
Abstract
Background:
Osteochondral allograft (OCA) transplantation has become a standard therapy for cartilage restoration in young patients.
Purpose:
To determine the efficacy of fresh OCA transplantation for focal cartilage lesions in patients aged ≥40 years compared with a group of patients aged ≤39 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A database was used to identify patients who underwent fresh OCA transplantation in the knee in a single-surgeon practice over a 10-year period and who completed baseline patient-reported outcome (PRO) questionnaires, including the International Knee Documentation Committee (IKDC); Knee injury and Osteoarthritis Outcome Score (KOOS) subscales of Pain, Symptoms, Activities of Daily Living, Quality of Life (QOL), and Sports & Recreation; and Veterans RAND 12-Item Health Survey (VR-12). Patients who completed the same PRO measures at a minimum 12-month follow-up were categorized into 2 groups based on age at surgery and were observed longitudinally. Mixed-model regression was used to predict longitudinal growth curves for each PRO score while controlling for confounding patient and surgical variables.
Results:
The study group consisted of 38 patients with a mean age of 52.32 years (range, 40-69 years) and mean final follow-up of 44.47 ± 24.32 months. The control group consisted of 42 patients with a mean age of 27.19 years (range, 15-39 years) and mean final follow-up of 33.75 ± 19.53 months. A statistically significant improvement from baseline to final follow-up was seen for the IKDC score and all 5 KOOS subscores in both the study and the control groups (P < .01 in 10 of 12 comparisons and P < .05 for the other 2 comparisons). Maximum improvements were seen in the KOOS QOL and Sports & Recreation subscores for both groups. There was no statistically significant difference between groups in the change from baseline to final follow-up or in differences at any time point in model-based longitudinal projections for any PRO score through 5 years.
Conclusion:
There was a significant improvement of outcomes for both groups, with no statistically significant difference between groups over longitudinal follow-up. The efficacy of fresh OCA transplantation in adults aged ≥40 years with a focal chondral lesion and without osteoarthritis is similar to that of younger adults, and benefits are greatest for the KOOS QOL and Sports & Recreation subscales, which reflect functional outcomes.
Patients with full-thickness cartilage defects of weightbearing joints experience pain, dysfunction, and the risk of progression toward osteoarthritis if they do not undergo surgical intervention because articular cartilage lacks the intrinsic capacity for regeneration. While surgical cartilage repair or restoration remains a clinical challenge, fresh osteochondral allograft (OCA) transplantation is an increasingly available and accepted therapy for the biological replacement of damaged cartilage and underlying bone. Historically, OCA transplantation has been reserved for larger cartilage lesions (>2.5 cm2), for lesions with substantial underlying bone loss, and as a secondary treatment option after a previous failed cartilage procedure. 5 Long-term follow-up and meta-analyses from pooled cohort studies have demonstrated favorable clinical outcomes, high patient satisfaction, and low failure rates from 18% to 25%. 3,4 While most cell-based and biological therapies for cartilage repair have failed to both re-create a hyaline cartilage phenotype and integrate into surrounding healthy tissues, OCAs overcome these challenges. 5 Specifically, the graft fills the defect with mature hyaline cartilage capable of withstanding and contributing to the biomechanical function of the joint, and the underlying bone of the graft integrates and anchors into the surrounding osseous bed.
Previous studies have evaluated causes of injury, prior surgery, concomitant procedures, graft location, and patient sex as confounding variables with respect to patient-reported outcome (PRO) and failure analyses. 4,10,14,15 Taken together, these studies demonstrate that young and active patients with an isolated condylar lesion have high success rates regardless of prior failed cartilage restoration. Thus, OCA transplantation represents a commonly performed treatment option for large chondral injuries in pediatric and adolescent populations, with 90% graft survivorship and 88% patient satisfaction after 10 years. 12 Among high-level athletes in younger populations (mean age, 31.2 years), the procedure has resulted in 75.2% returning to high-level activity, 13 which is often a primary outcome for younger athletic patients.
