
Abstract
Background:
Patient preference information has become increasingly more important in clinical decision making.
Purpose:
To assess patient preferences when making treatment decisions in the shoulder to determine which features are more important according to patient age, race, activity level, and sex.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Study participants aged ≥18 years were surveyed as to their preferences regarding surgical treatment for shoulder and proximal biceps abnormalities. Survey features included time to return to unrestricted activities, time to return to work, size and appearance of scars, the potential for persistent pain in the upper arm or shoulder, fatigue in the biceps with repetitive lifting, potential for muscle cramping, and deformity in the proximal biceps. Participants also completed a validated shoulder activity scale, and demographic data regarding age, race, and sex were collected.
Results:
A total of 349 participants (166 female, 183 male) with a mean age of 45 years (range, 18-81 years) completed the survey. Overall, time to return to unrestricted activities and residual pain were considered very important to the majority of the respondents, while the size and appearance of surgical scars were of little importance. Prior shoulder pain (ρ = –0.17; P = .01) and prior shoulder surgery (ρ = –0.16; P = .03) correlated to concern about time to return to unrestricted activities. Younger age (ρ = –0.11; P = .04) and a higher level of education (ρ = 0.14; P = .03) correlated with greater concern for time to return to work. Women and African Americans were more concerned about the size and appearance of surgical scars (ρ = –0.28; P < .0001 and ρ = –0.20; P = .0002, respectively) and biceps deformity. Respondents with a higher activity level (ρ = 0.20; P = .0002) and men (ρ = 0.11; P = .04) were more concerned about fatigue.
Conclusion:
Concerns about residual pain, time to return to unrestricted activities, and time away from work are important to patients when considering the treatment for shoulder lesions. Patient preferences are associated with age, sex, race, and shoulder activity level. These features should be considered when discussing treatment options for shoulder and proximal biceps tendon disorders.
Patient preference information (PPI) has become increasingly more important in clinical decision making. 6 Patient perspectives of a disease and their perception regarding the treatment for a disease may influence their decisions regarding treatment. PPI becomes even more relevant when multiple treatment options are appropriate and there is no definitive evidence that one treatment is clearly superior. 6 Decision making regarding the treatment for shoulder abnormalities, including degenerative rotator cuff tears, shoulder instability, and proximal biceps disorders, presents patients and surgeons with dilemmas in which PPI may be useful in deciding the best treatment approach.
There is growing evidence that surgical and nonsurgical treatment can be effective for degenerative rotator cuff tears, proximal biceps disorders, and shoulder instability. 11,15 Patients’ expectations regarding recovery time, lost work, residual pain, and loss of function may influence treatment decisions rather than the shoulder lesion itself. Similarly, there is no consensus on the best surgical treatment for proximal biceps disorders. Biceps tenotomy and tenodesis have similar clinical outcomes, but each has drawbacks that may be important to patients. 1,5,7,8,14,17,18 Because there is a higher incidence of cosmetic deformity and fatigue in patients treated with biceps tenotomy 12,16 and a higher likelihood of pain associated with tenodesis, 12 exploring patient preferences for these factors is critical to decision making. When faced with a treatment decision, it is important to understand what features of surgery and recovery may be important to patients so as to frame the discussion regarding their treatment.
Decisions regarding the treatment for shoulder injuries largely depend on the level of pain, functional disability, associated shoulder lesions, activity level, and response to conservative treatment. Additional relevant factors to discuss with patients include time to return to unrestricted activities, time to return to work, size and appearance of scars, the potential for persistent pain, fatigue in the biceps, the potential for biceps muscle cramping, or deformity in the biceps muscle. 2,3,9 Ideally, these factors are discussed as part of the informed consent process before surgery. In reality, these factors may be overlooked as the patient and physician focus on the underlying shoulder abnormality. Furthermore, decision making can be influenced by how the surgeon presents the choices to the patient. While the surgeon should guide the patient toward an informed decision, the concept that the surgeon can talk the patient into whatever treatment approach the surgeon prefers undermines the autonomy of the patient in making treatment decisions for himself or herself, particularly if there is more than one reasonable treatment option.
