
Abstract
Background:
Dynamic compressive neuropathies around the elbow are a rare entity described by a relatively small body of literature, mostly consisting of single-case reports. No standardized diagnostic protocols have been described to date. To the authors’ knowledge, this study represents the largest case series of dynamic compressive neuropathies in the upper extremity.
Purpose:
To identify various etiologies of dynamic compressive neuropathies around the elbow, devise a systematic diagnostic protocol, and review treatment options.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review was conducted of patients who presented to a single practice between 2013 and 2017 and were diagnosed with a dynamic compressive neuropathy around the elbow.
Results:
A total of 7 patients were identified, with a mean follow-up of 2 years. All patients were high-level pitchers. One patient was a minor league pitcher; 4 patients were National Collegiate Athletic Association athletes; and 2 patients were high school athletes. All patients underwent a systematic diagnostic workup. The diagnosis was established with dynamic nerve conduction testing. Three etiologies for dynamic nerve compression around the elbow were identified: 1 case of lateral antebrachial cutaneous nerve compression by the biceps tendon, 3 cases of ulnar nerve compression by an anconeus epitrochlearis muscle, and 3 cases of posterior interosseous nerve compression at the arcade of Frohse with hypertrophic extensor carpi radialis brevis and extensor digitorum communis muscles. Two patients were treated conservatively, while 5 patients required surgery. All patients were able to return to pitching.
Conclusion:
Dynamic compressive neuropathies around the elbow are rare entities that present unique diagnostic challenges to the treating clinician. In this cohort, all patients were young throwing athletes. Physical examination of the patient frequently lacks typical findings of chronic nerve entrapment syndromes. Dynamic nerve conduction studies establish the diagnosis, and treatment often requires surgical decompression to achieve complete resolution of symptoms.
Keywords
Chronic nerve compression and entrapment syndromes in the upper extremity are commonplace; however, the same cannot be said about dynamic compressive neuropathies. 3 Compressive neuropathies can occur at any point over the course of a nerve, and failure to treat the underlying pathology can lead to altered or even irreversible changes in function. These functional alterations are often the initial presenting signs of a compressive neuropathy, precipitated by pain and paresthesias, and are particularly troublesome for high-level pitchers. Pitching is a complex process based on a kinetic chain that starts with the lower extremity and courses through the entire body up to the finger tips at the point of release. An alteration of the kinetic chain of the pitcher attributed to a compressive neuropathy will affect athletic performance and increase stresses on the surrounding anatomy, possibly accelerating the potential for overuse injuries. 1 Early diagnosis and treatment are therefore critical in treating pitchers with compressive neuropathies.
Compressive neuropathies classically occur as a nerve passes through a fibro-osseous space, such as the cubital tunnel, leading to chronic and slowly progressive symptoms. In our case series, however, we identified 3 etiologies of dynamic nerve compression syndromes of the elbow among high-level pitchers. We refer to dynamic compressive neuropathies as entities with specific activity-dependent onset and resolution, which lack the “classic” progressive and chronic clinical course. A lack of standardized diagnostic protocols makes dynamic nerve compression syndromes a particularly challenging diagnosis. Current literature is scarce and based on single-athlete case reports. 2,4,7 –9 To our knowledge, this is the largest case series of dynamic compressive neuropathies described in the literature to date.
The aim of our study was to identify potential etiologies of dynamic nerve compression syndromes of the elbow and devise a standardized diagnostic protocol to aid the clinician in the workup and treatment of these diagnostically challenging entities.
Methods
This is a retrospective review of all patients with a dynamic compressive neuropathy of the elbow who presented to our clinic between 2013 and 2017. Accurate diagnoses were achieved per a stepwise workup: a thorough history corroborated an absence of symptoms at rest and an onset of symptoms with activity that resolved upon cessation of the offending action. The history suggested the particular nerve that was being compressed, commonly due to a distinct dermatomal distribution. Cases of posterior interosseous nerve (PIN) compression presented with temporary wrist and finger extension weakness accompanied by more generalized forearm pain. A complete physical examination of the upper extremity, pre- and postactivity, was performed to identify the affected nerve; radiographic evaluation of the elbow was ordered to rule out more common etiologies of pain and/or paresthesias; high-resolution magnetic resonance imaging (MRI) was conducted to further evaluate the patient’s anatomy around the elbow; and last, dynamic nerve conduction studies (dNCSs) were used to establish the diagnosis (Figure 1).

Proposed diagnostic protocol. dNCS, dynamic nerve conduction study; MRI, magnetic resonance imaging.
