
Abstract
Background:
Previous studies in the arthroplasty, spine, and shoulder and elbow literature have shown that patients perceive Medicare reimbursement to surgeons to be much higher than current reimbursement schedules.
Purpose:
To evaluate patient perceptions of surgeon reimbursement for various rotator cuff repair (RCR) procedures.
Study Design:
Cross-sectional study.
Methods:
We surveyed 153 patients who presented to a single surgeon’s orthopaedic sports medicine clinic between October 2016 and March 2017. Patients with a new complaint of hip or knee pain, those with a new complaint of shoulder pain, or those who had undergone shoulder surgery 1 year or more prior to their current visit were included. Patients were asked how much they thought surgeons should be reimbursed for RCR procedures, including arthroscopic repair of a simple tear and a massive tear as well as open repair of an acute tear and a chronic tear. They were also asked to estimate how much they thought surgeons were reimbursed by Medicare for these procedures. They were then given actual Medicare reimbursement rates for these procedures and asked whether they believed surgeons should be reimbursed that amount.
Results:
For arthroscopic repair of a rotator cuff tear, patients believed that surgeons should receive a mean (±SEM) reimbursement of US$5645 ± $442. This was significantly more than their estimate of what surgeons were actually reimbursed by Medicare ($3644 ± $408; P = .001). Patients also believed that surgeons should be reimbursed more than their estimate of what surgeons were actually reimbursed for arthroscopic repair of a massive tear ($8066 ± $708 vs $4694 ± $476; P = .0001), open repair of an acute tear ($8428 ± $768 vs $4549 ± $396; P = .00001), and open repair of a chronic tear ($8902 ± $844 vs $4639 ± $438; P = .00001). Both types of patient perceptions were higher than the actual state Medicare reimbursement data for all procedures surveyed (P < .001).
Conclusion:
Consistent with previous literature, patients perceive Medicare reimbursement for RCR to be higher than what surgeons are actually reimbursed. As the United States health care system enters a bundled care environment, price transparency is increasingly important. This study indicates a need for patient education on how their health care costs are allocated.
Keywords
Over the past decade, changes to the health care system in the United States have been a consistent topic of political debate. 1 While the focus of much discussion is on private insurance costs, Medicare serves as the benchmark that private insurance companies use to set reimbursement schedules. 3,8,11,15 Medicare has continued to gradually reduce physician reimbursement, while practice operating costs and cost of living expenses for physicians continue to rise. 5,9,13
Rotator cuff repair (RCR) is a relatively common orthopaedic procedure that is expected to be performed increasingly in the aging Medicare population as patients continue to remain active later in life. 10 The amount that Medicare reimburses for many orthopaedic surgical procedures has declined substantially in recent years, with a 68% decrease in reimbursement for RCR since 1992. 11 Meanwhile, studies in the arthroplasty, spine, and shoulder and elbow literature have shown that patients perceive Medicare reimbursement to surgeons to be much higher than current reimbursement schedules. 1,5,9,13
The purpose of this study was to evaluate patient perceptions of Medicare reimbursement for various RCR procedures. Based on the results of previous studies, we hypothesized that patients would overestimate surgeon reimbursement rates for these procedures. Additionally, we sought to evaluate how these perceptions of reimbursement varied between patients who had previously undergone shoulder surgery versus those presenting with new complaints of shoulder pain or new complaints of hip or knee pain. We hypothesized that patients with previous shoulder surgery would overestimate reimbursement to surgeons relative to other patients. Finally, previous studies have demonstrated that when presented with the actual reimbursement amounts, patients typically believe that surgeons should be paid more to perform these procedures. 1,5,9,13 Thus, we also sought to evaluate whether patients felt this way regarding RCR procedures.
Methods
Following institutional review board approval, 153 patients who presented to a single surgeon’s orthopaedic sports medicine clinic between October 2016 and March 2017 were surveyed. Upon presentation for their regularly scheduled visit, patients’ medical records were screened by a research fellow (B.R.S.) to determine whether inclusion criteria for the study were met. Inclusion criteria included patients presenting with a new complaint of hip or knee pain, those with a new complaint of shoulder pain, or those who had undergone shoulder surgery 1 or more years before their current visit. If these criteria were met, patients were approached by the research fellow and asked to complete a voluntary, confidential survey on patient perceptions of surgeon reimbursement while they were waiting to be seen by the surgeon. Those who chose to participate were given a paper survey, which they completed and returned to the research fellow or office staff to maintain anonymity with the treating surgeon.
