
Abstract
Background:
Gadopentetate dimeglumine–enhanced magnetic resonance imaging (MRI), or gadolinium-enhanced MRI, was used to prospectively study the postoperative course of bone–patellar tendon–bone (BPTB) and combined semitendinosus and gracilis (STG) tendon autografts following arthroscopically assisted reconstruction of the anterior cruciate ligament (ACL) in humans. Gadopentetate dimeglumine is a contrast agent that has been shown to enhance the signal of vascularized tissue when examined by MRI.
Purpose:
To prospectively determine and compare the pattern and timing of autograft revascularization following arthroscopically assisted ACL reconstruction by BPTB or STG autografts.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 73 patients (63 males, 10 females) with ACL tears who were scheduled to undergo reconstruction consented to participate in this study. The patients were randomized to receive arthroscopically assisted reconstruction of the ACL employing either BPTB or STG autografts. Gadolinium-enhanced MRI scans were scheduled at 3-month intervals during the first postoperative year to assess the integrity, timing, and pattern of enhancement of the ACL graft. The temporal sequence and morphologic characteristics of imaged signals were compared for both types of ACL reconstructions.
Results:
Based on all knees with 1 exception, there were no statistically significant differences in gadopentetate dimeglumine–mediated graft enhancement grade observed between BPTB and STG autografts.
Conclusion:
The results suggest that autograft revascularization probably varies in intensity and location during the time course of graft healing. The interval signal changes observed 3 to 9 months, but especially 6 to 9 months, postoperatively are due to increased contrast uptake as a reflection of ongoing neovascularization during the process of ligamentization.
Arthroscopically assisted anterior cruciate ligament (ACL) reconstruction is a commonly performed orthopaedic procedure, with the most common autografts being bone–patellar tendon–bone (BPTB) and semitendinosus and gracilis (STG) tendons. 18 Each has had its proponents, with BPTB grafts called the gold standard by some. 11 However, a recent systematic review comparing long-term outcomes after reconstruction with either BPTB or STG autografts suggested there were no significant differences in manual or instrumented laxity and graft failures. 27
Since its inception, magnetic resonance imaging (MRI) has revolutionized the diagnosis and treatment of musculoskeletal disorders. 32 Use of MRI in the knee is an accepted technique for evaluating the status of the ACL after injury. 23,24,31,33 Specifically, this technology has been applied to assess the position and integrity of the ACL graft following reconstructive surgery. 3 Howell et al 12 found that MRI could delineate, by increased signal intensity, those STG autografts that were impinged by the intercondylar roof. Autz et al 5 examined the postoperative appearance of reconstructed knees in which BPTB autograft was used for ACL reconstruction, and they found that the grafted patellar tendon demonstrated a variable appearance on MRI, with the most common pattern being a thick, well-defined low signal intensity band on T1- and T2-weighted sagittal and coronal images. However, in approximately one-third of their examinations, including clinically stable and unstable knees, the graft had an attenuated appearance. In contrast, Rak et al 28 performed MRI examinations on patients who underwent arthroscopic ACL reconstruction with BPTB autografts and found a 92% correlation between clinical examination and MRI results. Those patients with clinical ACL laxity failed to demonstrate a well-defined autograft with MRI examination. In a study examining the MRI appearance of STG autografts used for ACL reconstruction, Howell and coauthors 13 found that although increases in signal intensity were regionalized to the distal two-thirds of the intra-articular portion of the graft, the clinical outcome could not be predicted per the MRI signal.
After placement, an ACL autograft undergoes healing in sequential phases: necrosis, revascularization, cellular repopulation, and remodeling. Arnoczky et al 4 found that canine patellar tendon ACL autografts remained avascular for 8 to 10 weeks after surgery, with vascularization occurring over the ensuing 10-week period. This vascularization response subsided by 26 weeks, and the graft had the histologic appearance of a normal ligament 1 year postoperatively. A similar response may occur in humans. 28 In a 2-year study of sheep, Weiler et al 34 found that high signal intensity on MRI reflected decreased mechanical properties of the graft during early remodeling but that gadolinium-enhanced signal intensities were stronger than those observed with plain MRI. The weight of available evidence shows that revascularization of an ACL autograft is an important determinant of graft survival and strength.