While each patient should make individual decisions based on his or her own preferences, identifying factors that are important to patients faced with selecting individualized treatment options can help guide patient-focused decision making while minimizing surgeon bias. As such, PPI has the potential to improve patient satisfaction with treatment decisions. The purpose of this study was to define patient preferences regarding features associated with shoulder and proximal biceps surgery and to determine if patient age, race, sex, or activity level predicts the relative importance of these features. Our hypothesis was that age, race, sex, and activity level have no association with how patients rate the importance of various features after surgery for shoulder and proximal biceps abnormalities.
Methods
A 23-item survey was developed by 4 fellowship-trained sports medicine surgeons to evaluate 7 specific features of surgical treatment for shoulder and proximal biceps abnormalities to determine what patients care most about when considering treatment for shoulder pain. The survey was written at a sixth-grade level for ease of understanding across the entire survey population. The features included (1) time to return to unrestricted activities, (2) time to return to work, (3) size and appearance of surgical scars, (4) the potential for persistent pain in the upper arm or shoulder, (5) biceps fatigue with lifting, (6) the potential for muscle cramping, and (7) deformity of the proximal biceps.
A combination of a Likert scale and ordinal ranking questions was used to determine the relative importance of these 7 specific features of shoulder and proximal biceps surgery as well as what features are most and least important when considering this type of surgery. The 7 topics were scored on a 5-point Likert scale as follows: 5, very much; 4, quite a bit; 3, moderately; 2, a little bit; or 1, not at all. The patients were then asked to choose which feature was the most and the least important to them. Finally, the patients were asked to rank these same 7 features from most to least important when considering surgery on their shoulder. We asked the questions in different ways to allow for an assessment of construct validity. The survey also collected basic patient demographics, including age, sex, race, education level, body mass index, occupation, and shoulder activity score. 2
After institutional review board approval, a convenience sample of adults aged ≥18 years presenting to an academic orthopaedic sports medicine clinic in the Midwest were asked to complete the survey. Participants were recruited to complete the survey regardless of their presenting complaint to the clinic. Anyone under the age of 18 years was excluded from the study.
Statistical Analysis
Based on a population estimate of approximately 525,000 people undergoing shoulder surgery per year in the United States, 13 we estimated that 269 surveys were needed to have 90% confidence that the survey sample population reflected the overall population undergoing shoulder surgery. 4 Spearman correlation coefficients (ρ) were used to assess the association between respondent characteristics and the Likert ratings of the importance of each feature. For correlations, female participants were coded as 0 and male participants coded as 1, and African American race was coded as 0 and non–African American race coded as 1. Percentage agreement was used to represent consistency in the identification of the most and least important features assessed using rankings as compared with listing the most and least important features. Kappa was not calculated because of limited variability in responses for some features. P values <.05 were considered statistically significant.
Results
A total of 349 surveys, including 166 female and 183 male respondents, were collected over a 12-month period. The mean participant age was 45 years (range, 18-81 years); 60% had a college (32%) or professional degree (28%). Forty-eight percent of the respondents had seen a physician for shoulder pain in the past. Only 23% had a history of shoulder surgery.
The time to return to unrestricted activities and residual pain were very important to the majority of respondents, whereas the size and appearance of surgical scars were of little importance (Table 1).
Importance of Features to Respondents on a Likert Scale a

a Respondent was asked to rate how much each feature would matter if he/she had to undergo shoulder and biceps surgery (5 = very much, 4 = quite a bit, 3 = moderately, 2 = a little bit, 1 = not at all).
When asked to rank those factors most important regarding shoulder and proximal biceps surgery, the time to return to unrestricted activities, residual pain, and time to return to work were consistently most important to the respondents (Table 2). The size and appearance of surgical scars were least important.