Surveys were modeled after similar, previously conducted studies 1,5,9,14 and were divided into 4 sections (Appendix). In the first section, basic demographic data were collected, including age, sex, race, insurance status, annual household income level, highest level of education, and history of previous orthopaedic surgeries.
In the second section of the survey, patients were asked to estimate how much they thought surgeons should be reimbursed for various RCR procedures, including arthroscopic repair of a simple tear, arthroscopic repair of a massive tear, open repair of an acute tear, and open repair of a chronic tear. Patients were also later asked how much surgeons should be reimbursed for other common surgical procedures, including laparoscopic cholecystectomy and mitral valve replacement. For each of these surgeries, patients were then asked in the next question how much they thought the actual Medicare reimbursement to surgeons was.
The third section provided patients with the actual state reimbursement data from Medicare for the previously described operations based on the following Current Procedural Terminology (CPT) codes: 29827, 23410, 23412, 47562, and 33430. 4 This section of the survey was on the pages that followed section 2 so as not to influence patient responses regarding perceived reimbursement. Patients were asked whether they believed surgeons should be reimbursed more or less than the given Medicare reimbursement amount.
In section 4, patients were asked to provide their opinion on whether surgeons are fairly reimbursed by Medicare and whether surgeons will continue to accept Medicare patients based on the reimbursement data. Finally, patients were asked if they were aware of the 90-day global period, in which a surgeon does not receive any additional payments from Medicare for office visits which take place up to 90 days after surgery.
All data were entered into Microsoft Excel for statistical analysis. Demographic data were analyzed by use of basic descriptive statistics. For section 2, which compared patients’ estimates of surgeon reimbursement versus what they believed physicians should be reimbursed for various RCR surgeries, t tests were conducted to compare these responses, and P < .05 was considered significant. Additional t tests were conducted to compare actual state Medicare reimbursement amounts to these responses using the Real Statistics Resource Pack software (release 5.1) single-sample t test. Additionally, a 1-way analysis of variance (ANOVA) was performed to compare responses between each group of patients (new hip or knee pain, new shoulder pain, and previous shoulder surgery) for each of the RCR surgeries. As well, t tests were conducted to compare the responses between each of these groups. To control for outliers, the highest and lowest 5% of patient responses for each question were excluded prior to analysis.
Results
The 153 patients surveyed had a mean age of 52.5 years (range, 18-85 years); 70 male patients (45.8%) and 83 female patients (54.2%) were included in the study. Most patients had either private insurance (93/153, 60.8%) or Medicare (33/153, 21.6%) (Figure 1). The median patient income was $75,000-$100,000 (Figure 2). The breakdown for highest level of education is shown in Figure 3. Overall, 104 patients (68.0%) had undergone previous orthopaedic surgery.

Insurance type of respondents.

Annual household income of respondents.

Highest level of education of respondents.
For arthroscopic repair of a rotator cuff tear, patients believed that surgeons should receive a mean reimbursement of US$5645, which was significantly more than their estimate of what surgeons were actually reimbursed by Medicare ($3644, P = .001). Patients also believed that orthopaedic surgeons should be reimbursed more than their estimate of what surgeons were reimbursed for arthroscopic repair of a massive tear ($8066 vs $4694, P = .0001), open repair of an acute tear ($8428 vs $4549, P = .00001), and open repair of a chronic tear ($8902 vs $4639, P = .00001). Patients also indicated that general surgeons and cardiothoracic surgeons should be reimbursed significantly more than their estimate of what these surgeons were reimbursed for laparoscopic cholecystectomies ($5789 vs $3264, P = .00001) and for mitral valve replacements ($18,089 vs $10,333, P = .00005), respectively. While patients believed that surgeons should be reimbursed more for an arthroscopic repair of a massive tear compared with a simple tear ($8066 vs $5645, P = .004), no other significant differences were observed between the RCR procedures. When comparing the responses between the 3 patient groups (new hip/knee pain, new shoulder pain, and previous shoulder surgery), there were no significant differences regarding what the patients believed surgeons should be reimbursed versus their estimate of reimbursement, for any procedure (Figure 4).
