
Abstract
Background:
In the past few years, competition climbing has grown in popularity, and younger people are being drawn to the sport.
Purpose:
While radiographic changes in long-term climbers are known, there are little data available on adolescent climbers. The question arises as to whether climbing at high levels at a young age leads to radiographic changes and possibly an early onset of osteoarthritis of the finger joints.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 19 members of the German Junior National Team (GJNT group) and 18 recreational climbers (RC group) were examined clinically and radiographically in 1999. In 2011, these climbers were re-examined (mean follow-up, 11.3 ± 1.2 years). Radiographs were evaluated using a standard protocol, searching for physiological adaptations such as cortical thickness of the middle phalanx and an increased adopted Barnett-Nordin index, as well as for early-onset osteoarthritic changes of the hand. In contrast to the Kellgren-Lawrence scale, subchondral sclerosis was added to the group of physiological, adaptive stress reactions and was not defined as osteoarthritis. Osteoarthritis was defined by a Kellgren-Lawrence grade ≥2.
Results:
Overall, 15 of 19 (follow-up rate, 78.9%) climbers in the GJNT group and 13 of 18 in the RC group (follow-up rate, 72.2%), with a mean age of 26.8 years, were examined at the 11-year follow-up. Five climbers (33%) in the GJNT group presented with a decreased range of motion for the finger joints, in contrast to only 1 climber (8%) in the RC group. Radiographic stress reactions of the hand were found in 80% of the GJNT group and 46% of the RC group, including cortical hypertrophy (GJNT: 73%; RC: 23%), subchondral sclerosis (GJNT: 80%; RC: 31%), a broadened proximal interphalangeal joint base (GJNT: 67%; RC: 38%), and a broadened distal interphalangeal joint base (GJNT: 53%; RC: 31%). Training intensity in 1999 and body weight in 1999 were significant for the development of radiographic stress reactions in 2011 (P < .05 for both). Signs of early-stage osteoarthritis were seen in 6 climbers: 4 (27%) in the GJNT group and 2 (15%) in the RC group. Significant statistical influences for the development of early-onset osteoarthritis were found for overall total training years (P = .024), use of campus board training in 1999 (P = .033), and climbing level (P = .030).
Conclusion:
One-quarter of climbers who performed at a high level in their youth showed a “mild” form of osteoarthritis (Kellgren-Lawrence grade 2). In analyzing the training regimens of our climbers for longer than 10 years, we conclude that intensive finger training (eg, campus board training) can lead to early-onset osteoarthritis of the hand. We also demonstrate that a high Union Internationale des Associations d’Alpinisme (UIAA) climbing level correlates with the risk for early-onset osteoarthritis of the hand and therefore must be seen as a risk factor for developing early-onset osteoarthritis of the finger joints.
In the past decade, an elite group of young competition climbers has pushed the boundaries of sport climbing to new heights, having followed intense training regimens since their early teenage years. 22,29 As a higher rate of osteoarthritis in long-time climbers (>5 years) (Figure 1) has been reported, 1,5,11,24,25,39 –41 the long-term effects of this high impact and stress on the finger joints of these youngsters cannot be predicted. With the inclusion of sport climbing in the 2020 Olympics in Tokyo, a further increase in training intensity is to be expected. 22,34