Ranking of Importance of Features to Respondents a
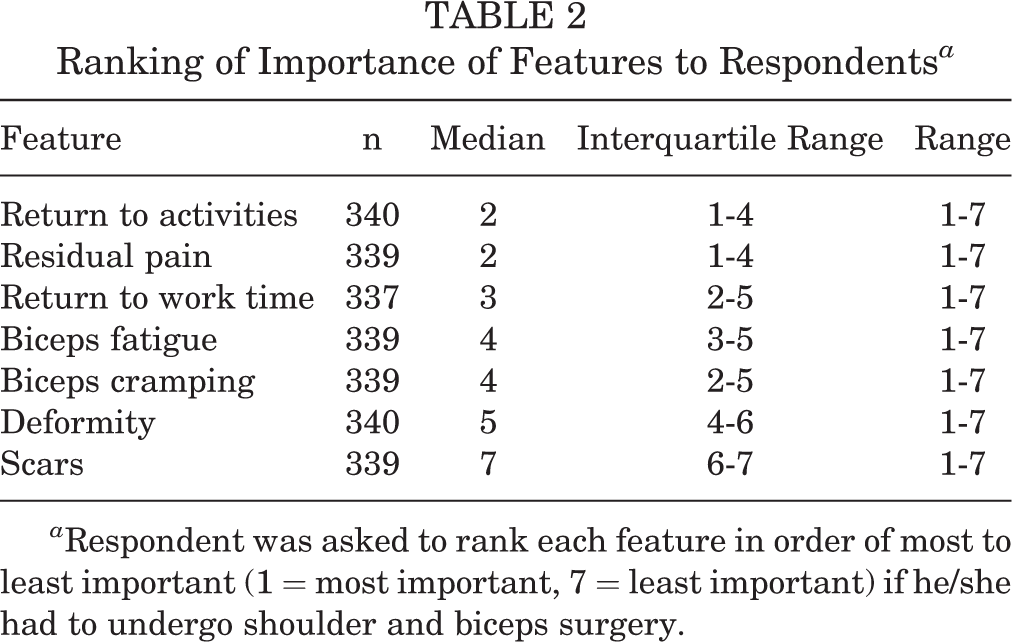
a Respondent was asked to rank each feature in order of most to least important (1 = most important, 7 = least important) if he/she had to undergo shoulder and biceps surgery.
The respondents were asked to indicate the single most concerning and the single least concerning features after shoulder and proximal biceps surgery. The most important features were time to return to unrestricted activities and discomfort in the upper arm after full recovery. The least important feature was the size and appearance of scars (Table 3).
Most and Least Concerning Features to Respondents a
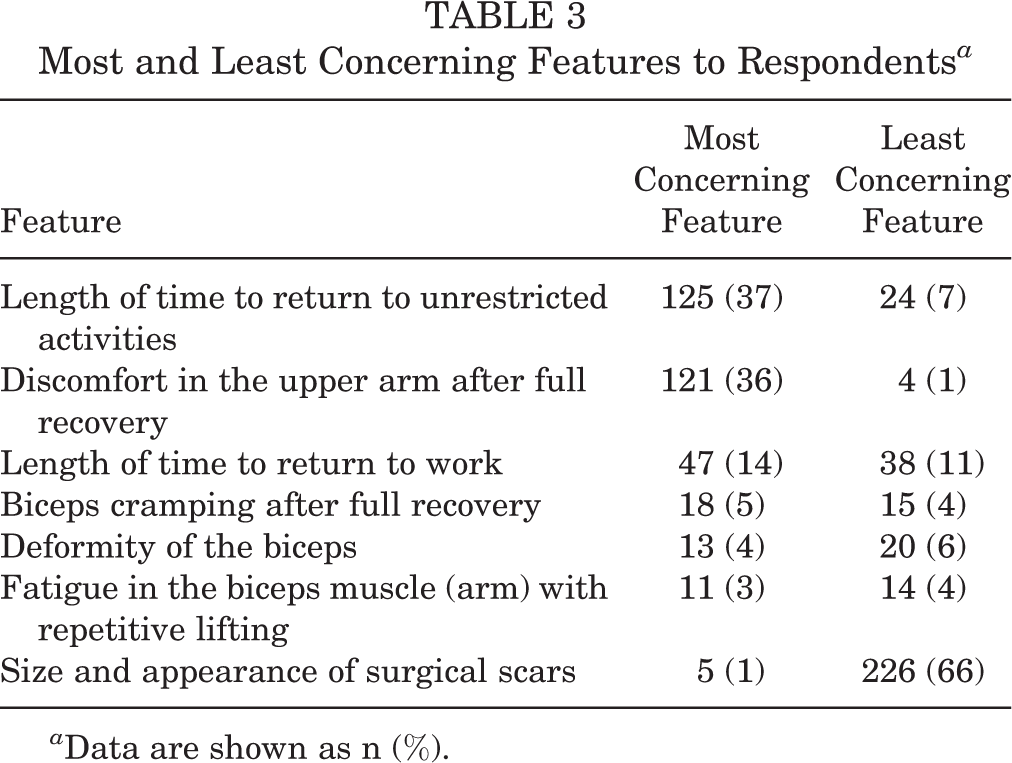
a Data are shown as n (%).
