
Abstract

Osteonecrosis is caused by diminished microperfusion of bone resulting in subsequent joint collapse. Estimates suggest that roughly 20,000 to 30,000 new cases are diagnosed annually in the United States, with even higher rates in other countries. 32 Osteonecrosis most commonly presents secondary to fractures or from nontraumatic means, such as prolonged glucocorticoid use, alcohol consumption, pancreatitis, or lipid disorders. 6,10,28,31,34 These latter conditions are believed to lead to the accumulation of fat emboli in the microcirculation or in the bone marrow, which can compromise blood flow and ultimately cause cellular death. 19,35
The disorder most often affects the hip and can also be seen in the knee joint at an incidence that is an order of magnitude less than the incidence in the femoral head. 27,32 Osteonecrosis can affect other joints as well, such as the shoulder, ankle, mandible, and spine. 7,14,15,23,30 Nonoperative management involves rest, limited weightbearing, and pharmacologic therapy, such as the use of bisphosphonates. 20 Surgical options in young patients consist of joint-preserving techniques including microfracture, autologous chondrocyte implantation, and autograft or allograft transplant; total joint arthroplasty (TJA) remains a last option. 1,22
Given that TJA is generally contraindicated in young patients, further investigation has been aimed at measuring the clinical outcomes associated with using allografts to repair large defects that may have otherwise been managed with TJA in older patients. While some success has been demonstrated in the literature, 13 investigators have not assessed graft incorporation using sequential postoperative magnetic resonance imaging (MRI). Furthermore, transplant of the entire medial femoral condyle for a large defect is very rare, and a paucity of clinical outcome data are available in the literature.
Here we describe a 25-year-old woman with a history of alcohol abuse and a course of glucocorticoids, in whom 2 previous surgeries failed. She underwent fresh hemicondyle allograft transplant of the right knee to treat osteonecrosis of the medial femoral condyle. To our knowledge, this is the first report to describe a case of medial femoral condyle osteonecrosis managed with large hemicondyle allograft transplant that also includes repeat MRI follow-ups at both 6 months and 1 year from surgery to evaluate for graft incorporation.
Case Presentation
Preoperative Evaluation
A 25-year-old woman was referred to our outpatient clinic to obtain a second opinion regarding her right knee. The patient had developed an insidious onset of knee pain approximately 2 years prior with a diagnosis of osteonecrosis following a 1-week course of high-dose prednisone treatment for an upper respiratory infection. Her medical history was also significant for heavy alcohol consumption of approximately 6 beers per day. As an initial course of management, microfracture surgery was performed at an outside hospital. The patient had persistent pain and underwent a second surgery that consisted of retrograde drilling at the same hospital 1 year before her surgery at our clinic.
At initial presentation in our clinic, the patient reported difficulty completing several activities of daily living, specifically walking up and down stairs, in addition to subjective knee weakness and an associated clicking or catching sensation. Using a 10-point visual analog scale (VAS) for pain, she indicated pain at rest (5/10) and pain with activities (8/10) and was able to ambulate only 50 feet before stopping due to pain. Her knee had moderate effusion, range of motion (ROM) 0° to 140°, and stable to varus-valgus stress of 0° and 30°. Lachman and anterior-posterior drawer tests were negative, and she remained neurovascularly intact. Physical examination revealed neutral mechanical alignment with a moderate effusion and tenderness to palpation along the medial joint line but was otherwise unremarkable. Radiographic imaging demonstrated a 5.1 × 2.1–cm osteochondral lesion involving the entire medial femoral condyle (Figure 1) with associated subchondral collapse.

(A) Anteroposterior, (B) tunnel, and (C) lateral radiographs of the right knee demonstrating a large osteochondral lesion of the medial femoral condyle with associated subchondral collapse (yellow arrows).