While there is a high prevalence of focal cartilage damage in the knee in young active populations with athletic injuries, cartilage lesions are quite common among all patients undergoing arthroscopic surgery. According to several large cohort studies with an average patient age between 39 and 43 years across studies, 2,6,16 the prevalence of cartilage lesions was approximately 60%. Widuchowski et al 16 reported that 58% of chondral injuries were sustained by traumatic noncontact causes during either activities of daily living (45%) or sports participation (46%); in total, 67% of lesions were focal osteochondral or chondral lesions, 29% were osteoarthritic lesions, and 2% were osteochondritis dissecans (OCD) lesions. Curl et al 6 reported that 19.2% and 41% of chondral injuries were Outerbridge grades 3 and 4, respectively, which warrants restoration procedures such as osteochondral transplantation. These studies indicate that focal cartilage lesions are common across all patients with knee injuries; however, OCA transplantation has primarily been indicated and studied in the context of populations younger than 40 years based on historical indications covered by insurance reimbursement.
It was not until recently that investigators considered age as a possible risk factor for OCA treatment failure. Poorer patient-reported pain outcomes have been attributed to many confounding factors, including preexisting or concurrent lesions, primarily osteoarthritis, and a historical lack of treatment options for middle-aged patients. 9 Aside from age, both a greater number of prior surgeries and a higher body mass index (BMI) are identified risk factors for OCA transplantation failure. These risk factors are likely also confounding variables because older patients are more likely to have undergone other primary operative procedures and tend to have a higher BMI on average. While younger patients usually have isolated chondral defects after an acute injury, older patients generally present with chronic and more diffuse chondral defects from a nontraumatic cause. 16 With that said, there is also a distinct population of older patients who present with focal cartilage defects and may be candidates for cartilage restoration therapy. Recent data suggest that OCA transplantation in adults older than 40 years has equivalent outcomes to those of younger patients and may be a reliable interim treatment for cartilage defects in the knee to delay total joint replacement. 8,15
The purpose of this study was to validate the efficacy of OCA transplantation in patients aged ≥40 years, in comparison with patients aged ≤39 years, by PRO scores, with a focus on functional outcomes. We sought to validate the results of recent studies, 8,15 to confirm the efficacy of OCA transplantation in older populations using predictive modeling with regression adjustments to identify the isolated effect of age on functional outcomes. We hypothesized that patients aged ≥40 years would experience a comparable benefit with younger patients after fresh OCA transplantation in the knee based on proportional differences in goals of care and functional outcomes.
Methods
Patient Selection and Outcome Measures
Approval was obtained from the institutional review board at Oregon Health & Science University to collect and manage PRO scores and demographics in a prospective longitudinal database (SOCRATES; Ortholink). All patients who presented to the clinic of the primary surgeon (D.C.C.) at a tertiary referral center consented to participate in reporting outcomes to the database for potential future use in retrospective studies. The database was queried to identify patients who had undergone fresh OCA transplantation in the knee in the primary surgeon’s practice between March 2007 and January 2017. Inclusion criteria were patients who provided baseline PRO scores and completed the same PRO measures at least 1 year past the date of the index surgery. OCA transplantation indications were patients with a ≥2-cm2 grade 4 International Cartilage Repair Society (ICRS) lesion to the medial and/or lateral femoral condyle and/or trochlea and/or patella and with pain and/or dysfunction directly attributable to this injury or condition. A chart review of electronic medical records was subsequently conducted to collect patient demographics and surgical variables for eligible participants.