The dNCSs were performed by a single neurologist on the same equipment for all athletes. To obtain dNCSs, a baseline pre-exercise study was obtained in the nerve distribution that was affected based on the aforementioned workup; after baseline conduction velocities and latencies were obtained, the athletes were instructed to perform the offending activity (ie, pitching) until the onset of symptoms. An immediate postexercise nerve conduction study was performed and compared with baseline. The diagnosis was considered established if the postexercise nerve conduction velocities and latencies mimicked the parameters used to establish the classic, static compressive neuropathies, such as cubital tunnel syndrome, in the setting of normal pre-exercise results per the report of the neurologist performing the study. 6
Conservative management consisted of activity modification, including a temporary cessation of pitching activity for 2 weeks, with gradual rehabilitation to normal activity levels as determined by the patient in conjunction with the athletic trainer. Furthermore, neoprene sleeve bracing to support the elbow and incentivize the athlete to rest it, in combination with injections of lidocaine with betamethasone acetate, was utilized to potentially combat inflammation-mediated swelling of the nerve and/or surrounding tissues. We typically used 4 mL of 1% lidocaine and 1 mL of betamethasone acetate (3 mg/mL) per injection. The injection was placed as close as possible to the likely point of compression, such as the arcade of Frohse. In patients who failed conservative management, surgical exploration and decompression of the affected nerve were performed.
Results
Seven patients between the ages of 14 and 23 years were identified, all of whom were high-level pitchers. The mean patient age was 18 years, and the mean follow-up was 24 months. One athlete was a minor league player, 4 were National Collegiate Athletic Association (NCAA) athletes, and 2 were high school athletes.
Three etiologies of dynamic nerve compression were identified: a single case of musculocutaneous nerve entrapment between the biceps brachii and brachialis muscles, 3 ulnar nerve compressions attributed to dynamic enlargement of an anconeus epitrochlearis, and 3 cases of dynamic compression of the PIN at the arcade of Frohse (Table 1). 5,9,10
Dynamic Compressive Neuropathy Etiologies a

a ECRB, extensor carpi radialis brevis; EDC, extensor digitorum communis; LABC, lateral antebrachial cutaneous.
On physical examination, a positive provocative test/Tinel sign could be elicited in all cases of ulnar and radial nerve entrapment after the offending activity (ie, pitching) was performed until the patient became symptomatic. Physical examination before the offending activity was performed or >1 hour after the offending activity was halted yielded normal results. The lateral antebrachial cutaneous (LABC) nerve entrapment did not have a positive provocative test even when performed immediately after cessation of the offending activity; however, the clear dermatomal distribution of the pain as described by the patient was consistent with an isolated LABC nerve compressive neuropathy.
Radiographic evaluation results of all 7 patients were normal. MRI revealed a hypertrophic anconeus epitrochlearis muscle in all 3 patients with a dynamic ulnar nerve compressive neuropathy, but results were normal for the remaining 4 patients.
The dNCSs showed a mean increase in postexercise latency of 28% when compared with baseline pre-exercise latencies. It took a minimum of 20 pitches and no more than 50 pitches to evoke symptoms in our cases. Injections with lidocaine and betamethasone acetate did not prove to be helpful as part of the diagnostic workup.
All patients underwent initial conservative treatment. Two patients, both of whom displayed symptoms of dynamic PIN compression, achieved return to play with conservative treatment alone. The first was an NCAA pitcher. Activity modification consisted of a brief period of pitching cessation for 2 weeks, followed by closely supervised rehabilitation as determined by the athletic trainer and pitching coach. The second patient, a high school pitcher, achieved incomplete resolution of symptoms. After consultation with the patient and his parents, he felt that he experienced a sufficient degree of improvement to return to play, for which he was cleared.
For the remaining 5 patients, conservative treatment unfortunately did not yield satisfactory improvement of their symptoms, necessitating surgical decompression of the affected nerve.
All surgery was undertaken by the same surgeon (G.M.L.). The first patient required surgical release of the LABC nerve with a partial biceps tendon excision for a dynamic compression of the LABC nerve as it emerged from lateral to the biceps tendon and brachioradialis (Figure 2, Video Supplements 1 and 2).