Enhanced MRI with the paramagnetic contrast agent gadopentetate dimeglumine, or gadolinium-enhanced MRI, has been frequently used in the evaluation of musculoskeletal disorders. This agent causes T1 shortening (spin–lattice relaxation time) and resultant higher signal intensity on T1-weighted images. After intravenous injection, the initial distribution of gadopentetate dimeglumine is relative to blood flow. 6 In the musculoskeletal system, this agent enters tissues with increased vascularity a few minutes after injection and is cleared less rapidly than from the surrounding normal tissue, providing a basis for detectable signal changes. 6
A preliminary study on gadolinium-enhanced MRI of BPTB autografts was presented by Gillogly et al (“Magnetic Resonance Imaging in the Assessment of Patellar Tendon Autograft Anterior Cruciate Ligament Reconstruction.” Scientific exhibit at the American Academy of Orthopaedic Surgeons 59th Annual Meeting, 1992). They studied 80 MRI examinations of knees that underwent ACL reconstructive surgery, and they found that maximum gadolinium enhancement of the signal intensity was present from 3 to 7 months postoperatively, suggesting that revascularization was occurring during this period. More recently, Ntoulia et al 26 studied revascularization in human BPTB autografts at 6 and 12 months postoperatively using contrast-enhanced MRI. In their study of 32 male patients, they found that revascularization took place gradually along the length of the graft but occurred faster in the intra-articular portion.
Even though the most commonly employed techniques of reconstructing the ACL use either BPTB or STG autografts, no study to date has prospectively compared the gadolinium-enhanced MRI revascularization response of STG autografts with that of BPTB autografts. The goal of this prospective study was to determine the pattern and timing of autograft revascularization following arthroscopically assisted ACL reconstruction by 2 commonly used surgical techniques. One technique employed an autogenous BPTB preparation as the ACL graft, and the other utilized autogenous STG tendons as an ACL autograft. Specific aims included characterization of autograft healing as represented by contrast-enhanced MRI signal changes, identification of any temporal or regional revascularization differences between the employed reconstructive techniques, and determination of any differences in overall graft healing.
Methods
Patient Selection
Patients at our institution who had reached skeletal maturity were considered possible candidates for ACL reconstructive surgery if they had pain and symptomatic instability that interfered with activities of daily living. Patients undergoing revision ACL reconstruction, those with multiple ligamentous injuries, those who were obese (body mass index >37), and those with a history of allergic reaction to previous administration of a contrast agent were excluded from the study population. Sixty-three male and 10 female patients with ACL tears were enrolled during the 4-year period of this study from 1993 to 1997 (Figure 1). Patient ages ranged from 15 to 51 years (mean, 27.3 years), with a mean body mass index of 26.1. The study protocol was reviewed and approved by our institutional review board. Each patient was given a detailed explanation of the anticipated benefits and risks of participating in the study, and a signed informed consent document substantiated consent. Patient confidentiality was maintained throughout the study. Patients were randomized via a random number–generated table to receive arthroscopically assisted ACL reconstruction with BPTB autograft 8,10,16 or quadrupled STG autograft. 19,30

Patient flow diagram. ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; MRA, magnetic resonance arthrogram; STG, semitendinosus and gracilis.
Operative Technique
Surgery was performed by 2 orthopaedic surgeons. The middle third of the patellar tendon was harvested through a 6- to 8-cm midline incision beginning just above the inferior pole of the patella extending inferiorly to the level of the tibial tubercle. A 10 mm–wide graft was obtained, and the attached 25 mm–long bone segments (10 mm in depth) were freed with an oscillating saw and a curved osteotome. Nonabsorbable sutures were then placed through the bone blocks for later graft positioning. The gracilis and the semitendinosus tendons were isolated through a 4-cm longitudinal incision over the insertion of the pes anserinus. The tendons were harvested proximally with an open tendon stripper that glides over the tendon and releases it at the musculotendinous junction. Both tendons were then doubled, and nonabsorbable sutures were placed into the free ends to facilitate graft pull-through.
