
Abstract
Background:
Evaluations of the stability of osteochondritis dissecans (OCD) lesions of the elbow using magnetic resonance imaging (MRI) have resulted in reports with variable accuracy. Therefore, the International Cartilage Repair Society (ICRS) classification remains the gold standard to determine OCD lesion stability. Because OCD commonly occurs in pediatric patients, a noninvasive method comparable with the ICRS classification is desired.
Hypothesis/Purpose:
Based on the previous literature, the capitellum of unstable OCD lesions has an irregular outline on MRI because of displacement or dislocation of the lesion via synovial fluid inflow. Therefore, we defined a 4-stage classification, similar to the ICRS classification, which focused on the outline of the capitellum and articular cartilage status on MRI without subchondral bone information. The purpose of this study was to validate this MRI-based staging system against the ICRS classification and to verify its accuracy in diagnosing unstable OCD lesions of the elbow.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
A total of 81 patients with OCD of the elbow who were surgically treated were evaluated. The MRI-based stages were as follows: stage 1, normal-shaped capitellum and articular cartilage without signal intensity change; stage 2, normal-shaped capitellum and articular cartilage with signal intensity change; stage 3, irregular-shaped capitellum and discontinuity of the articular cartilage; and stage 4, dislocated lesion with an articular cartilage defect. Agreement between the MRI and ICRS classifications was evaluated, and the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for lesion instability were determined. The intraclass correlation coefficient (ICC) for intrarater and interrater reliability of the MRI-based staging system was calculated.
Results:
Agreement between the MRI-based staging system and the ICRS classification was 88.9%, with a sensitivity of 98.4%, specificity of 84.2%, PPV of 95.3%, and NPV of 94.1% for diagnosing an unstable lesion. The ICC was high for both intrarater (0.925) and interrater (0.915-0.939) reliability.
Conclusion:
The MRI-based staging system corresponded well with the ICRS classification, providing an accurate preoperative assessment of OCD lesions of the elbow, even with minimal subchondral bone information.
Osteochondritis dissecans (OCD) of the elbow is an uncommon condition that typically occurs at the humeral capitellum, 20 causing pain and swelling on the lateral aspect of the elbow in adolescents and young adults. 5 OCD is currently recognized as a subchondral bone lesion without evidence of acute trauma and is characterized by various degrees of osseous collapse, resorption, and sequestrum formation, which often involves articular cartilage delamination. 9 OCD of the elbow usually occurs in young athletes involved in overhead-throwing sports, such as baseball, at a time when the epiphyseal growth plate is open. 3,11 The causes of OCD of the elbow are regarded as multifactorial; they include repetitive valgus stress applied to the poorly vascularized capitellum, vascular inflammation, genetic factors, and other factors that are currently unidentified. 9,20
The treatment options for OCD of the elbow depend on several aspects, including the size, location and stability of the lesion, as well as the severity of symptoms. 6,20 Clinically, the stability of an OCD lesion is considered the most important factor in determining the treatment options. 6,9,11,18,20 In general, stable lesions may be reversible and may heal completely with nonoperative treatment, while unstable lesions require surgical treatment. For operative treatment, the following options are considered: arthroscopic debridement of the lesion, subchondral drilling (bone marrow stimulation), and refixation of the fragments or autologous osteochondral transplantation. 6,20 The invasive aspect of surgery varies depending on the procedure. The correct grading and diagnosis of the lesions allow surgeons to select the most appropriate treatment. Currently, the International Cartilage Repair Society (ICRS) classification is the gold standard for assessing lesion stability, 2,10,18 and it is determined intraoperatively under either arthroscopic or direct observation.