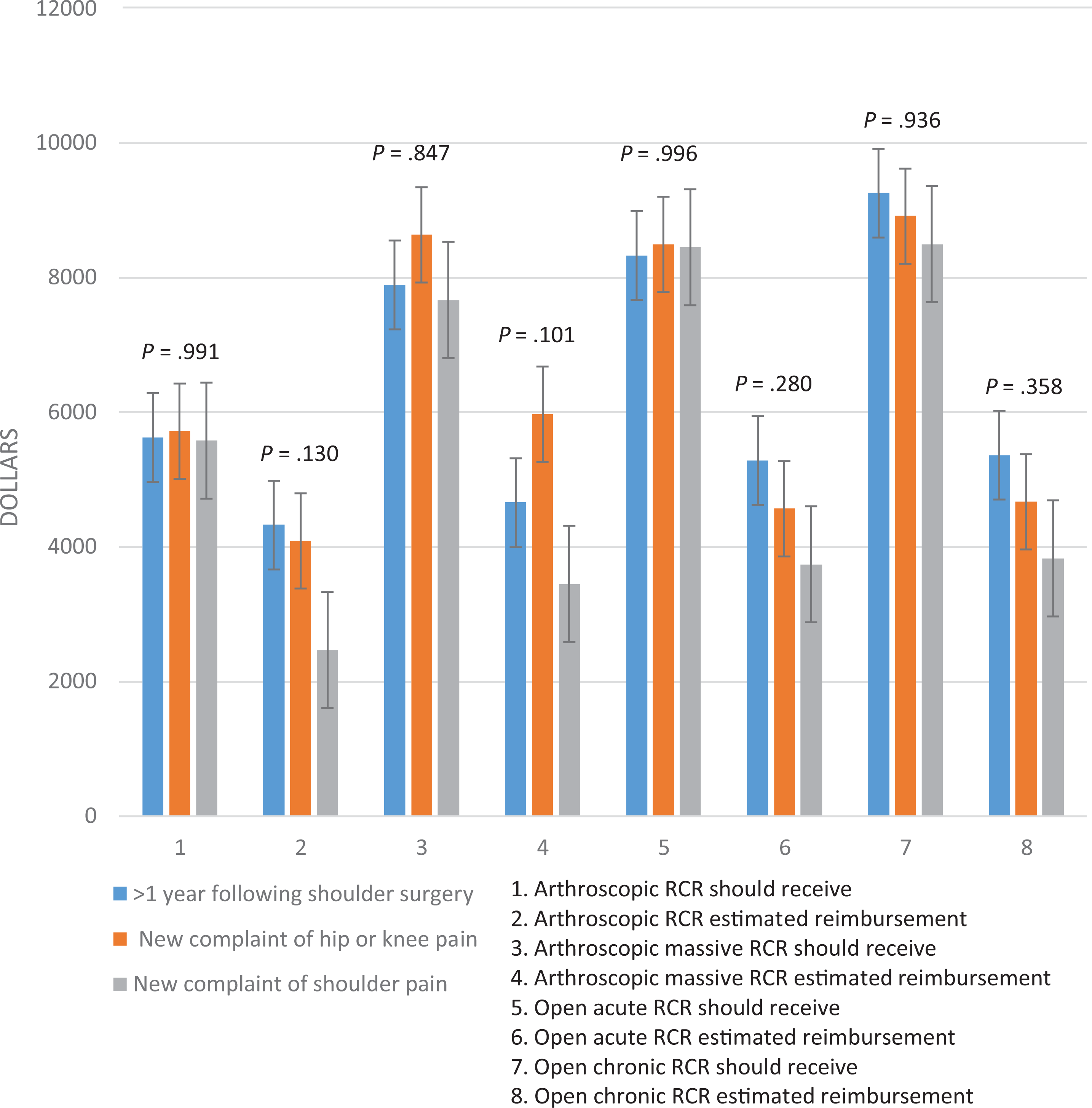
Analysis of variance (ANOVA) comparison of patient perceptions of reimbursement between groups. The ANOVA conducted found no significant difference in patient perceptions of reimbursement for each of the procedures between the 3 groups surveyed. However, t tests performed between each of the groups revealed a significant difference between what group 1 and group 3 thought Medicare reimbursed surgeons for arthroscopic repair of simple tears (question 2, P < .027). RCR, rotator cuff repair.
When we compared the patients' estimated reimbursement and the amount they believed that surgeons should be reimbursed with the actual state Medicare reimbursement data, we found that patients significantly overestimated both of these values for all 6 surgeries (Table 1). All P values were less than .001. Patient responses for estimated reimbursement versus what they believed surgeons should be reimbursed for each of the RCR procedures were evaluated according to the type of insurance the patient had (Table 2). Responses were also evaluated according to highest education level (Table 3) and annual household income level (Table 4). Comparing patients with private insurance versus those with Medicaid, Medicare, and workers’ compensation, we noted no significant differences between groups with regard to how much these patients believed surgeons should be reimbursed for each of the procedures. Similarly, when comparing patients who had undergone previous orthopaedic surgery versus those with no history of orthopaedic surgery, we found no significant differences between groups for each procedure.