All knees were examined arthroscopically, and any meniscal or other intra-articular lesions were treated as appropriate. ACL reconstruction was performed with an arthroscopically assisted technique. A notchplasty was performed if needed, and the ACL stump was debrided to minimize the possibility of future notch impingement from scar tissue. The tibial tunnel was placed to exit intra-articularly in the footprint of the ACL anatomic tibial insertion, and the posterior intra-articular margin of the tunnel was smoothed with a rasp to minimize edge carving. The femoral tunnel was created in the lateral femoral condyle at the posterior origin of the ACL (10 o’clock for the right knee and 2 o’clock for the left knee), with a low anteromedial portal or transtibial technique as appropriate to achieve desired placement, and its anterior intra-articular edge was smoothed to minimize graft chafing. Both patellar and hamstring autografts were tensioned near full knee extension and visualized arthroscopically with the knee at full extension to verify lack of notch impingement. The BPTB autografts were fixed in tibial and femoral tunnels with metal interference screws, and the STG tendons were fixed to the lateral femur and proximal tibia with a 6.5-mm screw and washer.
MRI Evaluation
Patients had coronal, axial, and sagittal MRI studies of the autografts at 3, 6, 9, and 12 months postoperatively. MRI scans were performed with the patient supine with a Signa 1.5-T magnet (General Electric Medical Systems) with a dedicated quadrature detection knee coil. Sagittal images were 3 mm thick to reduce confusing partial-volume effects, 22 and an oblique sagittal imaging plane was used to permit the entire graft to be visualized from origin to insertion in 1 section. 7,12,21,31 The axial and coronal images were 5 mm thick. Imaging was performed with the knee in 15° of external rotation to optimally align the graft in the sagittal plane. 21,28 Imaging sequences included the following: T1-weighted 5-mm axial localizer slices, T2-weighted fast spin echo oblique sagittal 3-mm slices through the ACL, T1-weighted coronal 5-mm slices through the entire knee, and T1-weighted oblique sagittal 3-mm slices obtained through the ACL graft before and after intravenous injection of 10 mL of gadopentetate dimeglumine (Magnevist; Berlex Laboratories).
MRI scans were graded by experienced board-certified radiologists blinded to the type of ACL reconstructive procedure employed. Mean pre– and post–gadopentetate dimeglumine injection pixel values for oblique sagittal images were determined for each of 3 geographic imaged zones of the graft (Figure 2). The tibial zone was defined as the segment of graft within the tibial tunnel; similarly, the femoral zone was that portion of the graft within the lateral femoral condyle. The remaining middle portion of the graft was considered the intra-articular zone. The homogeneity, continuity, and signal intensity of the ACL graft in each zone were determined with a modification of the grading scale of Jansson et al 15 whereby 4 instead of 3 grades of enhancement were used to describe signal characteristics (Figure 2): grade 0, no enhancement; grade I, minimal enhancement; grade II, moderate enhancement; and grade III, maximal enhancement. Specifically, the signal intensity was graded from 0 when similar to that of the intact posterior cruciate ligament, to III when similar to subcutaneous fat.

Examples of gadolinium enhancement (arrows) in the 3 zones of study: (A) no zone enhancement, (B) grade I tibial zone enhancement, (C) grade II femoral zone enhancement, and (D) grade III intra-articular zone enhancement.
Statistical Analysis
A power analysis with an alpha of .05 and a power of 0.80 and with SDs drawn from Jansson et al, 15 who used signal strength categorization as their measure, indicated that a difference of 0.2 units could be detected by a sample size of 11 per type of autograft and a difference of 0.1, by a sample size of 41. Gadolinium-enhanced MRI grades for the ACL grafts were statistically summarized for BPTB and STG autografts for the 3 zones under study (tibial, intra-articular, and femoral) and for the 4 postoperative time points (3, 6, 9, and 12 months). At each time point and location, the mean enhancement grade was calculated for the graft types. Although enhancement grades are values that behave as ranks, means were used because they better show typical grade behavior than do medians. However, the rank-sum test was used to compare enhancement grades for the graft types. Statistical significance was set at P < .05, and analyses were performed with Stata software (v 14; StataCorp).