Because OCD of the elbow most frequently presents in adolescents, a noninvasive method to assess the instability of an OCD lesion would be clinically meaningful. Plain radiography, computed tomography (CT), and magnetic resonance imaging (MRI) are widely used to evaluate OCD lesions of the elbow. Plain radiography is useful to determine the basic severity of the OCD lesion at the capitellum 13,17,19 but provides only single-plane information, which does not always correspond to the instability of the lesion assessed intraoperatively. 11 CT can assess the properties of bone fragments, the location of loose bodies within a joint, and the condition of the subchondral bone, such as sclerosis. 18,21 However, CT cannot provide sufficient information regarding changes in the articular cartilage associated with an OCD lesion. Several previous studies have used MRI to predict the instability of the OCD lesion. 8,11,14,15 According to these reports, the presence of synovial fluid inflow between the loose fragment and the floor of the OCD lesion, where the loose fragment originally existed, is an important factor when determining lesion instability. However, MRI findings on the subchondral bone condition vary in each patient, leading to uncertainty regarding the best treatment option to pursue. Iwasaki et al 12 concluded that MRI alone cannot provide a reliable assessment of OCD lesion instability.
Since 2009, we have routinely performed high-resolution MRI using a microscopy coil for the assessment of OCD of the elbow. Using the accumulated imaging data set, we aimed to construct a new MRI-based staging system that is simple and comprises easy-to-identify stages that correspond well to the ICRS classification. Based on the previous literature regarding MRI features of OCD lesions 8,11,14,15 as well as the ICRS classification, 10 it was believed that unstable OCD lesions would show an irregular outline of the capitellum on MRI because of displacement or dislocation of the lesion via synovial fluid inflow. 8,10,11,14,15 Therefore, in this study, we minimized the utilization of subchondral bone information and mainly focused on the outlines of the capitellum and the intensity changes of the articular cartilage. Per the ICRS classification, we subdivided our system into 4 stages based on the condition of the OCD lesion.
The purposes of our study were to validate our MRI-based staging system against the ICRS classification and to evaluate its accuracy and reliability in diagnosing an unstable OCD lesion.
Methods
Study Group
This study was carried out in accordance with the World Medical Association’s Declaration of Helsinki and was approved by the institutional review board of our hospital. We enrolled 81 patients who underwent surgery for OCD of the elbow from August 2009 to December 2014. The characteristics of the patients are presented in Table 1. The period from onset of symptoms to hospital admission ranged from 4 to 1825 days (mean, 413.3 ± 473.4 days), and the period from hospital admission to surgery ranged from 3 to 1484 days (mean, 141.8 ± 230.7 days). The period from MRI to surgery ranged from 1 to 86 days (mean, 19.1 ± 18.8 days). There were 48 patients who underwent conservative treatment at a different facility before being seen at our hospital; the treatment included abstaining from aggravating movements for a minimum of 6 months. In addition, there were 19 patients who failed conservative treatment at our hospital before surgery, including 12 patients who were previously treated conservatively at a different facility. There were 26 patients who presented with an advanced OCD lesion, and these patients were designated for early surgical intervention, as the healing potential is extremely low in advanced OCD cases. 16,19 The majority of patients underwent MRI several times at our hospital. For this study, we evaluated the most recent MRI scans obtained before surgery.
Patient Characteristics (N = 81) a

a Data are presented as No. unless otherwise specified.
MRI-Based Staging System
Preoperative high-resolution MRI of the elbow was performed for all patients. Patients were placed in a supine position with their elbow at full extension and forearm at neutral rotation. From August 2009 to March 2014, a 1.5-T MRI scanner (MAGNETOM Symphony; Siemens) and a microscopy coil (Loop Flex Coil; Siemens) were used for the assessment. Sagittal-plane proton density–weighted (PDW) images, T2 star–weighted (T2*W) images, and T2-weighted fat-saturated (T2WFS) images were obtained using 1.4 mm–thick slices with a 0.3-mm gap between slices, a 60-mm field of view, and a 256 × 141 matrix size. After April 2014, a 3-T MRI scanner (MAGNETOM Skyra; Siemens) and a microscopy coil (4-channel Special Purpose Coil; Siemens) were used. Sagittal-plane PDW images were obtained using 1.5 mm–thick slices with a 0.3-mm gap between slices, a 60-mm field of view, and a 320 × 256 matrix size. T2*W images were obtained using 1.5 mm–thick slices with a 0.3-mm gap between slices, a 60-mm field of view, and a 320 × 160 matrix size. T2WFS images were obtained using 1.5 mm–thick slices with a 0.3-mm gap between slices, a 60-mm field of view, and a 256 × 141 matrix size.