MRI revealed multifocal areas of osteonecrosis in both the medial and lateral femoral condyles. As seen on the radiograph, the medial femoral condyle lesion was associated with subchondral plate collapse and marrow changes on T1-weighted imaging. Imaging showed no collapse and no marrow changes of the lateral femoral condyle lesion (Figure 2). The patient was counseled for alcohol cessation and was provided with services to help her quit drinking prior to any surgical intervention.

(A) Coronal proton density, (B) coronal T2-weighted, fat-suppressed, and (C) sagittal proton density magnetic resonance imaging of the right knee demonstrating a large osteochondral lesion of the medial femoral condyle with underlying osteonecrosis and subchondral collapse (yellow arrows). An additional area of osteonecrosis lay within the lateral femoral condyle without subchondral collapse (arrowheads).
A diagnostic arthroscopy was performed as the first stage of management to evaluate for the size and the stability of the lesion compared with the MRI findings and to better determine the next step in the patient’s care. Direct arthroscopic visualization demonstrated a large, loose lesion involving the entire medial femoral condyle, with an intact lateral femoral condyle. Two weeks after diagnostic arthroscopy, the patient was doing well. Given her findings, the patient consented to medial hemicondyle transplant with a fresh-matched cadaver allograft. Since the lateral femoral condyle was intact and not collapsed, which was confirmed on diagnostic arthroscopy, and the patient had no laterally based knee pain, the decision was made not to address the lateral femoral condyle with surgery. Matching of the medial femoral condyle allograft to the patient was done with measurements taken on both magnetic marker radiographs and direct measurements on the MRI results.
Intraoperative Findings
Two months later, the patient underwent right knee hemicondyle allograft transplant to the medial femoral condyle; the procedure entailed 3 Acutrak headless screws (Acumed) for fixation and an anti-glide plate. Intraoperatively, a medial parapatellar arthrotomy was performed with the patella everted. The medial femoral condyle lesion was identified, measuring about 5 cm in length by 2 cm in width. It was completely loose and mobile (Figure 3). The lesion was removed with a rongeur and an elevator. Next, a sagittal saw was used to flatten the region of the medial femoral condyle down to the bleeding bed of bone for preparation of the allograft transplant (Figure 4). The graft was cut on the back table to exactly match the defect on the patient’s condyle (Figure 5). Three K-wires were used to hold the condyle in place anatomically, and 3 Acutrak screws (two 30-mm screws and one 28-mm screw) were placed into the condyle to affix and compress the graft (Figure 6A). After this was performed, an anti-glide plate was placed just over the region of the femoral condyle by use of a 2.3-mm, 8-hole plate to prevent shearing of the graft (Figure 6, B and C).

Medial parapatellar arthrotomy was first performed with the patella everted. (A) The loose medial femoral condyle lesion was identified, measuring about 5 cm in length by 2 cm in width. (B) After the necrotic lesion was removed, the entire medial femoral condyle was visualized.

(A) A sagittal saw was used to flatten the region of the medial femoral condyle down to the bleeding bed of bone for preparation of the allograft transplant. (B) The fresh matched femoral condyle was held up next to the recipient site.