Age (ρ = –0.02; P = .72), sex (ρ = –0.03; P = .55), race (ρ = 0.02; P = .69), and activity level (ρ = 0.08; P = .16) were not associated with the Likert rating of the importance of time to return to unrestricted activities. Having previously seen a physician for shoulder pain (ρ = –0.17; P = .01) and having undergone prior shoulder surgery (ρ = –0.16; P = .03) correlated with concern about time to return to unrestricted activities. Younger age (ρ = –0.11; P = .04) and a higher level of education (ρ = 0.14; P = .03) correlated with greater concern for time to return to work. Activity level (ρ = 0.10; P = .06) did not correlate with concern for time to return to work. Women were more concerned about the size and appearance of surgical scars (ρ = –0.28; P < .0001) and biceps deformity (ρ = –0.14; P = .01) than men. African American respondents were more concerned than non–African Americans about the size and appearance of surgical scars (ρ = –0.20; P = .0002) and biceps deformity (ρ = –0.18; P = .001). Respondents with a higher activity level (ρ = 0.20; P = .0002) and men (ρ = 0.11; P = .04) were more concerned about the potential for biceps fatigue. Men were also more concerned about residual pain (ie, discomfort in the upper arm or shoulder) after surgery compared with women (ρ = –0.12; P = .03). Age (ρ = 0.04; P = .43), race (ρ = –0.05; P = .35), and activity level (ρ = 0.005; P = .93) did not correlate with concern for residual pain. Age (ρ = 0.08; P = .17), sex (ρ = –0.10; P = .08), race (ρ = 0.0001; P = .99), and activity level (ρ = –0.03; P = .61) did not correlate with concern for cramping discomfort in the biceps muscle.
There was a high level of agreement between those questions asking the respondents to rank each feature and those questions asking to list the most (percentage agreement ranged between 90% and 97% across all features) and least important features (percentage agreement ranged between 82% and 97% across all features). This indicates that the respondents were consistent in their ratings of what is important regardless of the way the questions were asked, thus supporting the construct validity of the survey.
Discussion
Independent of age, race, sex, and activity level, participants in our study were most concerned about the length of time needed to return to unrestricted activities and residual pain when considering shoulder and proximal biceps treatment. This may seem intuitive but cannot be assumed without clear evidence confirming these concerns. The respondents of this survey also indicated that the length of time to return to work was a significant concern, particularly in younger, more active people. Those with prior shoulder pain or shoulder surgery were significantly concerned about the time needed to return to unrestricted activities. There was moderate concern among the respondents regarding biceps deformity and cramping. Overall, women and African Americans were more concerned about cosmetic features such as scarring and deformity. Scarring was of least concern among the entire group of respondents. These data provide useful information as to what matters to patients when faced with decisions regarding treatment for the shoulder. It is important to discuss these features with patients when making decisions regarding the potential surgical treatment for proximal biceps disorders. Not addressing the primary areas of concern could decrease compliance with postsurgical restrictions and/or reduce a patient’s satisfaction with his or her treatment.
Galdi et al 9 recently reported patient preferences specific to biceps tenotomy or tenodesis. In their study, patients with biceps tendinitis discussed the diagnosis and treatment with a provider. Afterward, they were given a description of the 2 procedures and a list of features that were associated with each procedure. The authors found that 64% of patients chose biceps tenodesis when asked for a preference. Female patients were more likely to choose biceps tenodesis because of concerns about cosmetic deformity and residual pain. Male patients were more likely to choose biceps tenotomy because of concerns about recovery time. Overall, age, body mass index, occupation, and income level did not affect their preference for biceps treatment. Our findings are similar in that female participants were more concerned about deformity and scarring than male participants. We also found that age and activity level influenced the respondents’ concern for the length of time to return to work and that men were more concerned with residual pain compared with women.