These imaging protocols were designed to maximize the evaluation of the capitellum’s outline and the articular cartilage condition. The articular cartilage is most clearly depicted in PDW images; therefore, the outlines of the capitellum and intensity changes of the articular cartilage were mainly evaluated via PDW images. Because T2*W images and T2WFS images show synovial fluid at high intensity, these were used as auxiliary evaluations of the outline of the capitellum.
Four OCD lesion stages were defined from the MRI scans, focusing on the outline of the capitellum and the intensity changes of the articular cartilage. In grading the MRI-based stages, images obtained under the 3 imaging protocols were comprehensively evaluated and classified.
The 4 MRI-based stages are defined in Table 2 and are summarized as follows: stage 1, normal (circular)–shaped capitellum with no change in the intensity of the articular cartilage, corresponding to ICRS class I (Figure 1); stage 2, normal (circular)–shaped capitellum with a change in the intensity of the articular cartilage, corresponding to ICRS class II (Figure 2); stage 3, irregular-shaped capitellum with an observable discontinuity or displacement of the articular cartilage as well as the subchondral bone, corresponding to ICRS class III (Figure 3); and stage 4, a completely dislocated OCD lesion with an articular cartilage defect, corresponding to ICRS class IV (Figure 4). In our MRI-based staging system, we consider stages 1 and 2 stable lesions and stages 3 and 4 unstable lesions, per the ICRS classification.
Our MRI-Based Staging System a

a MRI, magnetic resonance imaging.
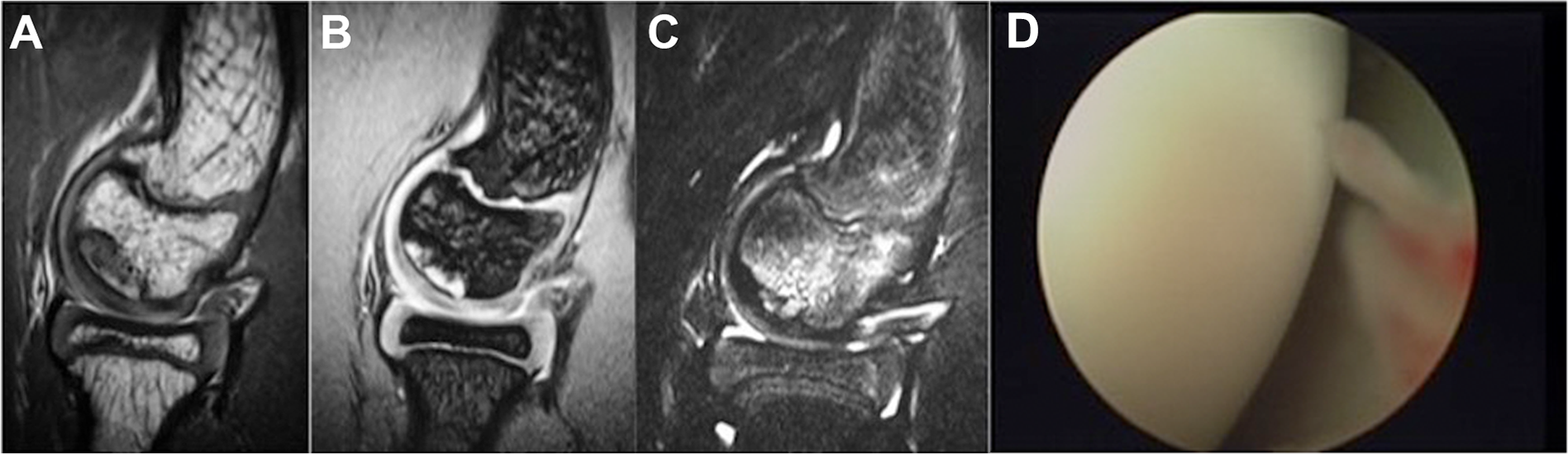
Representative magnetic resonance imaging of stage 1 in a 12-year-old boy. (A) The proton density–weighted image shows that the capitellum has a circular shape and no evidence of an abnormality of the articular cartilage. The osteochondritis dissecans lesion was identified beneath the articular cartilage on the (B) T2 star–weighted image and (C) T2-weighted fat-saturated image. (D) Intraoperative arthroscopic view of the lesion showed no abnormalities of the articular cartilage.

