line of agreement is shown by the solid horizontal black line, and the lack of agreement or bias is presented by the dashed line at −0.76 mm, indicating that the intraoperatively observed distance was, on average, 0.76 mm smaller than the preoperatively imaged distance (as noted in Table 1). Points on the plot suggest that for larger distances, the agreement becomes poorer; however, the relatively small sample size prevents a proper assessment of this. The figure also shows the 95% LOA (dashed horizontal lines at the top and bottom of the plot), which indicate that the intraoperative measurement could be as much as 4.3 mm larger to 5.8 mm smaller than the preoperative measurement. This suggests that preoperative MRI may not offer a good estimate of the expected position of the axillary nerve.
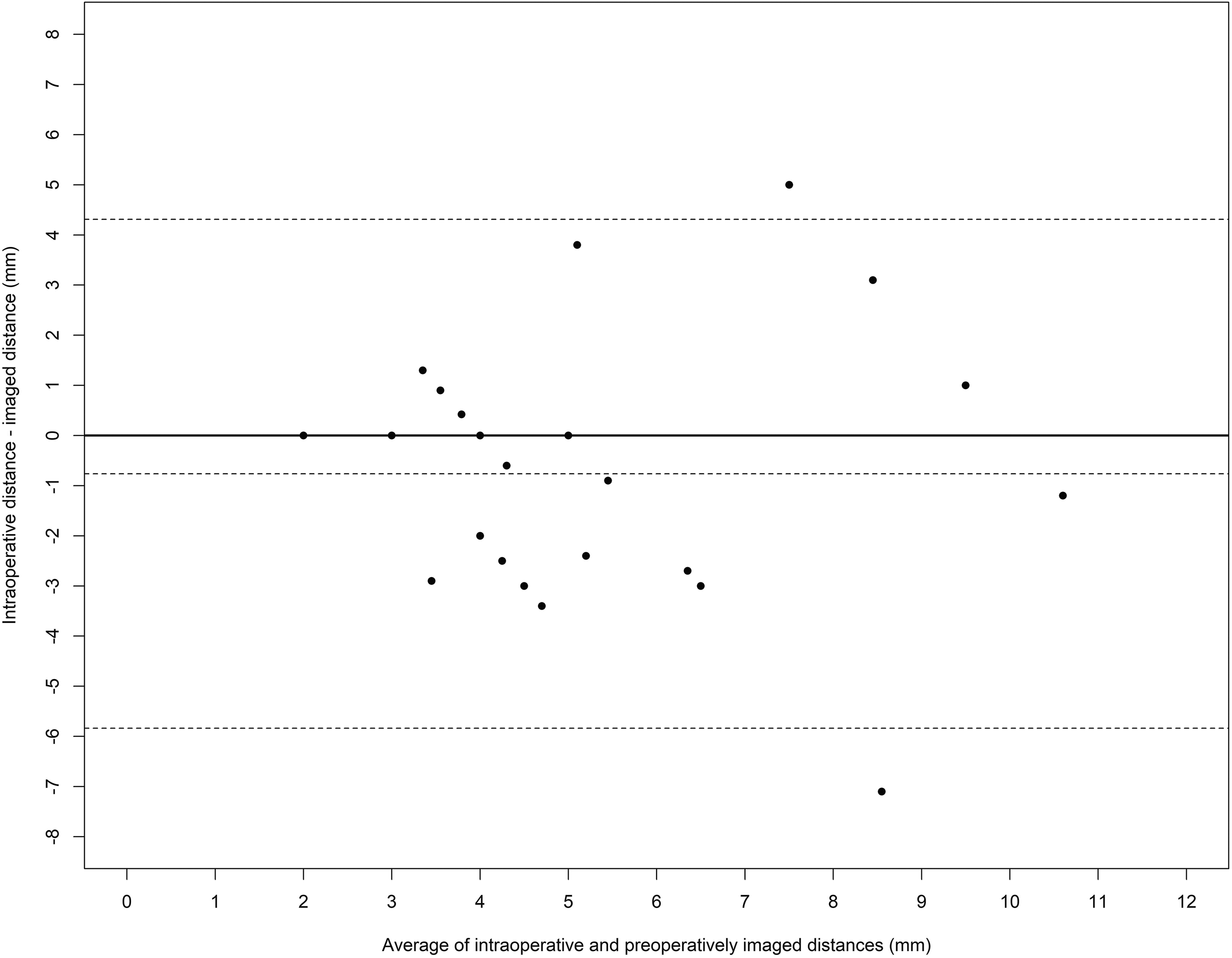
Bland-Altman analysis for all participants. Dashed horizontal lines show the mean difference (lack of agreement; center line) with 95% limits of agreement (outer lines). Solid horizontal line indicates where agreement should be located.
Table 1 also shows a summary of the agreement between methods (the mean difference is also the bias) and 95% LOA for each covariate group. The results indicate that for all subgroups, MRI overestimated the observed distance. The LOA suggest that large differences are possible in the actual intraoperative versus preoperative MRI distances between the axillary nerve and the free edge of the HAGL lesion at the 6-o’clock position relative to the glenoid face.
Discussion
Our results show that the axillary nerve lay a mean of 5.60 ± 2.51 mm from the free edge of the HAGL lesion at the 6-o’clock position on preoperative MRI, while the actual intraoperative distance during open HAGL repair was a mean of 4.84 ± 2.56 mm, although this difference did not reach statistical significance. In 52% (13/25) of patients, the actual intraoperative distance of the axillary nerve to the free edge of the HAGL lesion was overestimated by preoperative MRI. In 36% (9/25), this overestimation of distance was greater than 2 mm. These overestimations suggest a smaller safety margin than might be expected and hence a substantially higher risk for potential damage.