Osteoarthritis of a 38-year-old climber with 22 years of experience with climbing.
Radiographic adaptations and changes in long-time adult climbers are well-known facts, and a positive correlation with their years of climbing has been shown. 1,5,11,24,25,39 –41 Very few data are available for young adolescent (<18 years) climbers. 24,28 Although nontraumatic epiphyseal fractures were first observed at the end of the 1990s, 6,13 they are more common nowadays. 4,12,22,28,39 In 2004, we reported on radiographic changes in the hands and fingers of the German Junior National Team (GJNT group), a group of recreational climbers (RC group), and a group of nonclimbers. 29 Although osteoarthritis was rare, radiographic adaptations were common in the young high-level climbers. The question arose as to whether these adaptations are precursors of osteoarthritis. 29 After analyzing our former adolescent climbers 40 for more than a decade, we aimed in this study to evaluate whether the documented radiographic adaptations lead to the early onset of osteoarthritis and whether radiographic adaptations are related to specific training regimens such as campus board training or training with additional weights.
Methods
This study was part of a long-term joint venture program of the German Alpine Club and the Technical University of Munich for the evaluation of child and adolescent climbing. 29 Several aspects, including social, cultural, economic, training method, gear and safety equipment development, and medical viewpoints, have been researched. 31 In 1999, 19 climbers in the GJNT group (mean age, 16.5 ± 1.9 years) and 18 in the RC group (mean age, 14.7 ± 2.3 years) were examined clinically and through radiographs. Between 2011 and 2013, we re-examined the climbers, resulting in a mean follow-up rate of 75.7% and a mean follow-up period of 11.3 ± 1.2 years. 40 All patients were examined clinically as well as by means of a radiographic examination of the hand in the anteroposterior (AP) view and of the fourth finger in the right hand in the lateral view. The fourth finger was used because some studies found this to be the most injured finger. 26,41,44 Before radiographs were taken, all participants/legal guardians gave written informed consent, and the Ethics Commission of RWTH Aachen University approved the study.
The clinical examination followed a typical examination protocol adopted from the standards of German peer assessments of statutory accident insurance. Active range of motion was measured using a goniometer manually attached to the finger joints. A decreased range of motion was determined if the following ranges could not be obtained actively—proximal interphalangeal (PIP) joint: extension/flexion 0°/0°/100°, and distal interphalangeal (DIP) joint: extension/flexion 0°/0°/60°—or if the climber could not actively extend all fingers to the horizontal level or flex them to touch the palm. Finger length was measured on the palmar side from the proximal flexor fold at the metacarpophalangeal level to the fingertip. Finger width was measured at the widest part of the PIP and DIP joints with a measuring caliper. 30 Radiographs were evaluated in a blinded fashion using a standard protocol and were grouped into physiological stress reactions and signs of early-stage osteoarthritis (Table 1 and Figures 2 and 3), analogous to the initial evaluation. 29,40 Radiographs in 1999 were all on film, and measurements were performed with a translucent scale using a magnifying glass; most (92%) of the re-evaluation radiographs could be analyzed digitally.