Representative magnetic resonance imaging of stage 2 in a 12-year-old boy. (A) The proton density–weighted image shows that the capitellum had a circular shape but with a low intensity vertical line that was visible across the articular cartilage at the superior edge of the osteochondritis dissecans lesion. (B) Enlarged view of the low intensity line within the cartilage (arrow). (C) T2 star–weighted image. (D) T2-weighted fat-saturated image. (E) Intraoperative arthroscopic view of the lesion with visible damage of the joint cartilage but with no instability.
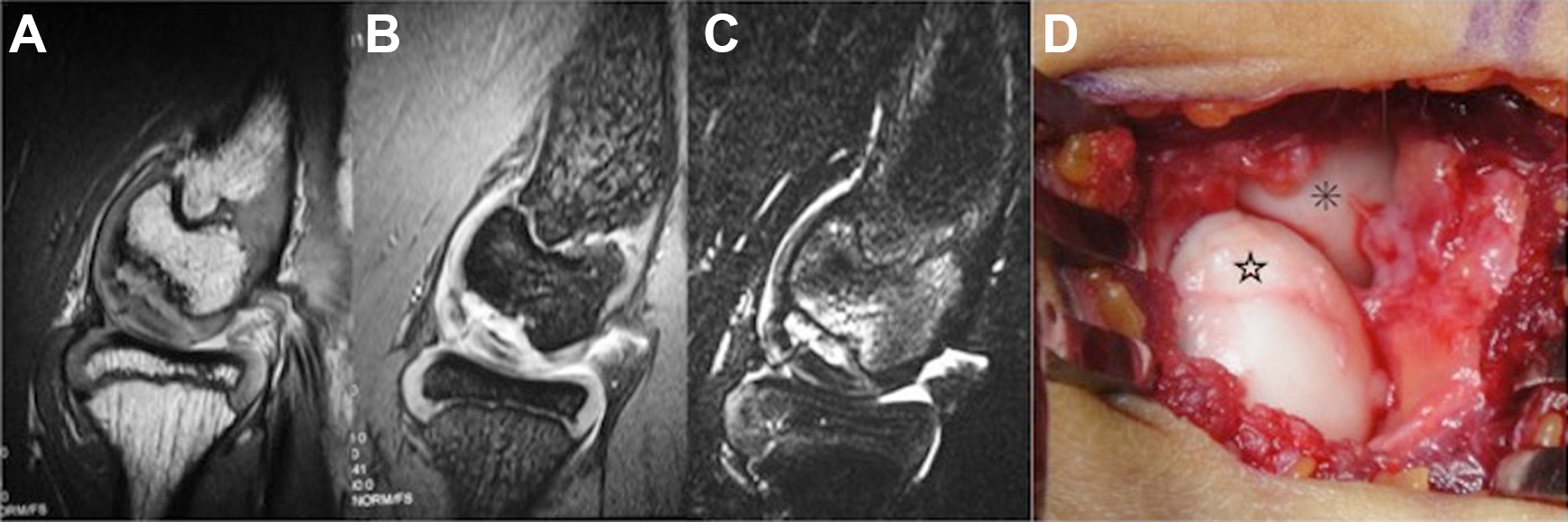
Representative magnetic resonance imaging of stage 3 in a 12-year-old boy. (A) The proton density–weighted image shows the irregular shape of the capitellum with a displaced osteochondritis dissecans lesion. (B) T2 star–weighted image. (C) T2-weighted fat-saturated image. (D) Intraoperative photograph of the lesion with evidence of displacement and an irregular shape of the articular cartilage; the lesion was considered unstable via palpation. ☆, displaced lesion; *, radial head.