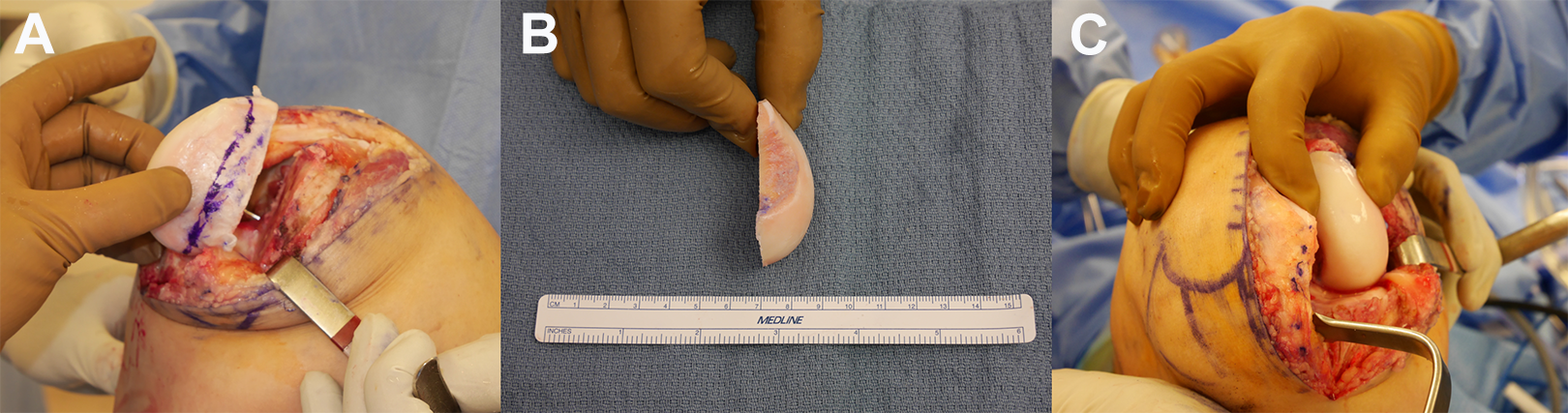
(A) The graft was held up to the recipient and the cut plane was marked. (B) The graft was cut on the back table freehand to match the recipient site. (C) A perfect anatomic match was completed with the graft held up to the medial femoral condyle.
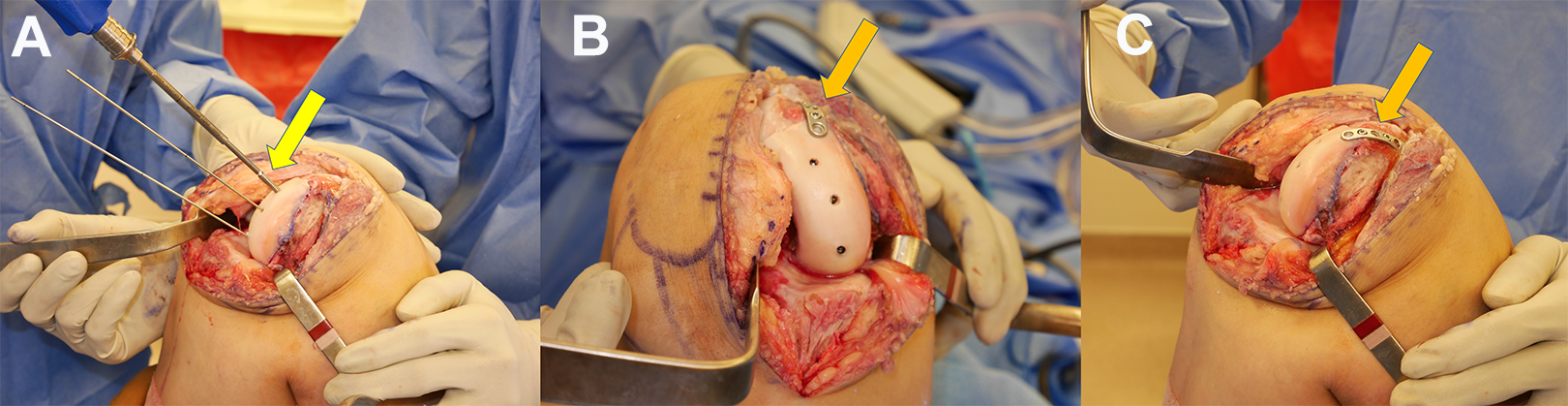
(A) Three K-wires were used to hold the condyle in place anatomically, and 3 Acutrak screws (yellow arrow) were placed into the condyle to affix and compress the graft. (B and C) An anti-glide plate (orange arrows) was placed just over the region of the femoral condyle by use of a 2.3-mm, 8-hole plate to prevent shearing of the graft.