Cortical hypertrophy.
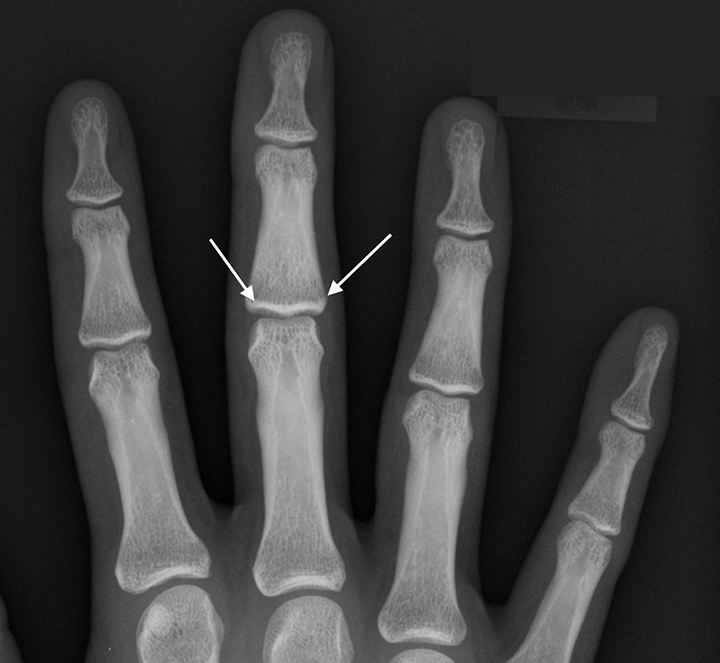
Subchondral sclerosis and broadened joint base.
In contrast to the Kellgren-Lawrence scale, 18 subchondral sclerosis was added to the group of physiological, adaptive stress reactions and was not defined as osteoarthritis. 29,40 Furthermore, osteoarthritis was defined if a Kellgren-Lawrence grade ≥2 was present. 1,25,29,40 Prior studies have shown that such reactions as cortical hypertrophy and subchondral sclerosis in the fingers could be adaptive signs of the high stress in climbing and could not be attributed to pathological osteoarthritic changes. 9,10,42 For a comparison with normal radiographic results, the visual guidelines given in the The Epidemiology of Chronic Rheumatism 17 were used. 1,25,29,40 For the evaluation of physiological adaptations to high stress, an adopted Barnett-Nordin index 3,29 (cortical thickness of the middle phalanx/total osseous thickness of the middle phalanx [cortical and cancellous bone] in the AP view) was used (normal range, 0.35-0.66). The original Barnett-Nordin index was defined for osteoporosis and measured on the metacarpals. 3 As there is no other specific score for osseous hypertrophy in the fingers, the Barnett-Nordin index has been used in several studies on radiographic osseous finger adaptations. 1,29,40 The results were compared between the GJNT and RC groups.
History was obtained using a standard questionnaire (64 questions on training history, sport-related medical history, nutrition, training methods). 31 The questionnaire also examined if campus board training (feetless climbing hand over hand on an overhanging board with various rungs) or training with extra weights was performed. Documented training hours were obtained from training books for the GJNT group and from trainers/high school teachers for the RC group, as these were part of a high school climbing program. For analyzing climbing levels, the hardest redpoint of the past year was transferred from the Union Internationale des Associations d’Alpinisme (UIAA) scale to the UIAA Medical Commission scale (eg, UIAA –9 = 8.7; UIAA 9 = 9.0; UIAA +9 = 9.3). 37 Presently, the UIAA climbing level ranges from 1 to 12, with grade 1 being the easiest and grade 12 the hardest. Redpoint criteria are defined as the completion of a climbing route without rest in a free manner; that is, rope, bolts, and quickdraws are purely used for protection and not as aid.
Statistical analysis was performed using Excel (Microsoft) for data collection and SPSS (IBM). Statistical analysis was performed through an independent statistician. All measured values are reported as mean ± SD. Normally distributed variable differences within and between groups were assessed with paired and unpaired t tests. All tests were 2-tailed, and a 5% probability level was considered significant. Cross-table analysis with the Pearson chi-square test was performed for group analysis. For correlation analysis for nonpaired variables, the Mann-Whitney rank-sum U test was used (2-tailed and a 5% probability level was considered significant).
Results
Fifteen of 19 climbers in the GJNT group and 13 of 18 climbers in the RC group were re-evaluated at a mean follow-up time of 11.3 ± 1.2 years. The dropout rate was 21% for the GJNT group and 28% for the RC group.
Biometrics and Physical Examination
The mean age of the climbers at follow-up was 27.3 ± 2.1 years in the GJNT group and 26.2 ± 2.3 years in the RC group. Within the 11-year follow-up period, body height and weight increased in both groups, and the body mass index (BMI) increased significantly from 1999 to 2011 for the GJNT group (P < .01) and the RC group (P < .01). In 2011, there were no significant differences in BMI between the groups. No significant changes could be found for the finger length and width of the PIP joint of the fourth finger of the right hand within the groups (Table 2).
Biometric Data a