Representative magnetic resonance imaging of stage 4 in a 14-year-old boy. (A) The proton density–weighted image shows the irregular shape of the capitellum with evidence that the osteochondritis dissecans lesion had dislocated. (B) T2 star–weighted image. (C) T2-weighted fat-saturated image. (D) Intraoperative photograph of the lesion showing that it had dislocated from the floor and become unstable. *, dislocated lesion.
Intraoperative ICRS Classification
All OCD lesions were evaluated under either arthroscopic or direct observation to determine the ICRS classification, defined as follows: Stable lesions with a continuous but softened area covered by cartilage, deemed as normal for elasticity on both visual inspection and palpation, were classified as ICRS class I lesions. Lesions with a partial discontinuity that was visually observed but deemed stable on palpation were classified as ICRS class II lesions. Lesions with a complete discontinuity of the fragment from the underlying articular cartilage but were not yet dislocated (dead in situ) were classified as ICRS class III lesions. Empty defects, as well as defects with a dislocated or loose fragment within the cartilage bed were classified as ICRS class IV lesions. 4,10 Generally, ICRS classes I and II are considered stable lesions, with classes III and IV considered unstable lesions.
Assessment of the MRI-Based Staging System
Two orthopaedic surgeons (S.K., N.M.) evaluated the MRI scans and determined the MRI-based stage. Assessors were blinded to the preoperative history, symptoms, physical examination results, and operative findings. One of the assessors (S.K.; examiner 1) evaluated MRI findings twice, at least 2 weeks apart. The first assessment was labeled as examiner 1-1, with the second assessment labeled as examiner 1-2. The assessment by the other examiner (N.M.) was labeled as examiner 2.
We evaluated the intrarater and interrater reliability of our MRI-based staging system using the intraclass correlation coefficient (ICC). The interpretation of ICC values was based on criteria proposed by Bartko, 1 defined as follows: 0.00-0.20, slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and ≥0.81, almost perfect agreement.
The accuracy of our MRI-based staging system relative to the ICRS classification was evaluated. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of our MRI-based staging system for the diagnosis of OCD lesion instability were also evaluated. The results obtained from the first trial by examiner 1 (examiner 1-1) were used for these analyses.
Results
The reliability of our MRI-based staging system was high, with an intrarater ICC of 0.925 (examiner 1-1 and examiner 1-2) and interrater ICCs of 0.939 (examiner 1-1 and examiner 2) and 0.915 (examiner 1-2 and examiner 2). The grading of all 81 patients using our MRI-based staging system and the ICRS classification is presented in Table 3, and the agreement between our MRI-based staging system and the ICRS classification is shown in Table 4. Our MRI-based staging system yielded an 88.9% (72/81) agreement with the ICRS classification. With regard to the identification of unstable OCD lesions, our MRI-based staging system yielded a sensitivity of 98.4% and specificity of 84.2%, with a PPV and NPV of 95.3% and 94.1%, respectively.
Grading of the MRI-Based Staging System Versus the ICRS Classification a

a ICRS, International Cartilage Repair Society; MRI, magnetic resonance imaging.
Agreement Between the MRI-Based Staging System and the ICRS Classification a

a Data are presented as No. ICRS, International Cartilage Repair Society; MRI, magnetic resonance imaging.