Eligible patients were categorized into 2 groups based on age at the time of surgery. The study group consisted of patients who were ≥40 years of age, and the control group consisted of patients who were ≤39 years of age at the time of the index surgery. Preoperatively, each patient completed baseline PRO measures, including the Knee injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee (IKDC), and Veterans RAND 12-Item Health Survey (VR-12). Questionnaires were administered either in person during clinical postoperative visits or through a link emailed to the patient directly from the SOCRATES PRO management database. Any subsequent surgery in the knee after the index procedure was documented at this time. A reoperation was defined as any surgery on the ipsilateral knee. Allograft failure was defined as any procedure that removed or revised the allograft, including unicompartmental or total knee arthroplasty. Outcome scores were routinely collected at 6 months, 12 months, and annually thereafter. Patients who completed preoperative questionnaires but did not complete any postoperative questionnaires were considered lost to follow-up and were included as a third group in the analysis.
Surgical Treatment and Rehabilitation
Fresh OCA tissue was obtained from JRF Ortho. Tissue was aseptically harvested from cadaveric donors aged 12 to 39 years and stored at 4°C in a proprietary nutrient medium. The tissue was implanted between 18 and 28 days postmortem. The surgical technique involved minimally invasive (no patellar eversion) paramedial and/or lateral arthrotomy based on the location of the defect. The area of injury was exposed, and the size and extent of the pathological tissue were estimated. All lesions underwent press-fit fixation after debridement and host site preparation. A press-fit dowel graft was created from the allograft donor tissue and placed using a well-described technique that provided the most congruous surface tailored for press fitting from the available transplant source. 17
Postoperatively, patients were allowed to immediately bear weight as tolerated in a knee brace locked in extension during recovery from continuous femoral regional nerve block (3-4 days). Unrestricted active and passive ranges of motion were encouraged while nonweightbearing; a continuous passive motion device was not prescribed. After sutures were removed at 10 to 14 days, the patient was allowed to bear weight as tolerated with full range of motion.
Statistical and Data Analyses
The Welch t test was used to compare the mean time to final follow-up, and the Fisher exact test was used to assess differences for completeness of each PRO measure at 2 years between age-based groups. Demographic and surgical variables were compared between each of the 3 groups (≥40 years, ≤39 years, lost to follow-up) using the Welch t test or robust 1-way analysis of variance (ANOVA) for means and the Fisher exact test for counts. Differences in baseline PRO scores were assessed using robust 1-way ANOVA. The Welch t test was used to assess differences in the change from baseline to final follow-up between groups for each PRO score. The longitudinal trajectories for PRO scores over time for each group were modeled with nonlinear regression modeling, in which the best-fitting curve to describe the mean growth trend within each group was found to be a logarithmic transformation of the number of months after surgery.
As the measurements for a single patient are repeated across time points, there is an expectation that scores measured close in time to one another are positively correlated because of their proximity. There is also likely to be some overall convergence to a stable final value across the entire follow-up. These sources of correlation can be modeled as an exponential decay of correlation between adjacent measurements, in which the rate of decay is estimated as a parameter and the amount of decay is calculated as a function of the time interval between the measurements.
The variability of individual trajectories was addressed by the use of regression adjustment to the growth curves. A mixed-model regression framework was used to adjust for offset of age at surgery from the mean age for the group (ie, age offset from 27.19 years in the ≤39-year group and from 52.32 years in the ≥40-year group), BMI at surgery, sex (male or female), size of the lesion (maximum size in the case of more than 1 lesion), prior surgery (yes or no), and whether surgery involved 1 or 2 grafts. These adjustments may reflect sources of confounding due to patient characteristics and disease severity characteristics as well as the possibility of sex bias in the reporting of outcomes.
Power was quantified in terms of the minimum detectable effect size, which was defined as a fraction of the pooled baseline SD that could have been declared significant at a power of 80% and alpha level of 0.05 with the given sample sizes. The target for effect size was the time-averaged difference in outcome means between the younger and older groups, scaled by the baseline SD and based on the assumed autocorrelative residual structure in the response model. Statistical power calculation was performed using the “Tests for Two Means in a Repeated-Measures Design” module in PASS (version 15; www.ncss.com/software/pass/), with the autocorrelation value set to 0.7, representing the average autocorrelation across all PRO measures.