This is the first study to assess the proximity of the axillary nerve to the free edge of the avulsed IGHL complex in actual cases of HAGL injuries. Previous studies examining the axillary nerve about the glenohumeral joint have all been in uninjured cadaveric specimens. Price et al 12 showed that the average distance between the nerve and the inferior glenoid rim at the 6-o’clock position was 12.4 mm, but it lay even closer to the IGHL, with a relatively fixed distance of 2.5 mm throughout its course. This distance is much less than the mean distances of 5.60 mm and 4.84 mm that we measured on MRI and under direct vision, respectively. This discrepancy may be explained by the fact that our study evaluated the proximity of the axillary nerve to the free edge of the avulsed IGHL in patients as opposed to an intact IGHL in cadaveric specimens.
Yoo et al 16 determined the location of the axillary nerve in cadaveric specimens under arthroscopic conditions in the lateral decubitus position. The authors carried out arthroscopic dissection through the IGHL complex to study the course of the axillary nerve. They found that it appeared in the joint near the inferior edge of the subscapularis muscle and ran posterolaterally with a mean running angle of 23° with respect to the inferior glenoid rim horizontally, and they confirmed that the nerve was closest to the inferior glenoid rim at the 6-o’clock position. In this study, 87% (20/23) of the specimens were found to have a distance of greater than 15 mm (range, 15-25 mm) between the inferior glenoid rim and the axillary nerve in the neutral arm position, 16 far greater than the 12.4 mm reported by Price et al 12 in their cadaveric study. The distance was measured arthroscopically via the accessory superior Neviaser portal using a 5-mm premarked probe. Because accurate measurements of the distance were not possible, Yoo et al 16 categorized the closest distance of the nerve to the glenoid rim in 5-mm units. Furthermore, insufflation of the joint may have pushed the nerve farther away from the rim. An interesting finding in the Price et al 12 study was the fact that abduction–neutral rotation was the optimal position for minimizing axillary nerve injuries because it resulted in the greatest distance between the inferior glenoid and the nerve.
Although the exact incidence of iatrogenic axillary nerve injuries during HAGL repair is unknown, shoulder surgeons have long been aware that the nerve is vulnerable to damage during surgery to repair HAGL lesions.
There are various descriptions of arthroscopic techniques for HAGL repair in the literature. 5,9,10 Surgeons use various techniques, arthroscopic graspers, and other instruments to facilitate suture passage through the IGHL complex. Two such instruments are the Scorpion (Arthrex) and Spectrum (Conmed) (Figure 4). Both these instruments have dimensions that may place the axillary nerve at risk during arthroscopic HAGL repair. In using these and any other suture-passing device, the surgeon needs to be acutely aware of the dimensions of the jaws and the radius of curvature of the tip to ensure careful placement of sutures on the capsular edge. The dimensions for the greatest depth of passage of these suturing devices may be significantly greater than the measured proximity of the axillary nerve to the free capsular edge that we report here. Furthermore, as the surgeon places pressure on the instrument to facilitate passage through tissue, he or she may distort the local anatomy and draw the capsular edge closer to the axillary nerve.

Examples of arthroscopic suture-passing instruments. (A) The Scorpion (Arthrex) suture passer has a 17-mm jaw length with a 13-mm aperture. Using this instrument, the surgeon needs to be cautious to not pass the jaws too deep to minimize capture of the axillary nerve. (B) The Spectrum (Conmed) 45° suture passer has a radius of curvature of 7 mm, and the surgeon may penetrate deeper than expected when applying force to perforate the capsular edge, again endangering the axillary nerve.
There are limitations to this study. Because all measurements on imaging (with or without contrast) were taken once and the actual intraoperative distance was measured once only by a single surgeon at the time of the surgical procedure, interobserver and intraobserver reliability could not be assessed. The intraoperative measurements of the actual distance between the free edge of the HAGL lesion and the underlying axillary nerve may be affected by the surgical dissection required for exposure, although every attempt was made to identify the capsular edge and the position of the nerve as early as possible to minimize any subsequent tissue displacement.
Conclusion
The importance of protecting the axillary nerve during surgery to repair HAGL lesions cannot be overemphasized. In the current study, the axillary nerve lay closer to the free edge of the HAGL lesion (4.84 mm) than preoperative MRI suggested (5.60 mm) at the 6-o’clock position. Despite the lack of a significant difference between the distance measured on preoperative MRI and the actual intraoperative distance during open repair, in 52% of cases, the actual distance of the axillary nerve to the free edge of the HAGL lesion was overestimated by preoperative MRI, and in 36% of cases, MRI overestimated the distance by more than 2 mm. These overestimations suggest a smaller safety margin than might be expected and hence a substantially higher risk for potential damage. Considering these findings, we recommend that shoulder surgeons exercise caution when contemplating arthroscopic repair of HAGL lesions, as the proximity of the nerve to the free edge of the HAGL tear is small enough to be injured by arthroscopic suture-passing instruments.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.B. is a consultant for Smith & Nephew, Rotation Medical, Zimmer Biomet, Wright Medical, and Allegra Orthopaedics and owns stock/stock options in Allegra Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Macquarie University Human Research Ethics Committee (No. 5201500889).