Discussion
MRI is useful for detecting early stage changes in OCD lesions and assessing the size and location of the lesion, the presence of joint effusion, the condition of the subchondral bone, and discontinuity of the articular cartilage over the OCD lesion. 6,11,15 Evaluating the stability of the OCD lesion is important to determine the best treatment option for a patient. Generally, unstable lesions require surgical treatment, while stable lesions may heal with conservative treatment. 16,19
The application of MRI to identify potentially unstable OCD lesions has previously been reported. Kijowski and De Smet 15 reported evidence that unstable OCD lesions have a peripheral rim of high signal intensity or an underlying fluid-filled cyst on T2-weighted images. Similarly, Jans et al 14 reported MRI features of unstable OCD lesions as multiple underlying cysts or a large underlying cyst >5 mm, a peripheral rim of T2 signal intensity as high as joint fluid, breaks in the subchondral bone plate, and an osteochondral fracture line with T2 high signal intensity or a fluid-filled osteochondral defect. Dipaola et al 8 classified MRI findings of OCD lesions into the following 4 categories: grade I, lesions with no break in the articular cartilage or with thickening of the articular cartilage were classified; grade II, lesions with an articular cartilage breach and a low signal rim behind the fragment, indicating a fibrous attachment; grade III, lesions with an articular cartilage breach with T2 high signal changes behind the fragment, suggestive of fluid behind the lesion; and grade IV, lesions with a loose body and defect of the articular surface. Upon review of these reports, it appears that the key factor in identifying instability of the OCD lesion is determining the presence or absence of an inflow of synovial fluid between the lesion and the floor of the OCD lesion.
Iwasaki et al 12 evaluated the staging systems proposed by De Smet et al 7 and Dipaola et al. 8 The classification system proposed by De Smet et al 7 had a sensitivity of 89%, specificity of 44%, PPV of 76%, and NPV of 67%. In contrast, the classification proposed by Dipaola et al 8 had a sensitivity of 83%, specificity of 44%, PPV of 75%, and NPV of 57%. Iwasaki et al 12 concluded that these values were insufficient for clinical reliability; therefore, MRI alone was not reliable for identifying OCD lesion instability of the capitellum.
To our knowledge, the only MRI staging system specific for OCD lesions of the elbow that considers the ICRS classification is that reported by Itsubo et al 11 in 2014. Their classification system separated OCD lesions into 5 stages, yielding a very high accuracy (94%), sensitivity (100%), specificity (84%), PPV (92.5%), and NPV (85.7%) relative to the ICRS classification. On the other hand, Itsubo et al 11 reported that an accurate evaluation is sometimes difficult, as suspected synovial fluid flow in the subchondral bone may merely reflect bone marrow edema.
Our MRI-based staging system divided lesions into 4 stages per the ICRS classification. Because the ICRS classification is also a 4-stage classification, we believe that our MRI-based staging system corresponds better with the ICRS. In addition, we mainly focused on the outlines of the capitellum and the intensity changes of the articular cartilage for our MRI-based staging system, whereas the classification proposed by Itsubo et al 11 required additional information: signal intensity of the subchondral bone of the lesion, existence of a high signal interface line between the capitellar lesion and subchondral bone, contour of the capitellum in coronal and sagittal sections, and continuity of the cartilage surface. From this perspective, our MRI-based staging system is simpler and offers easy-to-identify stages. Although the diagnostic accuracy and specificity are slightly higher in the classification proposed by Itsubo et al 11 than in our MRI-based staging system, our system achieved equivalent specificity and higher PPV and NPV.