Results
Of the 118 patients who met the inclusion criteria, 80 eligible patients completed PRO measures at a minimum of 9 months (78/80 had at least 12 months). Completed PRO scores at ≥2-year follow-up were obtained for 34 of 42 (81%) of the control group and 33 of 38 (87%) of the study group; the difference in loss to follow-up between groups was not significant (P = .476). The follow-up duration tended to be longer for the older group, but the groups were similar in 2-year PRO completeness. The study group consisted of 38 patients, 10 women and 28 men, with a mean age of 52.32 ± 8.46 years (range, 40-69 years) and a mean final follow-up of 44.47 ± 24.32 months (range, 12-119 months) (Table 1). The control group consisted of 42 patients, 27 men and 15 women, with a mean age of 27.19 ± 7.13 years (range, 15-39 years) and a mean final follow-up of 33.75 ± 19.53 months (range, 9-83 months). The group of 38 patients that was lost to initial follow-up (ie, they did not complete postoperative questionnaires) was of intermediate age (8 patients were ≥40 years old) in comparison with the other groups, but they did not differ with respect to any other demographic variable. Age was the only demographic variable that was significantly different between the study and control groups.
Continuous Patient Demographics and Surgical Parameters a

a Data are presented as mean ± SD unless otherwise indicated.
b Welch t test or robust 1-way analysis of variance for mean values and Fisher exact test for count values.
Previous surgical treatment had been performed on 31 of 38 knees (82%) in the study group and 37 of 42 knees (88%) in the control group; this was most commonly loose body removal, chondroplasty, or microfracture for both groups. Aside from these prior procedures, 1 patient in the study group had previously undergone osteochondral autograft transplantation, while 10 patients in the control group had undergone prior osteochondral autograft transplantation or open reduction internal fixation of an OCD lesion. The most common underlying cause of the lesions in both the study and the control groups was OCD at 39% and 64%, respectively (Table 2). The preoperative diagnosis and lesion location/surgical site were significantly different between the study and control groups. In the study group, the medial femoral condyle was the most frequently grafted site (66%), whereas the lateral femoral condyle was the most frequently grafted site (50%) in the control group. The group that was lost to follow-up had a greater proportion of patients with a preoperative diagnosis of avascular necrosis or prior microfracture failure, as well as a greater proportion of patellar or trochlear lesions, in comparison with either the study or control group.
Categorical Patient Demographics and Surgical Parameters a

a Data are presented as n (%). LFC, lateral femoral condyle; MFC, medial femoral condyle.
b Fisher exact test.
A single allograft dowel was transplanted in 68% of the study group and in 71% of the control group, with the remaining patients receiving multiple grafts per lesion. In total, 46% of patients underwent concomitant procedures. Of the 38 knees in the study group, 17 (45%) underwent additional procedures during the index surgery, with the most common being arthroscopic meniscectomy (Table 3). In comparison, 20 (48%) of the 42 knees in the control group underwent concurrent procedures, with loose body removal accounting for the majority.