Patient Reimbursement Responses Versus Actual State Medicare Reimbursement a

a Values for “patient response,” “actual state Medicare reimburesment,” and 95% CIs are in US$. RCR, rotator cuff repair.
Patient Reimbursement Responses by Insurance Type a
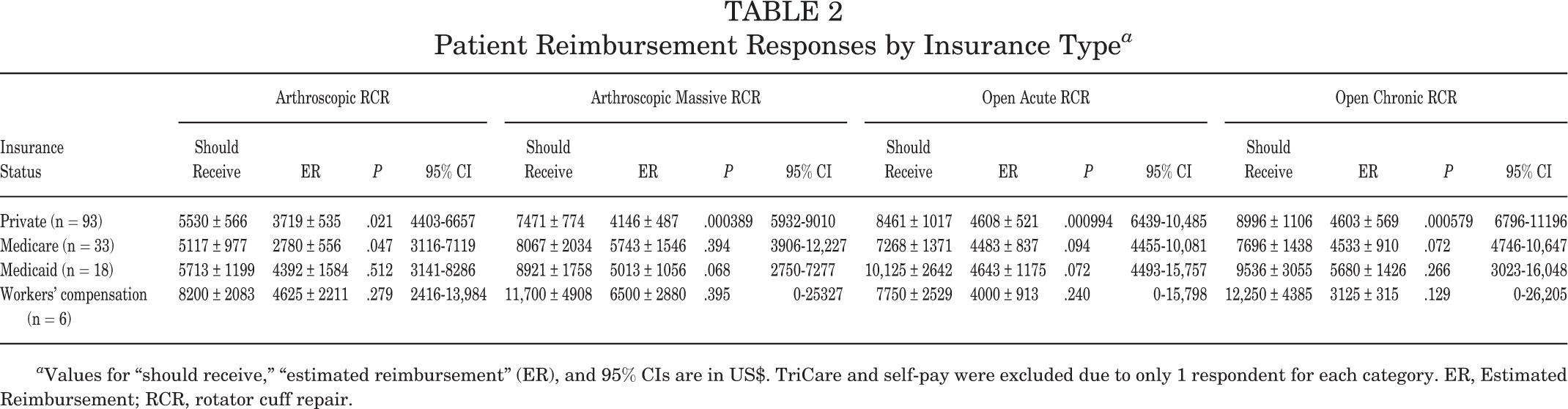
a Values for “should receive,” “estimated reimbursement” (ER), and 95% CIs are in US$. TriCare and self-pay were excluded due to only 1 respondent for each category. ER, Estimated Reimbursement; RCR, rotator cuff repair.
Patient Reimbursement Responses by Highest Education Level a
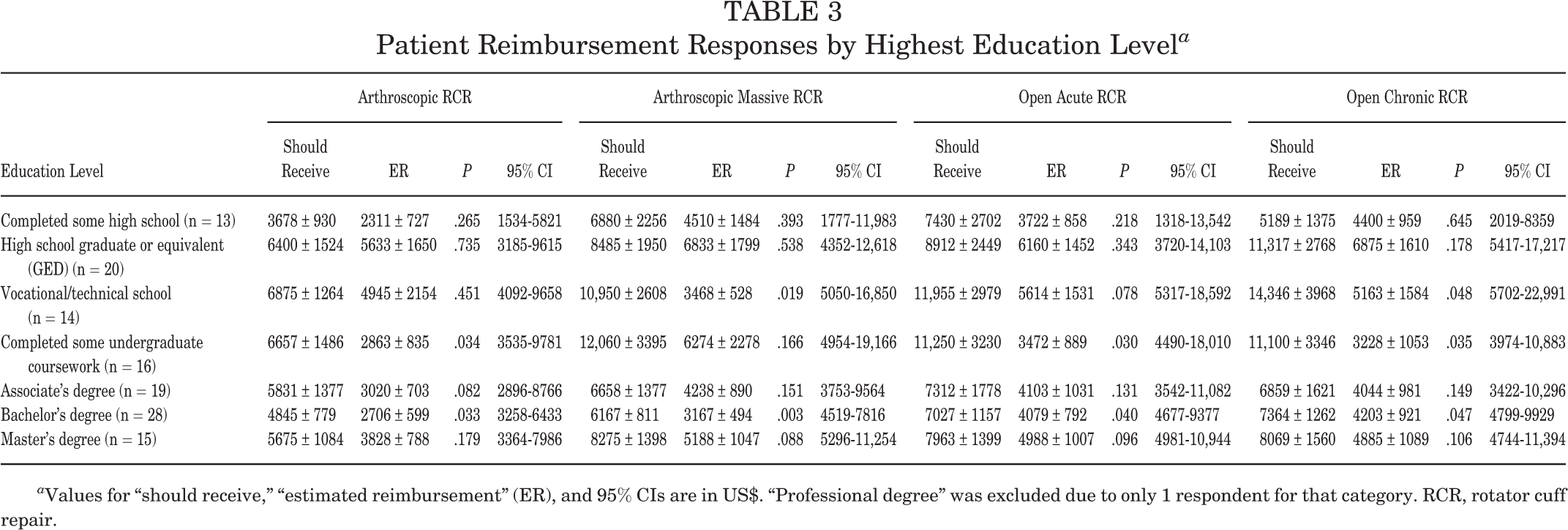
a Values for “should receive,” “estimated reimbursement” (ER), and 95% CIs are in US$. “Professional degree” was excluded due to only 1 respondent for that category. RCR, rotator cuff repair.