In the evaluation of OCD lesions, the ICRS classification remains the gold standard; therefore, it is sometimes unclear until surgery whether the OCD lesion is stable without relying on arthroscopic or direct visual assessment. 4,10 The MRI findings of the subchondral bone in cases of OCD at the elbow vary widely, with CT providing the standard for the evaluation of subchondral bone lesions. 18,21
Satake et al 18 reported that a sensitivity higher than 80% to detect an unstable OCD lesion was achieved for subchondral bone segmentation on CT (83%), but no MRI findings showed similar sensitivity. They reported specificities higher than 80% for articular irregularity (80%) and defect (80%), T2 high signal intensity interface (80%), and high signal intensity line through the articular cartilage (80%) on MRI as well as displaced fragment (100%) on CT. These findings suggest that subchondral bone information from MRI provides limited diagnostic accuracy. As the goal of our study was to create a simple and easy-to-identify staging system using MRI, and knowing that the condition of the articular cartilage is a key factor in determining the ICRS classification, we decided to focus solely on the capitellum’s shape rather than adhere to detailed subchondral bone information. Therefore, we made the difficult decision to minimize information on the subchondral bone in our staging system, based on previously reported literature stating that unstable OCD lesions show an irregular capitellum outline on MRI as the fragment is displaced or dislocated by articular fluid inflow. 8,10,11,14,15 Thus, our MRI-based staging system only uses the shape of the capitellum and the signal intensity of the articular cartilage for the grading of OCD lesions. The current validation study demonstrated a high rate of accuracy (88.9%) for our MRI-based staging system against the ICRS classification. The MRI-based system correctly identified the instability of OCD lesions with a sensitivity of 98.4%, specificity of 84.2%, PPV of 95.3%, and NPV of 94.1%.
We identified 9 cases for which our MRI-based staging system did not match the ICRS classification; the MRI-based system underdiagnosed (false negative) the lesion in 5 cases and overdiagnosed (false positive) the lesion in 4 cases. From a treatment perspective, determining if a lesion is ICRS class II or III is essential to inform the clinical decision regarding conservative versus surgical treatment, a clinical decision that is difficult to make. For cases with MRI-based stage 2 revised to ICRS class III, the capitellum was circular in shape, but the subchondral bone under the lesion was very thin and was considered to be unstable on palpation. For cases with MRI-based stage 3 revised to ICRS class II, the shape of the capitellum was irregular on MRI, but the lesion was deemed stable on intraoperative palpation. As the previous literature has suggested, it is very difficult to completely assess the condition of the subchondral bone via MRI alone, 12,18 and this limitation may have affected our false negative and false positive cases. Moreover, the difference in the diagnostic accuracy between the 1.5-T and 3-T MRI scanners might have been another reason for these findings. Although we did not obtain 100% accuracy, our MRI-based staging system correctly diagnosed ICRS class II and III lesions in 91.4% of cases (43/47 lesions). Therefore, we believe that this system is sufficiently accurate and effective for clinical application.
There are several limitations to our study that need to be acknowledged. Foremost, we retrospectively investigated MRI findings only. In actual practice, as mentioned previously, CT provides useful information on the condition of the subchondral bone, which helps in understanding the stability of an OCD lesion involving the capitellum and to determine the best surgical procedure. 18,21 Second, the MRI models used for imaging may differ depending on the time point along the course of OCD development. From August 2009 to March 2014, a 1.5-T MRI scanner (MAGNETOM Symphony) and a small coil (Loop Flex Coil) were used, and after April 2014, a 3-T MRI scanner (MAGNETOM Skyra) and a small coil (4-channel Special Purpose Coil) were used. The 3-T scanner has higher rendering accuracy and may have influenced the results, especially the false negative and false positive cases. Third, our staging system is only based on sagittal-plane MRI, which prevents a 3-dimensional evaluation of the OCD lesion, making it difficult to define whether the lesion is located medial, center, or lateral to the capitellum. We must rely on CT to evaluate the location of the lesion. Finally, because our MRI protocols were specifically designed to evaluate the capitellum’s outline and the articular cartilage’s condition, we cannot examine concomitant injuries, such as ulnar collateral ligament injuries or elbow instability. For those patients who needed an evaluation for these concomitant injuries, additional MRI was performed.
Conclusion
We provide evidence to support the integration of our MRI-based staging system of OCD lesions of the elbow into clinical practice as a preoperative tool to evaluate the stability of OCD lesions in an effort to inform the best treatment approach. The system corresponds well with the ICRS classification, with a diagnostic accuracy of 88.9%. We believe that our MRI-based staging system provides a useful preoperative clinical assessment for pediatric patients with OCD lesions of the elbow.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mito Clinical Education and Training Center, Tsukuba University Hospital, Tsukuba, Japan.