Our study differs from the Galdi et al 9 study in that our survey evaluated general features of shoulder treatment in addition to biceps lesions. Also, respondents were not given any information about shoulder or biceps treatment from a medical provider before completing the surveys; thus, there was no concern for surgeon bias that may influence their responses. As many patients are faced with making treatment decisions in the office without prior knowledge of information related to their shoulder, we wanted to make sure that we had a mix of study participants who could evaluate what both “informed” and “uninformed” patients may identify as important. Nearly 50% of the study population had a history of shoulder pain, and 23% had undergone shoulder surgery in the past. Because we included a similar number of participants with and without shoulder pain or previous injuries, our data may be more generalizable to the overall population. Furthermore, our study and the Galdi et al 9 study show similar findings using different methodologies from different regions of the United States. The patient preferences are consistent and reproducible across studies, despite the variation in study design.
Previous work has shown that the shoulder activity scale is correlated with patient age and sex in addition to socioeconomic factors of income and type of employment. 2,10 Heavy laborers and those with higher income levels were shown to have higher shoulder activity scores, likely attributable to the demands of the job and their ability to participate in recreational activities that include contact and overhead sports, respectively. 2 This plausibly explains, at least in part, the findings that patients with a higher activity level were more concerned with time to return to work and the potential for biceps fatigue.
There are limitations to our study. While we believe that this study is generalizable to many patients in the United States, regional variation regarding preferences may exist. Our study may not predict patient preferences in countries outside of the United States. Additionally, while our survey data address general features that patients are frequently faced with when choosing a treatment for shoulder conditions, our data may not apply to all shoulder conditions or all shoulder surgeries. We also surveyed a convenience sample from an orthopaedic clinic consisting of patients who may or may not have experienced a shoulder injury. If a patient does not have the disorder in question, it may alter how he or she might view any potential treatments. However, the similar findings between our study and the Galdi et al 9 study suggest that this might not be as much of a concern. We did not analyze the association of occupation with preferences because of variable self-reported descriptions of occupation and unclear delineation of the specific duties required of each occupation. Instead, we chose to evaluate activity level with a validated shoulder activity scale that has been shown to correlate with occupational demands on the shoulder. 2,10
Another limitation is that we did not track the number of people who were offered the survey but refused to take it, which may introduce responder bias. Furthermore, the survey that we used has not been previously validated. Validation of a survey is a process rather than a specific test. We asked the survey questions in different ways to look for agreement in how the respondents answered each question, and we had a high level of agreement with the features that were most and least important regardless of how the questions were asked, which lends support to the survey’s construct validity.
Last, this survey’s data provide general information to medical providers that highlight the factors that may be important for different patient demographics. These data should not be used to make treatment decisions for patients. Treatment decisions should be individualized to each patient. Instead, these data should be used to help physicians understand what features may be important to patients across demographics to improve communication with patients and to ensure that their concerns are addressed before finalizing a treatment plan. Our study data are meant to provide insight into the concerns that patients may have, which need to be discussed when making treatment decisions.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for the statistical analysis by K.S.-M. was provided by the Washington University Institute of Clinical and Translational Sciences (grant UL1TR000448) from the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). M.V.S. is a paid speaker/presenter for Arthrex and Elite Orthopedics and is a consultant for Flexion Therapeutics and ISTO Technologies. M.J.M. has received educational support from Breg and Arthrex, is a paid speaker/presenter for Apollo Surgical, and is a consultant for Pacira Pharmaceuticals. R.W.W. has grants/grants pending from the NIH and receives publishing royalties from Wolters Kluwer–Lippincott Williams & Wilkins. R.H.B. is a consultant for Sanofi, Arthrex, and ISTO Technologies; is a paid speaker/presenter for Arthrex and Smith & Nephew; and has grants/grants pending from Zimmer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Human Research Protection Office of Washington University in St Louis.