Patient Reimbursement Responses by Annual Household Income Level a

a Values for “annual household income,” “should receive,” “estimated reimbursement” (ER), and 95% CIs are in US$. RCR, rotator cuff repair.
When given the actual Medicare reimbursement (MR) rates for arthroscopic repairs, 71% of patients believed reimbursement should be higher for simple tears (MR, $1052) and 84% believed it should be higher for massive tears (MR, $1052). For open repairs, 86% of patients believed reimbursement should be higher for repair of acute tears (MR, $816) and 88% believed it should be higher for repair of chronic tears (MR, $846). Sixty-eight percent of patients believed that surgeons were not fairly reimbursed, and 44% believed that surgeons would no longer continue to see Medicare patients based on current reimbursement. Seventy-eight percent of patients who participated in this study were unaware of the global period prior to completing the survey.
Discussion
Previous research has indicated that patients believe physicians are largely overpaid; however, more recent research suggests that patients think surgeons should be reimbursed 4 times current reimbursement rates. 5,12 This study sought to evaluate patient perceptions of surgeon reimbursement for RCR procedures and how these were influenced by previous RCR versus patients presenting with new complaints. Additionally, patients were given actual reimbursement data for these procedures and asked to provide their opinion on whether surgeons should be reimbursed that amount for each procedure. Considering previous research, we hypothesized that patients would overestimate the actual amount that Medicare reimburses for each of the procedures described in the questionnaire. Consistent with the literature, patients in this study perceived Medicare reimbursement for RCR to be much higher than it actually is and believed that reimbursement should be much higher than it is currently. 1,5,9,13
This effect was observed across all RCR procedures. Nagda et al 9 demonstrated that patients estimate Medicare reimbursement for RCR surgery to be approximately 3 times the amount that orthopaedic surgeons are actually reimbursed ($4692 vs $1175). Foran et al 5 found that patients overestimate the reimbursement for total hip arthroplasty and total knee arthroplasty by a factor of approximately 6 times for each procedure. Despite patient perceptions, Medicare reimbursements to orthopaedic surgeons continue to decline. 2,6,7,11
When patients in the current study were provided with the actual reimbursement data for each of the RCR procedures, between 71% and 88% of patients believed that orthopaedic surgeons should be reimbursed more than the actual Medicare reimbursement depending on the procedure. In contrast, only approximately 4% of patients thought that surgeons were overreimbursed for any RCR procedure. These results are similar to the results of Nagda et al, 9 who found that 75.7% of patients believed that reimbursement for RCR was lower than it should be, while 11.8% believed that reimbursement was fair and 2.5% believed it was more than it should be. However, these findings are in contrast to previous work by Ross and Lauritsen 12 from 1985, which indicated that approximately 70% of the general public believed that physicians were paid too much, preceded only by movie stars, professional athletes, and top executives. As previous authors have noted, these differences may reflect a changing public perception of physician reimbursement that has taken place over the past 30 years. 5,9 Additionally, it is possible that patients believe that subspecialized surgeons should receive increased reimbursement commensurate with their increased level of training. 9 However, it is not possible to draw these conclusions from the present study.