Results
Clinical Evaluation
At the end of the 12-month imaging period, all study patients had resumed their normal activities of daily living, with no cases of functional instability except for 1 patient who sustained a traumatic ACL graft tear. Apart from this patient, serial physical examinations by orthopaedic surgeons during the study period indicated no BPTB of STG graft tears, as clinically demonstrated by negative Lachman and pivot-shift tests.
Gadolinium MRI Evaluation
Table 1 shows the mean enhancement grade differences between BPTB and STG autografts for the tibial, intra-articular, and femoral zones at 3, 6, 9, and 12 months postoperatively, as well as the sample sizes at each period and the P values of the rank-sum tests comparing autograft types. At postoperative 3 months, we collected data from 72 subjects (n = 31, BPTB; n = 41, STG), but we experienced a decline in the number of patients undergoing MRI scans at 6, 9, and 12 months (n = 31, 14, and 5, respectively). While several of our differences in signal category were sizable, although not reaching significance, we noted that they vacillated between BPTB and STG being the larger, thereby lending credence to a conclusion of no real difference.
Differences in Mean Enhancement Grades for Graft Type a
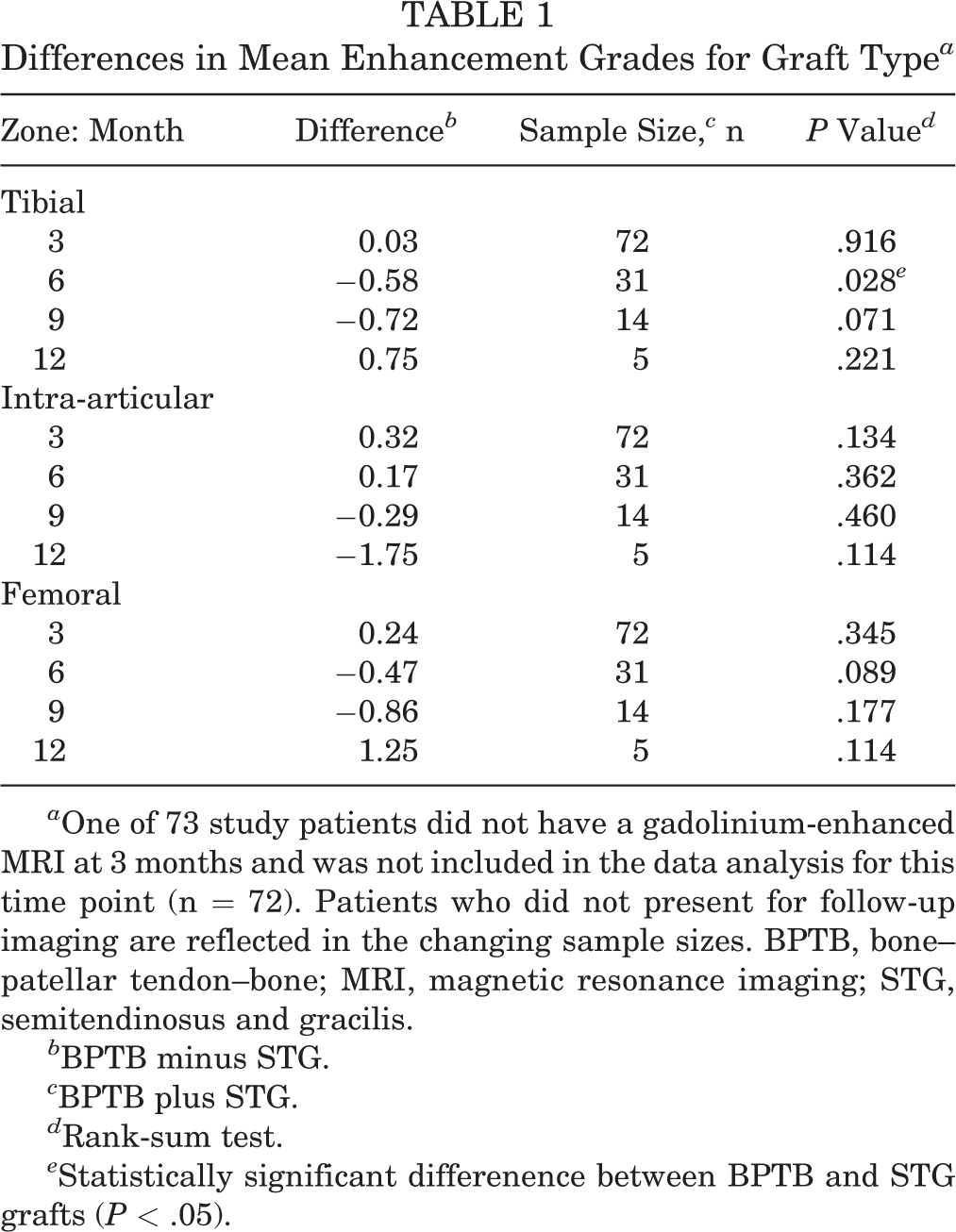
a One of 73 study patients did not have a gadolinium-enhanced MRI at 3 months and was not included in the data analysis for this time point (n = 72). Patients who did not present for follow-up imaging are reflected in the changing sample sizes. BPTB, bone–patellar tendon–bone; MRI, magnetic resonance imaging; STG, semitendinosus and gracilis.
b BPTB minus STG.
c BPTB plus STG.
d Rank-sum test.
e Statistically significant differenence between BPTB and STG grafts (P < .05).
Postoperative 6-month data showed that within the tibial zone, there was greater mean enhancement grade of STG grafts as compared with BPTB grafts (0.58; P = .028). However, when a Bonferroni adjustment was made for multiple comparisons of data from the same patients, there were no statistical differences between grafts. Therefore, the overarching enhancement pattern for all zones and time points indicated no marked observable difference in autograft revascularization (Figure 3).

Mean enhancement grades for bone–patellar tendon–bone (BPTB) and semitendinosus and gracilis (STG) graft types at 3, 6, and 9 months postoperatively for the tibial, intra-articular, and femoral zones. The asterisk (*) shows a significant difference (P = .028) between graft types per the rank-sum test. Twelve-month grades are not shown, because the BPTB group had only 1 patient.