Postoperative Course
The patient’s knee was put in a RoadRunner brace (Breg) locked in extension with toe-touch weightbearing and was given a continuous passive motion machine to use for the first 4 weeks. The patient was transitioned to partial weightbearing between weeks 4 and 6 and then to full weightbearing around week 8. Six weeks postoperatively, the patient had improved ROM from 0° to 90° with minimal effusion. At 3 months postoperatively, the patient reported that she was able to ambulate without pain for the first time in 2 years. She was instructed to continue performing physical therapy. At her 6-month follow-up, she had full ROM, with a modified Cincinnati questionnaire score of 58, Tegner Lysholm knee score of 54, International Knee Documentation Committee (IKDC) subjective knee evaluation score of 49.4, and VAS pain score of zero. At 1-year follow-up, her modified Cincinnati, Tegner Lysholm, and IKDC scores had improved to 88, 96, and 70, respectively, and she continued to have full ROM and a VAS pain score of zero. These were marked improvements from her preoperative scores: modified Cincinnati, 36; Tegner Lysholm, 15; IKDC, 24.1; and VAS, 5. These values are summarized in Table 1. Repeat MRIs were obtained at the 6-month (Figure 7) and 12-month (Figure 8) marks to assess for graft incorporation and healing. These images showed excellent graft incorporation with the native condyle. The patient’s postoperative radiograph at the 1-year follow-up demonstrated graft incorporation (Figure 9).
The Patient’s Knee Function Scores a

a Scores for the modified Cincinnati questionnaire, Tegner Lysholm knee scoring scale, International Knee Documentation Committee (IKDC) knee evaluation, and visual analog scale (VAS) for pain were assessed at 3 time points to evaluate the patient’s knee function.
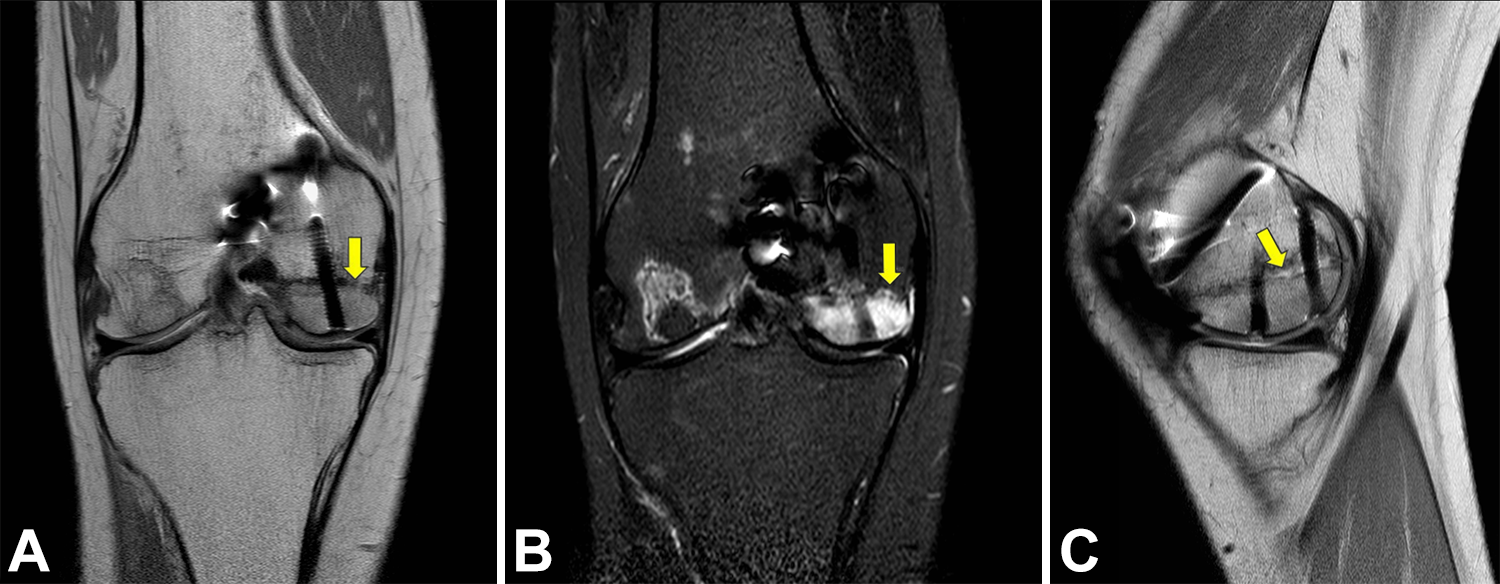
Postoperative (A) coronal proton density, (B) coronal T2-weighted, fat-suppressed, and (C) sagittal proton density magnetic resonance imaging of the right knee at 6 months. A pattern of residual, intense bone marrow edema appeared within the medial femoral condyle allograft, but early bony incorporation was seen with the native bone (yellow arrows).