Concomitant Procedures Performed With Osteochondral Allograft Transplantation a
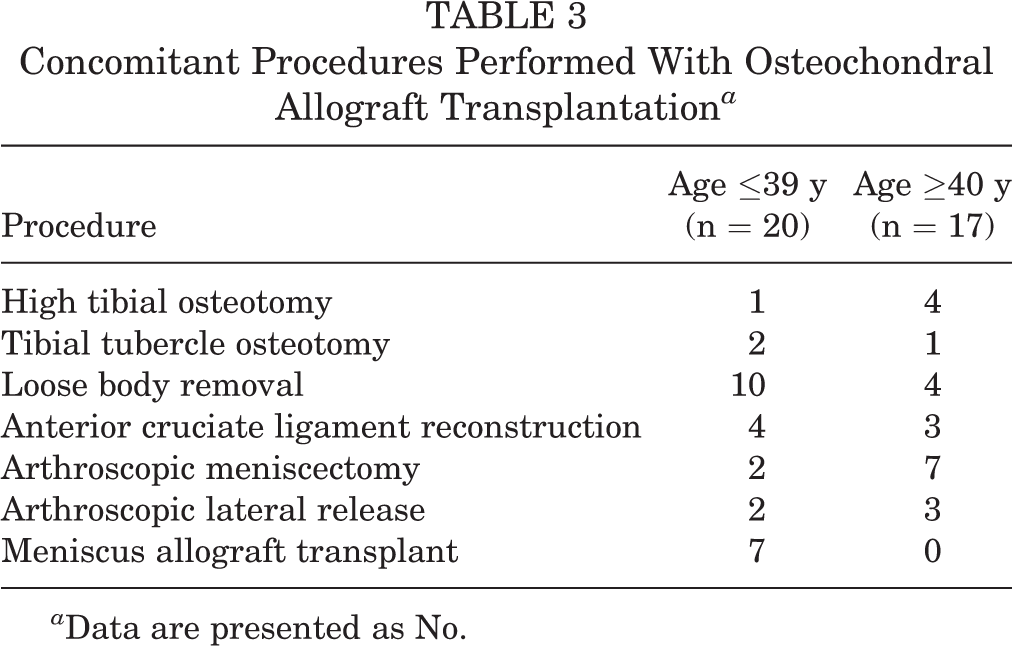
a Data are presented as No.
A significant difference in mean baseline PRO scores was not detected between the study group, the control group, or the group lost to follow-up, aside from the KOOS Activities of Daily Living subscore; younger patients had higher baseline function, which declined with increasing age in the other groups (Table 4). In both the study and the control groups, there was a statistically significant improvement from baseline to final follow-up (at least P < .03) for all 5 KOOS subscores and the IKDC score but not for VR-12 physical or mental scores. There was no statistically significant difference (P > .3) between the study and control groups in the magnitude of change from baseline for each outcome (Table 5). Maximum improvements were seen in the KOOS Quality of Life (QOL) and Sports & Recreation subscores in both the control and the study groups.
Baseline Patient-Reported Outcome Scores a

a Data are presented as mean ± SD. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; VR-12, Veterans RAND 12-Item Health Survey.
b Robust 1-way analysis of variance.
c Sample sizes vary slightly depending on the subscale: Symptoms (≤39: n = 39), Pain (≤39: n = 40), ADL (≤39: n = 40; lost to follow-up: n = 36), Sports & Recreation (≤39: n = 37; ≥40: n = 35; lost to follow-up: n = 36), and QOL (≤39: n = 40).
d Sample sizes vary slightly depending on the group: ≤39: n = 16; ≥40: n = 16; lost to follow-up: n = 29.
Preoperative, Postoperative, and Change in Outcome Scores at Final Follow-up a

a Data are presented as mean ± SD. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; VR-12, Veterans RAND 12-Item Health Survey.
b Postoperative scores indicate values at final follow-up for each patient for each measure; as such, mean values represent a longitudinal range of follow-up time, not a discrete point for all patients.
c Welch t test for difference in change from preoperative scores between groups.
When the given PRO data sets were modeled in a regression framework to evaluate long-term trajectories with adjustments for patient demographics and surgical variables, there were no statistically significant differences between the study and control groups at any projected time point (Table 6). The minimum detectable effect size at 80% power with alpha set to 0.05 was 0.49, indicating that time-averaged differences as small as one-half of the baseline SD across the longitudinal model would be detectable with the group sample sizes that we obtained. In this study, the differences were much smaller than one-half the baseline SD for all PRO scores, which is an average difference of about one-fourth of the baseline SD in magnitude. For all outcomes, the projected long-term growth curves indicated that the groups were similar, at least to the power that the sample size in this study offered. Although there was a remarkably consistent tendency for the younger group to have slightly higher “final” levels on most of the outcomes, even the largest differences were usually small and not significantly different. The projected long-term growth curves and differences between groups along the same time frame for the KOOS QOL are provided as an example in Figure 1, while the growth curves for the remainder of the outcomes are included as Figure A1 in the Appendix.