Discussion
For ACL reconstruction to be successful, the autograft must proceed through a process of “ligamentization,” a term coined by Amiel et al. 2 In their study with rabbits that underwent patellar tendon ACL reconstructions, the investigators found that histologic and biochemical data demonstrated a “remarkable metamorphosis” such that tissue originally consisting of patellar tendon had been transformed to a substance very similar to normal ACL. An analogous process is thought to occur in humans.
To our knowledge, this is the first prospective randomized study to evaluate ACL graft revascularization with contrast-enhanced MRI to compare BPTB and STG autografts. Gadolinium-enhanced MRI examination of ACL autografts provides information on graft revascularization not available with standard MRI techniques. The results suggest that patellar and hamstring tendon autografts demonstrate varying increased uptake of gadopentetate dimeglumine during the postoperative course, with zonal and temporal differences corresponding to geographic region and graft type.
There are several possible reasons for the differential contrast uptake and, thus, the varying MRI signal enhancement within the graft. Increased vascularity attributed to an initial inflammatory response in the early postoperative period may occur at different rates within different regions of the graft. Subsequent neovascularization of the nonvascularized autogenous graft probably also occurs in a differential geographic pattern, possibly as a reflection of the available blood supply in the specific recipient region. Evidence of nonuniform graft revascularization was reported by Nikolaou and colleagues. 25 Using microangiography, these investigators showed that revascularization of a canine ligament autograft occurred by 8 weeks; however, a small, relatively hypovascular zone was still present in the middle of the graft at that time. By week 24 onward, the microangiographic appearance of the graft was normal. Vessel ingrowth was observed to come mainly from the infrapatellar fat pad and the synovium and from endosteal blood vessels within the bone tunnels. Later in the healing process, the number of vessels in the healing canine autograft decreased from a supraphysiologic to a physiologic level.