Postoperative (A) coronal proton density, (B) coronal T2-weighted, fat-suppressed, and (C) sagittal proton density magnetic resonance imaging of the right knee at 12 months with further bony incorporation of the medial femoral condyle allograft. The residual allograft bone marrow edema pattern had decreased in extent and intensity, and no evidence of graft necrosis was seen (yellow arrows).

Postoperative (A) anteroposterior, (B) tunnel, and (C) lateral radiographs of the right knee at 12 months demonstrated bony incorporation of the condyle allograft with the native bone (yellow arrows), and no sclerosis to suggest graft necrosis was seen.
Discussion
Large osteochondral defects, particularly in young patients, are challenging to manage given the poor intrinsic healing properties of hyaline cartilage and the subsequent risk of progression to osteoarthritis. 1 Furthermore, options such as microfracture, drilling, and chondroplasty, which attempt to encourage new fibrocartilage formation, do not offer viable long-term reliability for large lesions due to the tendency for fibrocartilage to compress over time. 2,4,21 Still, the reluctance to move forward with arthroplasty in young patients has encouraged the use of biological alternatives that include whole tissue transfer (autograft vs allograft) or cell-based cartilage repair. While autograft transplant offers better graft incorporation and no host immune response, it is less suitable for large lesions (>3 cm2) due to limited donor-site availability and morbidity. 8,16,17 Autologous chondrocyte implantation, alternatively, can be used for bigger defects, but it is a 2-step procedure that is costly and not optimized for lesions that involve subchondral bone collapse. 18
Osteochondral allograft transplant (OAT) is a single-stage procedure that restores full-thickness hyaline cartilage tissue with subchondral bone while also emulating normal joint architecture. It is also the only biological salvage option available following the failure of cell-based procedures or prior graft implantation. 33 OAT is primarily indicated for lesions measuring more than 2 cm2 and less than 8 cm2 where there is extensive bone loss, violation of the subchondral plate, and underlying subchondral edema. 12 However, when the lesion is large and involves the periphery of the condyle, using a traditional OAT technique may be challenging secondary to noncontainment and possible loosening of the graft over time. OAT has other limitations, particularly with regard to the timely procurement of matched cadaveric bone. Among the 3 storage methods (fresh, cryopreserved, and frozen), fresh grafts are reported to have the best outcomes, as chondrocyte viability decreases from 100% on day 1 to 51.6% by day 60. 3,36 An optimal time frame exists for implantation, which can cause scheduling difficulties. The recommended maximal time from harvest to transplant is 28 days, 25 but given that all grafts must be biologically and serologically screened, a process that generally takes 14 days or more, 12 this gives surgeons roughly a 2-week window for optimal operative intervention. 33
In this case presentation, we report a 25-year-old woman who successfully underwent a right knee hemicondyle transplant of a fresh allograft to the medial femoral condyle to manage osteonecrosis. The senior author (X.L.) decided to proceed with the hemicondyle transplant rather than the traditional OAT with plugs due to the size of the lesion, peripheral involvement, and the depth of the subchondral bone involvement. The hemicondyle graft fixation method included the use of metal headless compression screws and an anti-glide plate to prevent shear of the graft. The decision to use the plate to prevent shear was made to allow the patient early motion in the continuous passive motion machine to decrease the risk of stiffness after surgery. Absorbable compression screws can also be used in this situation. However, cases of cyst formation have been reported in the literature with bioabsorbable screws in tibial fixation after anterior cruciate ligament reconstruction. 11 The senior author was concerned about the risk of cyst formation and catastrophic failure with these bioabsorbable screws, and thus metal headless screws were used. Repeat MRI at 6 and 12 months postoperatively showed excellent graft incorporation. Persistent edema was seen in the allograft on both 6-month and 1-year MRIs but decreased over time. Given the patient’s marked improvement and excellent clinical outcome at more than 1 year following surgery, we believe that this surgical approach offers a viable alternative to joint arthroplasty for treating large osteonecrosis lesions of the femoral condyle in very select young and active patients.