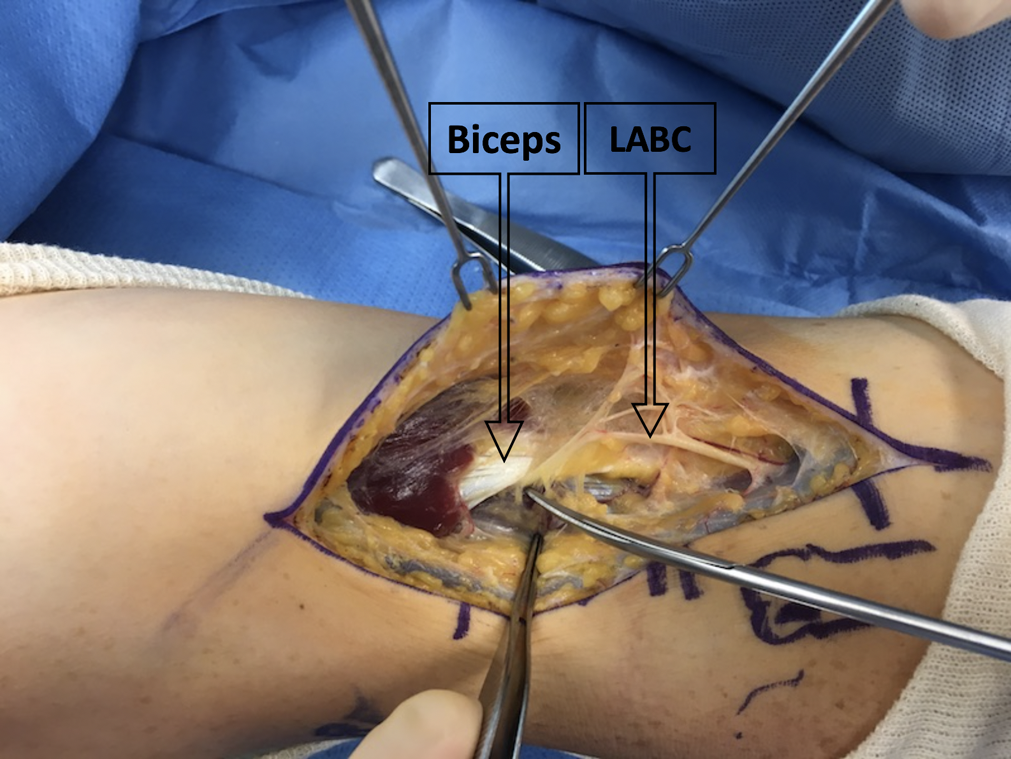
The dissection scissors point to the lateral antebrachial cutaneous (LABC) nerve exiting underneath the biceps brachialis tendon in supination. Entrapment is exacerbated by pronation, as demonstrated in Video Supplement 1.
The second patient underwent a radial tunnel release with debridement of hypertrophic extensor carpi radialis brevis and extensor digitorum communis muscles for dynamic compression of the PIN and posterior cutaneous nerve. The 3 remaining patients requiring surgery all underwent in situ decompression of the ulnar nerve with excision of the anconeus epitrochlearis, which was present in all 3 cases of dynamic ulnar nerve compression, and neurolysis of the posterior branch of the medial antebrachial cutaneous nerve. No nerve transpositions were necessary in our case series. All 5 patients who underwent surgical decompression achieved complete resolution of their symptoms and returned to pitching activity. Time frames for return to play were variable, but we typically kept the patient immobilized for the first 4 weeks postoperatively. After the 4-week mark, a removable splint was applied, and passive range of motion exercises were initiated. At postoperative 6 weeks, full active range of motion exercises were started, strengthening at 10 weeks, and baseball-related activities at 12 weeks after the index procedure.
Discussion
The overall incidence or prevalence of dynamic nerve compression syndromes in the upper extremity is unknown. Case reports suggest that the elbow and shoulder girdle are the most common locations and that athletes performing overhead activities, such as pitching or serving, are at highest risk. In our case series, all individuals were young male pitchers. All patients experienced a significant decrease in their athletic performance owing to the onset of pain and paresthesias when pitching. Several factors differentiate dynamic from chronic nerve compression and entrapment syndromes around the elbow during a history and physical examination: Patients report a more severe and rapid onset of symptoms in the dynamic compression syndromes. Pain is often the initial presenting symptom, not paresthesias. The pain tends to be more severe and located over the area of the compressive lesion (eg, overlying the cubital tunnel in the case of a symptomatic anconeus epitrochlearis), instead of distal to it. The quality of pain is sharp and burning, consistent with neurogenic pain versus the more dull and aching myofascial pain often experienced by athletes after strenuous exercise. Patients with dynamic nerve compressive syndromes experience a complete resolution of their symptoms often within minutes of stopping the offending activity. None of our patients reported night symptoms. The physical examination is challenging, as virtually all classic findings indicative of nerve compression—such as atrophy, clawing, a decrease in sensation, motor weakness, and provocative tests—are negative in the clinic. We have found that provocative tests, such as the Tinel sign, may be positive if the patient is performing the offending activity until symptomatic; as such, an examination of the patient during practice is required, rather than one in the clinic. We have found that, given the relatively benign nature of the physical examination in our patient cohort, a thorough history with the patient describing the location, quality, and distribution of pain and paresthesias is the most important factor in identifying the particular nerve that is affected.