A secondary goal of this study was to identify whether any differences existed in perceptions about surgeon reimbursement between each of the groups surveyed: patients with a new complaint of hip or knee pain, those with a new complaint of shoulder pain, and those who had undergone shoulder surgery 1 or more years before their current visit. The single-factor ANOVA that was performed revealed no significant differences for either the estimated Medicare reimbursement or the reimbursement amount that patients believed surgeons should receive between the 3 groups. The t tests performed between each of the groups revealed a significant difference in the amount that patients with a previous shoulder surgery versus those with a new complaint of shoulder pain thought Medicare reimbursed surgeons for arthroscopic repair of simple tears ($4326 vs $2469, P = .027). Although not significant, a similar trend was observed between these 2 groups for the amount that they believed Medicare reimbursed surgeons for each of the RCR procedures. This difference may be attributable to the perceived value that patients with previous shoulder surgery placed on the procedure. Alternatively, this difference may have been a result of the fact that patients who had undergone shoulder surgery were aware of their overall previous medical expenses and therefore used that amount as the frame of reference upon which they estimated Medicare reimbursement, causing them to estimate a higher amount.
In this study, patients appeared to place a higher value on the amount they believed that cardiothoracic surgeons should be reimbursed for mitral valve replacement relative to the amount they believed orthopaedic surgeons should be reimbursed for RCR. This finding is consistent with previous studies reporting that patients believe surgeons should be reimbursed more for coronary artery bypass graft surgery relative to both total shoulder arthroplasty and RCR as well as total hip arthroplasty and total knee arthroplasty. 5,9 However, these studies also found that patients placed a lower value on appendectomy relative to those aforementioned procedures, indicating that they have some understanding of the relative complexity of these procedures. In contrast, our patients placed a similar value on laparoscopic cholecystectomy relative to arthroscopic RCR of a simple tear, which may indicate a belief that these procedures require a relatively similar level of technical skill and expertise. In this study, patients also believed that arthroscopic RCR of a massive tear should receive a significantly higher reimbursement than arthroscopic RCR for a simple tear, indicating an appreciation for the increased complexity associated with the repair of a larger tear.
Previous survey studies have reported that patients had independently expressed their concern over surgeons continuing to see Medicare patients in light of current reimbursements. 1,5 Therefore, we sought to quantitatively measure the number of patients we surveyed who felt this way. We found that nearly half our population did not think surgeons would continue to accept Medicare based on current reimbursement, which they believed was too low. Additionally, several patients who had Medicare insurance indicated on their survey that they hoped their surgeon would continue to accept Medicare reimbursement and therefore disagreed with the question based on those grounds. These findings suggest that patients are growing concerned over whether their surgeon will continue to take their insurance. A previous study demonstrated that patients have a poor understanding of the global period, with nearly 75% of patients assuming that orthopaedic spine surgeons are reimbursed for all postoperative appointments that occur within the first 3 months after surgery. 14 Given that this is an important concept in understanding physician reimbursement, we also decided to assess patient understanding of the global period in our survey population and found that nearly 80% of patients were unaware of the global period. Interestingly, this did not appear to be influenced by highest level of education, annual household income level, or history of previous orthopaedic surgery.
Limitations
Our study has several limitations that should be noted. First, we had a limited number of respondents (N = 153 patients) from a geographically distinct area in southwest Ohio, which is likely not representative of the general United States population. Second, approximately 30% of patients who met inclusion criteria chose not to participate in the study due to their own perceived lack of knowledge about surgeon reimbursement or a general lack of interest in participating. Thus, the population who chose to participate in the study may have biased the results. Prior to completing the survey, patients were reassured that the results of the survey were confidential. However, since the survey was administered in the surgeon’s office prior to the patients’ scheduled clinic visit, some patients might have perceived that their responses would influence the subsequent care they received, which may have affected their responses. Third, the format of the survey may have influenced responses, given that the survey asked patients what a surgeon should be reimbursed and then immediately asked for an estimate of what Medicare actually reimburses. Patients may have assumed that actual reimbursement was less than what they believed reimbursement should be and may have answered the questions based on that assumption.
Conclusion
The results of this survey indicate that patients believe surgeon reimbursement should be much higher than actual current Medicare reimbursement rates. This effect was observed across all RCR procedures irrespective of insurance, education level, or median household income. As the United States health care system enters a bundled care environment, price transparency is increasingly important, particularly in the elective surgery setting. This study indicates an increasing need for patient education on how health care costs are allocated.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.S. has received research support from DePuy Synthes. B.M.G. has received educational support from Arthrex and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Cincinnati Institutional Review Board (IRB ID: 2016-5240).