a Values are reported as mean ± SD. GJNT, German Junior National Team; PIP, proximal interphalangeal; RC, recreational climbers.
In the clinical re-examination, 21% of the participants encountered contractures of the finger joints. Four of the 6 contractures were already evident in 1999. In 75% of all contractures, the PIP joint of the fifth finger had contracture; in 1 case, the PIP joint of the third finger was affected after an injury of the joint capsule; and in 1 case, the DIP joint of the third finger was affected (Table 3).
Clinical Signs of Osteoarthritis a
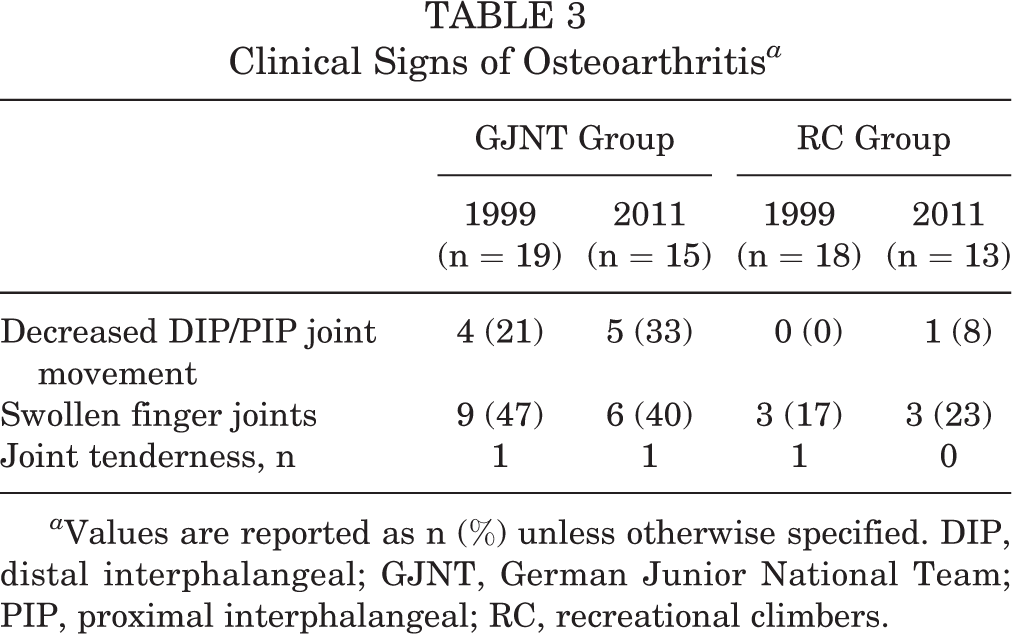
a Values are reported as n (%) unless otherwise specified. DIP, distal interphalangeal; GJNT, German Junior National Team; PIP, proximal interphalangeal; RC, recreational climbers.
During follow-up, 40% of the participants of the GJNT group and 23% of the RC group complained about swollen finger joints in the morning. In all cases except for 1, swelling was reported without any accompanied pain.
Sport-Specific Evaluation
In 1999, the mean climbing level was 8.9 ± 0.9 (UIAA scale) for the GJNT group and 6.7 ± 1.2 for the RC group. In 2011, the mean climbing level was 10.0 ± 1.1 for the GJNT group and 7.0 ± 1.5 for the RC group. The climbing level was significantly higher in the GJNT group than in the RC group in both 1999 and 2011 (P < .01 for both). At the time of follow-up, 79% of the participants (GJNT: 87%; RC: 69%) were still climbing regularly, with a mean of 14.9 ± 3.4 years of climbing in the GJNT group and 10.7 ± 4.7 years in the RC group. At the 2011 follow-up, the mean time spent climbing was 85 ± 49 days per year in the GJNT group and 16 ± 10 days per year in the RC group. At follow-up, participants in the GJNT group trained more frequently (P < .01) and had longer training sessions (P < .01).
Specific regimens such as campus board training was undertaken in 62% of the participants in the GJNT group, which represents a 20% increase in this group, whereas this sort of training saw a decrease of 8% in the RC group over the follow-up period, resulting in no campus board training at all in the RC group in 2011. Nevertheless, with a dropout rate of 6 athletes in the GJNT group, it may be possible that the athletes with campus board training are actually the same 8 as before and that this conclusion may be inaccurate. Pull-up training with extra weights was performed in 8% of the GJNT group, a decrease of 8% from 1999, while none of the participants in the RC group used this training technique. Table 4 lists specific training parameters for both groups.
Training Data a

a Values are reported as mean ± SD unless otherwise specified. GJNT, German Junior National Team; RC, recreational climbers.
b Detailed training data could not be gathered for all participants.
Radiography
Radiographic findings were grouped into physiological stress reactions and early-stage osteoarthritis signs. Stress reactions were found in 12 of 15 (80%) in the GJNT group and in 6 of 13 (46%) in the RC group in 2011. In 1999, 79% of the GJNT group and 28% of the RC group showed stress reactions. Table 5 shows the radiographic results for 1999 and 2011.
Radiographic Results a

a Values are reported as n (%) unless otherwise specified. GJNT, German Junior National Team; RC, recreational climbers.
By dividing the groups further into active climbers and nonactive climbers as of the date of follow-up, 14 of 27 (52%) active climbers showed radiographic stress reactions in 2011: 10 of 13 (77%) in the GJNT group and 4 of 8 (50%) in the RC group. Both epiphyseal fractures (1 in each group) from 1999 had healed completely and without later radiographic abnormalities (Figures 4 and 5).

Epiphyseal fracture in 1999.