A number of factors may affect graft neovascularization. A clinical study by Kim et al 17 showed that cigarette smoking appeared to have a negative effect on subjective and objective outcomes of ACL reconstruction. Although the exact pathophysiologic process by which cigarettes exert a negative influence is unknown, the authors proposed that smoking may impede graft revascularization. In addition, mechanical stress has a role in modulating graft healing such that anatomic tunnel placement facilitates physiologic loading of the ACL graft. 20 It has also been suggested that excessively low or excessively high graft tension may reduce the biomechanical properties of the graft, although the optimal tension is unknown. 9 Furthermore, Rodeo et al 29 found that graft-tunnel motion in animals may adversely affect early graft healing, leading to osteoclast-mediated bone resorption. They proposed that early, aggressive postoperative rehabilitation may have detrimental effects on graft-to-bone healing.
Alm et al 1 performed biopsies of human midthird BPTB autografts in 16 patients who underwent repeat arthroscopy or arthrotomy ranging from 3 months to 5.5 years after ACL reconstruction. Transplants that were taut were all histologically well organized and in some cases similar to normal ligamentous tissue; however, transplants that were lax were less well organized. In a more recent study, Falconiero et al 10 performed repeat arthroscopy and graft biopsies in 48 patients (43 ACL autografts, with 5 normal ACLs to serve as controls) and observed that neovascularization and increased cellularity continued to increase up to 12 months postoperatively. They also noted that collagen organization seemed to plateau 12 months after surgery.
The weight of both animal studies and the limited human histologic studies to date show that an autograft will undergo, to at least some degree, a multiphase process that includes an initial inflammatory response, a revascularization phase, a cellular repopulation phase, and a subsequent and prolonged remodeling phase. The changes in vascularity associated with these different phases provide an indication of autograft healing. Increased vascularity within the early period is probably an indication of the early healing response. However, evidence of increased vascularity that is present ≥12 months after surgery probably indicates that the graft is less than robust, as with graft notch impingement. 14
A limitation of our study is that contrast-enhanced MRI images do not describe the mechanism of autograft remodeling. Second-look arthroscopy with histologic graft analysis to correlate with the MRI signal intensity would have been ideal. However, this would have been difficult to justify given ethical considerations. Another limitation, analogous to other human studies, is that not every patient who began the study completed all contrast-enhanced MRI scans. Given that our study involved a mobile, mostly military population and was invasive, as it involved intravenous injection of contrast agent, we found that patient participation declined substantially over the yearlong period needed for the 4 scans. Our study was powered enough to draw conclusions at the 3-month mark but was underpowered at the 6-, 9-, and 12-month points to rule out type II error.
Conclusion
The results of this study suggest that autograft revascularization probably varies in intensity and location during the time course of graft healing. The interval signal changes observed at 3 to 9 months, and especially 6 to 9 months, postoperatively owing to increased contrast uptake probably reflect ongoing neovascularization as a component of the histomorphologic changes occurring during so-called ligamentization. Although BPTB autografts have sometimes been referred to as the gold standard, 10 our study suggested that with respect to revascularization, as reflected by gadolinium signal intensity, there were likely no marked differences between graft types during early healing. Gadolinium-enhanced MRI is a useful nonsurgical technique to study the time-course and pattern of ACL autograft revascularization and may be applicable to evaluation of other soft tissue healing. Characterization of postoperative graft healing has important implications in the development of optimum protocols for rehabilitation and for determining the appropriate time for return to unrestricted activities.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This investigation was supported by Naval Medical Research and Development Command (grant B2EW.00095.008.9311). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Department of the Navy, Naval Medical Research and Development Command.