Differences Between Groups at Various Time Points Within Longitudinal Modeling a

a Data are presented as estimate ± SE. Positive values: younger age group greater than older age group; negative values: younger age group less than older age group. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; VR-12, Veterans RAND 12-Item Health Survey.
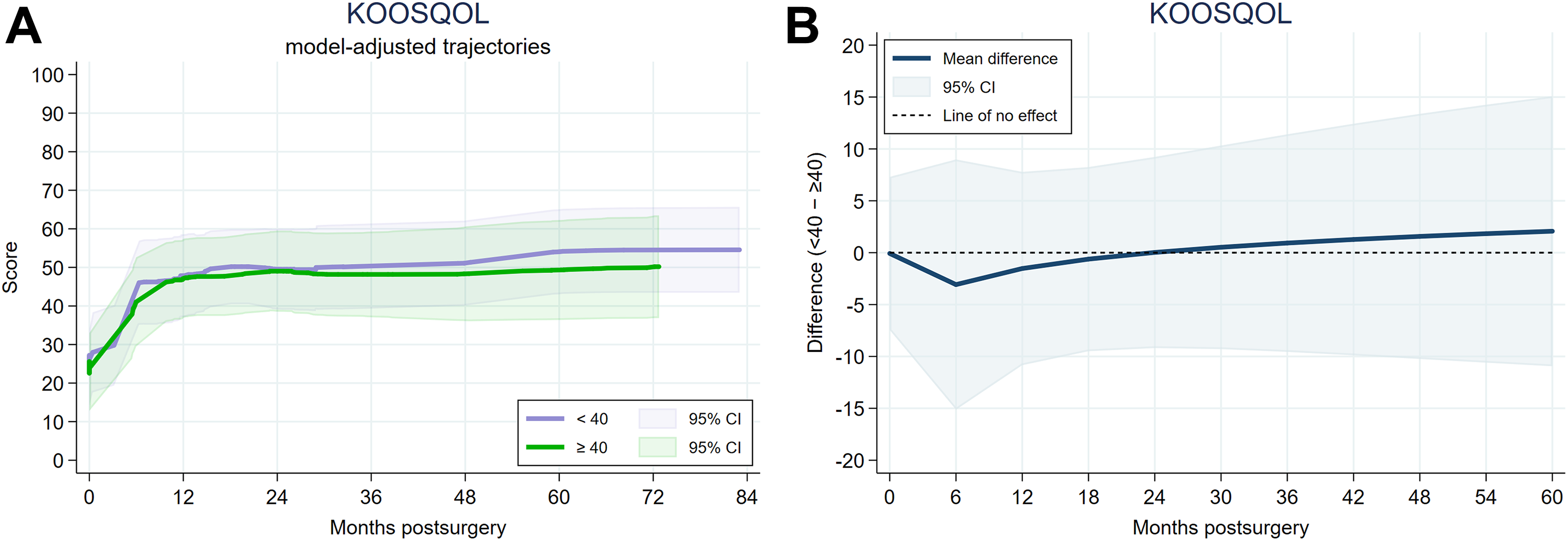
(A) Representative longitudinal model-based regression for the Knee injury and Osteoarthritis Outcome Score (KOOS) Quality of Life (QOL) (mean [95% CI]), accounting for potential confounding factors, including offset of age at surgery from the mean age for the group (ie, age offset from 27.19 years in the ≤39-year group and from 52.32 years in the ≥40-year group), body mass index at surgery, sex, size of the lesion, prior surgery, and number of grafts. (B) Representative difference between growth trajectories for the younger and older patient groups.