Our findings support a growing consensus within the literature regarding the effectiveness of allograft transplant. Specifically, in a retrospective review of 129 knees in 122 patients (mean age, 32.8 years) after OAT, Levy et al 26 found that allograft survivorship at 10, 15, and 20 years was 82%, 74%, and 66%, respectively. Of all the knees surveyed, 31 (24%) underwent reoperation due to allograft failure, but otherwise, mean IKDC pain scores were significantly improved from 7.0 ± 1.9 to 3.8 ± 2.9, while the mean modified Cincinnati knee score increased from 3.3 to 6.3. Osteonecrosis was the underlying reason for surgery for 19 (14.7%) of these cases. 26 Further, a prospective study that examined 25 consecutive patients with defects measuring greater than 2.5 cm2 who underwent a fresh allograft transplant found that patients were 84% satisfied with their results and believed that their surgically repaired knee functioned 79% as well as their unaffected, contralateral knee. Overall, 22 of 25 (88%) of the grafts showed incorporation into the host bone on follow-up radiographic imaging. 29
In a large-scale systematic review of 19 studies evaluating 644 knees with a mean follow-up of 58 months (range, 19-120 months) and a mean defect size of 6.3 cm2, the patient satisfaction rate was 86%, short-term complication rate was 2.4%, and overall failure rate was 18%. Osteonecrosis accounted for 12% of the surgical cases. 5 Specific to distal femoral osteonecrosis, Flynn et al 9 evaluated 15 patients (17 knees) who underwent fresh-frozen osteoarticular allograft transplant; the patients were younger than 50 years and had a follow-up time of more than 2 years. The investigators determined that 7 knees had excellent results, 5 good results (occasional complaints, unlimited walking without aids, functional range of motion), 1 fair result, (intermittent pain, ambulatory tolerance limited), and 4 failures. No wound complications, infections, or nonunions occurred. 9
Finally, allograft transplant has been shown to be successful for young athletes who wish to continue playing sports. Krych et al 24 retrospectively assessed 43 athletes with an average lesion size of 7.25 ± 2.36 cm2 who underwent an OAT procedure. Thirty-four of the 43 athletes (79%) were able to return to sport at 9.6 ± 3.0 months (range, 7-13 months). However, in the above-mentioned published series, the majority of the procedures were performed with the standard OAT technique and not hemicondyle transplant. Thus, it is difficult to translate their reported outcomes to our case.
In summary, our case demonstrated successful transplant of the medial femoral condyle with fresh allograft, showing both excellent clinical outcome and graft incorporation on MRI at 1-year follow-up. Although this procedure is technically difficult, we recommend considering this option in the management of large osteonecrosis of either medial or lateral femoral condyle in the young and active patient, especially when total or unilateral joint replacement is not indicated because of age.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.M. is a consultant for the Pfizer Anti-Nerve Growth study and Boston Imaging Core Lab. X.L. is a consultant for Tornier, Encore Medical, DePuy, and Stryker and has equity in the Journal of Medical Insight. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.