The same patient as in Figure 4, 11 years later.
The parameter of active climbing or nonactive climbing did not show a statistically significant correlation (P = .104) for the outcome of stress reactions in 2011. A significant statistical correlation was seen between training intensity in 1999 (P = .032) as well as body weight in 1999 (P = .038) and the development of radiographic stress reactions in 2011 (Table 6).
Mann-Whitney Rank-Sum U Test Findings for Stress Reactions on Radiographs in 2011 a

a PIP, proximal interphalangeal; UIAA, Union Internationale des Associations d’Alpinisme.
The Barnett-Nordin index increased in the GJNT group from 0.50 ± 0.06 to 0.63 ± 0.11 in 2011 and in the RC group from 0.49 ± 0.07 to 0.61 ± 0.08 in 2011. There was no significant difference (P = .562) in the Barnett-Nordin index between the GJNT and RC groups. Table 5 shows the radiographic results.
Signs of an early stage of osteoarthritis were seen in 6 climbers: 4 (27%) in the GJNT group and 2 (15%) in the RC group. This shows an increase of 2 climbers per group over the follow-up period.
Statistically significant influences for the development of early-onset osteoarthritis were found for overall total training years (P = .024), use of campus board training in 1999 (P = .033), and climbing level (P = .030). Table 7 shows the detailed radiographic results, and Table 8 presents the Mann-Whitney U test findings.
Specific Radiographic Results a


Normal radiographic findings of a German Junior National Team member in 1999.

Normal radiographic findings of the same climber as in Figure 6 in 2011, still climbing at a national level.
Mann-Whitney Rank-Sum U Test Findings for Radiographic Signs of Osteoarthritis in 2011 a