Imaging studies are an important aspect of accurately diagnosing the etiology of dynamic nerve compression syndromes. A basic 3-view radiographic evaluation of the elbow was performed in all patients. Patients who appeared to have symptoms stemming from the ulnar nerve or cubital tunnel also received a cubital tunnel view radiograph to better assess the osseous anatomy. The primary purpose of the radiographic evaluation was to rule out other potential causes for compressive neuropathies, such as traumatic injuries, tumors (especially osteochondromas and synovial osteochondromatosis), or disease processes (eg, myositis ossificans). 11 In our cohort of patients, all radiographic results were normal. In the absence of pertinent radiographic findings, high-resolution MRI was performed to visualize soft tissue anatomy and rule out occult fractures. Four patients had unremarkable MRI scans; however, 3 patients with dynamic compression of the ulnar nerve had a hypertrophic anconeus epitrochlearis—the presence of which is normal in 34% of patients but has been described as the potential cause of ulnar nerve neuropathy, especially among throwing athletes. 4,9
The most useful diagnostic tool in our case series was the dNCS, underlining the importance of a well-integrated interdisciplinary approach in the diagnosis and treatment of patients with dynamic compressive neuropathies. Baseline dNCS results at rest were normal for all patients. However, repeat dNCSs after the patient performed the offending activity until the onset of symptoms showed an increase in latency and decrease in nerve conduction velocities. Unfortunately, given the rarity of dynamic compressive neuropathies, no good data exist to determine precise diagnostic cutoff values for dNCSs; however, values established for the diagnosis of classic, static compressive neuropathies may be used as a guide. Based on this relative ambiguity, a close relationship with a neurologist well trained in performing and interpreting electrodiagnostic studies is critical. In our cases, all patient had changes in their dNCSs of a magnitude sufficient enough to rule out intraobserver variability, temperature changes, or other ambient factors that may influence electrodiagnostic studies. This was true for purely sensory nerve compression, such as the LABC nerve in 1 patient, as well as mixed nerves, such as the ulnar nerve. The presence of abnormal immediate postexercise dNCSs versus normal baseline studies was considered diagnostic of dynamic compressive neuropathies.
Injections with lidocaine and betamethasone have not proven to be helpful in the diagnostic workup. We hypothesize that this is likely due to the dynamic compressive neuropathy being caused by a temporary microcirculatory compromise of the affected nerve rather than an inflammatory process. However, since we cannot rule out at least a partial contribution of inflammatory-mediated nerve and soft tissue swelling to the overall symptomatology, we continue to utilize injections as part of our conservative management to maximize potential resolution of the compressive neuropathy.
Conservative management with injections, activity modification, and bracing was successful in the treatment of 2 patients with dynamic compression of the radial nerve at the arcade of Frohse and might be a useful tool in the clinician’s armamentarium for patients reluctant to undergo surgery. Surgical treatment, consisting of fascial releases, muscle debulking, and neurolysis, was successful in achieving a complete resolution of the symptoms and return to play for all 5 patients who failed conservative treatment.
Given the rarity of the described entities, it is difficult to hypothesize about potential preventative strategies. All patients were under the care of professional athletic trainers and coaching staff, with close supervision of their training, making improper training habits an unlikely source of the problem. What we hope to achieve with this publication is to raise awareness of the existence of dynamic compressive neuropathies and to facilitate an early and accurate diagnosis in an effort to prevent a potential injury to the athlete because of an unintended alteration in the pitching mechanics that puts the elbow at risk of harm.
Limitations
The main limitation of the study is its retrospective design. The rarity of the investigated pathology also causes our cohort to be underpowered to draw epidemiologic conclusions, although we believe this to be the largest case series of dynamic compressive neuropathies in the upper extremity to date. We did not track the progress of our patients with standardized outcome measures, such as the DASH (Disabilities of the Arm, Shoulder and Hand) score. It is also difficult to draw definitive conclusions about treatment algorithms, given the potential of differential responses to various treatments among the 3 identified nerves.
Conclusion
Dynamic nerve compression syndromes of the elbow are a rare entity that may be seen among young throwing athletes. An accurate diagnosis should be based on exclusion of more common etiologies. We propose a workup consistent of a history that confirms a dynamic symptomatology and suggests entrapment of a specific nerve. Physical examination of the suggested nerve is benign at rest, but a positive provocative test may be elicited if performed immediately after the offending activity is performed for a sufficiently long-enough time to elicit symptoms. Diagnostic injections have not proven to be useful. Radiographs followed by a high-resolution MRI should be obtained to assess the patient’s anatomy, and then dNCSs should be undertaken to confirm the diagnosis. The success of the workup depends on an integrated approach by the treating surgeon, radiologist, and neurologist. Successful treatment may be achieved through conservative measures, but our experience has shown that higher level athletes often require surgery to achieve complete resolution and an ability to return to play.
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/2325967118807131.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the WellStar Atlanta Medical Center Institutional Review Board/Privacy Board.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.