Failure was defined as a patient undergoing any procedure that removed or revised the allograft or underwent conversion to unicompartmental or total knee arthroplasty. The study group had 9 (24%) patients undergo a reoperation after the index surgery, with 1 surgery defined as a failure (Table 7). The patient who failed surgery underwent conversion to total knee arthroplasty 6 years after the index surgery. Comparatively, the control group had 2 failures among 14 (33%) patients who underwent a reoperation. The failures in the control group underwent revision to a medial unloading spring implant (an investigational device) 3 years after the index surgery in one case and revision to an allograft 1 year after the index surgery in the other case.
Reoperations After Osteochondral Allograft Transplantation a

a Data are presented as No. Some knees had >1 procedure performed during reoperation or >1 reoperations.
b Planned second-stage reoperation.
c Failure.
Discussion
The principal findings of this study demonstrate that both the study and the control groups experienced a statistically significant improvement in all 5 KOOS subscores and the IKDC score at final follow-up and that there was not a significant difference in the results for the groups because of age alone. Additionally, the older and younger groups were not statistically different with respect to overall pain and function, as measured by KOOS, IKDC, and VR-12 scores, at both baseline and final follow-up. The greatest improvement for both groups was seen in functional outcomes, specifically the KOOS QOL and Sports & Recreation. The relatively high SDs among PRO scores for a given group account for heterogeneity among the population at baseline. When modeled in a regression framework to account for any differences in patient demographics and surgical variables other than age, there were still no statistically significant differences in outcomes between groups within the defined follow-up period or over a projected long-term follow-up. Overall, these findings supported our hypothesis that patients aged ≥40 years and without osteoarthritis benefit as much from OCA transplantation as younger patients.
While studies investigating the efficacy of OCA transplantation in younger patient populations include pain as an outcome, the primary outcomes in these young and active populations are functional, primarily return to sport. 11,13 Unlike younger patients, however, those older than 40 years are less likely to be engaged in organized sports for which return to play is a primary outcome, so pain reduction often represents a primary goal of intervention. When evaluating a heterogeneous population for differences in patient factors including smoking, workers’ compensation, BMI, and preinjury activity level, Nuelle et al 14 found that patients who had a lower BMI and higher preoperative activity levels benefited more from OCA transplantation when only considering pain outcomes. Frank et al 9 similarly found BMI, as well as the number of prior surgeries, to be an independent risk factor for failure over long-term follow-up after OCA transplantation. As older patients tend to be less active, have a higher preoperative BMI, and have potentially had more time to undergo prior surgery, these confounding variables may lead to the conclusion that older patients do not benefit from OCA transplantation. When accounted for in our modeling, BMI, among other covariates, did not significantly influence the response of the given populations to intervention based on differences in age alone. Surprisingly, the older group had a lower rate of previous surgery than the younger group; however, this only accounted for cartilage procedures. This metric likely corresponds to the mechanism of injury and indications for chondral restoration, such that the younger group presented with OCD lesions, whereas the older group presented with traumatic lesions or focal degenerative lesions secondary to prior trauma. To this point, the clinical decision to offer an older patient cartilage restoration versus total joint replacement is predicated on the extent of the cartilage injury and degenerative osteoarthritis. This decision should be based on clinical history, a physical examination, and imaging; those with a focal lesion may be candidates for OCA transplantation, while those with more diffuse osteoarthritis will benefit from total joint replacement.
Pain outcomes were significantly improved from baseline in our study population; however, larger improvements in functional outcomes of activities of daily living, quality of life, and sports and recreation indicate that older patients benefit to a degree similar to younger patients, despite differences in activity demands. We argue that the use of more objective functional outcomes over subjective pain scores may better elucidate the overall success of cartilage restoration procedures in older populations, just as return to play represents a primary outcome for younger patients.
To date, the literature on outcomes after OCA treatment in middle-aged patients is limited. There have been 2 recently published cohort studies that have evaluated PRO data to determine if age is an independent risk factor in older patients after OCA treatment. 8,15 Our findings that older patients benefit from OCA transplantation to a degree similar to younger patients are in agreement with these studies and further validate OCA transplantation as a reasonable approach to focal cartilage restoration, regardless of patient age at the time of surgery. Frank et al 8 reported that in a cohort study of 55 patients older than 40 years and 115 patients younger than 40 years, the older patients who underwent OCA transplantation did not have inferior outcomes compared with the younger group. The authors concluded that OCA treatment is a safe and reliable treatment option for osteochondral defects, regardless of patient age. 8 Similarly, in a noncomparative study among 51 patients older than 40 years, Wang et al 15 reported that OCA treatment resulted in clinically significant improvements in knee symptoms, although there was a higher failure rate in this cohort than in patients younger than 40 years when compared with historical studies conducted in younger patient populations.
A primary limitation of this study is the duration of follow-up, which cannot necessarily capture failures beyond the immediate or short term. We used the available data to build robust models for the longitudinal trajectory of groups beyond 5-year follow-up, but these models do not predict or account for clinical failures. Another clear limitation of this retrospective cohort study that relied on the prospective collection of PRO scores is loss to follow-up. We characterized those lost to follow-up relative to the study and control groups, with the primary differences being age and indication for surgery. The patients lost to follow-up were of an intermediate age and had a greater proportion of cartilage lesions secondary to avascular necrosis or of failed prior microfracture, with fewer traumatic lesions. When presenting to a tertiary academic center, such patients often have experienced prolonged disability and multiple failed therapies. After surgical intervention, these patients may be satisfied and want to finally move on without constant follow-up in prospective research. Alternatively, they may be dissatisfied and seek care elsewhere. A third limitation is the lack of demographic factors, including smoking and workers’ compensation status, which may be age-dependent confounding variables. Frank et al 8 reported a significantly higher proportion of workers’ compensation claims but no difference in clinical outcomes in the older group relative to the younger group; however, they did not assess specifically for interactions between variables.
The present study is further limited by a lack of quantitative analysis of radiographs for lower extremity alignment and/or osteoarthritis. All patients included in the current study had preoperative imaging that demonstrated at least 1 focal cartilage lesion warranting OCA transplantation; however, radiographs for quantitative scoring were not obtained unless there was a clinical suspicion of malalignment based on the mechanism of injury and gait analysis or osteoarthritis based on history and a physical examination. Malalignment was addressed primarily in patients with patellofemoral injuries. Some isolated patellofemoral lesions benefit from concomitant procedures, including lateral release or tibial tuberosity osteotomy, to correct malalignment that initially contributed to chondral injuries or would otherwise impede graft healing. For osteoarthritis, we have previously reported that low Kellgren-Lawrence grades (representing minimal to no radiographic evidence of osteoarthritis) have a positive effect on PROs after minimally invasive chondroplasty procedures. 1 While we expect similar results across all cartilage procedures and know that there is a higher prevalence of osteoarthritis with increasing age, we did not quantify the Kellgren-Lawrence grade in this setting because osteoarthritis is a contraindication to OCA transplantation. 7 Thus, we avoided OCA transplantation in patients with clinical or radiographic evidence of osteoarthritis.
Conclusion
We report in this study that patients aged ≥40 years benefit from fresh OCA transplantation for the treatment of focal cartilage defects in the absence of osteoarthritis to a degree similar to younger patients, especially when considering functional outcomes. With that said, consideration must still be given to confounding demographic and surgical variables that may independently influence outcomes. With a longer follow-up and more experience in cartilage restoration for older patients with focal cartilage lesions and without osteoarthritis, we hope to eventually further define the role of biological restoration as a method for long-term joint preservation or a bridge to total joint replacement based on the clinical situation. When added to recent studies conducted by Frank et al 8 and Wang et al, 15 our longitudinal regression modeling results and clinical outcomes support the position that OCA transplantation is a reasonable treatment modality for older patients based on age alone.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.C.C. is a consultant for JRF Ortho, DePuy, Histogenics, Moximed, and Arthrosurface and has received research support from EMD Serono, Zimmer Biomet, Histogenics, and Moximed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Oregon Health & Science University (No. 4745).