a PIP, proximal interphalangeal.
Discussion
Radiographic adaptations and changes in long-time adult climbers are a well-known fact, and a positive correlation with their years of climbing has been shown. §§ Unfortunately, most of this research concerns adult long-term climbers (>5 years), while data on young climbers or the long-term effects of intensive climbing since childhood are still sparse. 35 Leal et al 20 were the first to report radiographic abnormalities in fingers and hands of sport climbers in 1987. They found subchondral sclerosis, cortical hypertrophy, and microfractures. Heuck et al 9 as well as Hochholzer et al 10 demonstrated radiographic adaptations to the high stress of climbing using radiographic and magnetic resonance imaging analyses. They found adaptive hypertrophy of the joint capsule in the PIP and DIP joints, thickening of the collateral ligaments, cortical hypertrophy, and hypertrophy of up to 50% of the flexor tendons themselves. They also showed that certain reactions, such as cortical hypertrophy, could be adaptive signs of high impact to the fingers in climbing and could not be attributed to pathological osteoarthritic changes. Similar findings of connective tissue adaptations were also reported by Schreiber et al. 42 Rohrbough et al 25 could not demonstrate a significantly higher rate of osteoarthritis among climbers than among nonclimbers.
These findings are contrary to those in a 2011 study by Allenspach et al. 1 They compared 31 male climbers with 67 nonclimbers and found a significantly higher risk of osteoarthritis in the climbers (P < .001). 1 While another study by Sylvester et al 43 could also not prove a higher risk of osteoarthritis in climbers’ hands, these authors found that climbers’ fingers have an increased diameter, with additional bone deposited subperiosteally. Significant predictors of such adaptations include the highest level achieved in bouldering and sport climbing. 43 Bollen and Wright 5 and Hochholzer and Schöffl 11,14,40 found that 28% to 39% of climbers with more than 15 years of climbing showed osteoarthritic findings on radiographs. In contradiction to these radiographic findings, the respective climbers were sometimes surprisingly free of complaints. 11 This result was confirmed by Allenspach et al, 1 who concluded that the “development of osteophytes seems to be ordinary in every climber.” Nevertheless, 15 years after the beginning of our research project and a mean of 11 climbing years later, this statement must be differentiated.
In our present study, 2 groups were monitored over a mean of 11 years, and detailed information on biometric data, training methods, and climbing parameters was collected. The follow-up rate was comparable in both groups (GJNT: 78.9%; RC: 72.2%). Both study groups were comparable for the parameters of body size and body weight at the beginning of the study as well as at follow-up. Regarding climbing load and performance, 79% of the participants still actively participated in the sport of climbing at follow-up: 69% in the RC group and 87% in the GJNT group. The participants of the GJNT group climbed significantly longer, more frequently, and at a higher climbing level. With regard to stress continuity, the comparison of the training data and climbing performances in 1999 and 2011 shows that the performances and associated stress in both groups remained largely constant. There was no significant difference between the groups in the Barnett-Nordin index in 1999 and at the time of follow-up. A comparison with the cohort of the original publication by Barnett and Nordin 3 showed that the Barnett-Nordin index of our climbing population was within the range of the age-specific standard group.
Finger contractures were found in 21% of our climber population, corresponding to 6 participants. This rate of contractures is well above epidemiological numbers of the population. Degreef and De Smet 7 reported a prevalence of finger contractures of 8% in the over-50-year-old Belgian population. Within this sample, a prevalence of 32% was shown for Dupuytren disease. The numbers in a comparable nonclimbing peer group were not available. In our study, we found 1 contracture of the fifth finger associated with Dupuytren disease. An increased prevalence of Dupuytren disease in climbers was observed by Schöffl and Schöffl 41 and Logan et al. 21 The latter authors found a prevalence of Dupuytren disease in their climbing cohort of up to 19.5%. Nevertheless, this study was conducted on adult climbers and classified all finger flexor contractures as Dupuytren disease; therefore, a comparison is not feasible. 21
Concerning the radiographic analysis, we were able to show a correlation between long-term radiographic adaptations and high-level young climbers, which may lead to an early onset of osteoarthritis. The re-evaluation showed an almost unchanged high proportion of radiographic stress reactions in 80% of the GJNT group after 11 years. In the RC group, these stress signs increased from 28% to 46% at follow-up. Years of climbing, participation in climbing competitions, training units and hours per week, and climbing level were significant denominators for the development of osseous stress reactions in youth climbers in our initial study. 40 At the follow-up in 2011, training intensity and body weight in 1999 were significantly correlated with the development of radiographic stress reactions.
Body composition (high BMI) has been reported as a possible risk factor for injuries in adult climbers, although this evidence is inconsistent. 2,8,15,35,36,38,45 Our study did not show a significant difference in BMI between both groups.
While 15 of 19 (79%) climbers in the GJNT group showed stress reactions on radiographs, early signs of osteoarthritis were seen in 27% of the GJNT group and 15% of the RC group. This corresponds to an increase of 22% in the GJNT group and 15% in the RC group over the follow-up period (P > .05). When signs of osteoarthritis were seen, the PIP joint (4/6 cases) was most frequently affected. These results are consistent with the most recently published study results on the subject. §§
It is remarkable that both cases of an epiphyseal fracture, 1 in each group, healed without consequences. Epiphyseal fractures have recently been reported more frequently 39 and are still a matter of intensive research for early detection, correlation with growth spurts, and best treatment options. 28,35 New results can be provided in our study for the correlation between training practices and climbing performance on the development of early finger arthritis. Our study was able to show a significant correlation between the development of osteoarthritic changes and the number of training years, climbing performance, and previous training (campus board training). For the prevalence of stress reactions, there was a significant correlation with previous training intensity in 1999 and body weight in 1999. Participants with a higher body weight thus showed proportionally more frequent radiological stress reactions of the hand.
Sylvester et al 43 compared osteological changes in rock climbers with nonclimbers and interestingly found a higher rate of osteoarthritis in the nonclimbers. Of course, these patients may have been nonclimbers because of the osteoarthritis. While this is in clear contradiction to the findings of many other studies,§§ the authors reported a significant correlation of climbing ability with bone strength, which our study showed as well. They also found a greater total bone width in the fingers of the climbers but not medullary width, which indicates that additional bone is deposited subperiosteally. 43 This finding is similar to our results, represented through a larger Barnett-Nordin index 3 in the GJNT group, although this finding did not reach statistical significance. In clinical adaptations of the hands (direct measurement of the finger width at the PIP joint), we found thicker measurements for the PIP joint in climbers versus nonclimbers but not at a statistically significant level, as shown by Schreiber et al 42 in adult climbers. We conclude that these adaptations are a result of a slow, long-term process and take many years to come to their end. Further research should analyze prophylactic matters to reduce the onset of osteoarthritic changes. The benefits of a proper “warm-up” and “cooldown,” no overuse of the crimping position, avoidance of early-age campus board training, no training with additional weights at a young age, and age/development-related training have been recommended but need further evaluation. 23,24,28,32,35 Also, epiphyseal stress fractures, their onset in correlation with growth spurts, and screening programs for early detection must be further understood. 28,35
Our study has several limitations and possible weaknesses that need to be accounted for. Overall, the number of participants is rather small. Nevertheless, this is based on the limited size of the national team per year. Several studies and authors have expressed limitations of the Kellgren-Lawrence scale itself, 16,19 which may have affected our results. There is no “gold standard” for the grading of osteoarthritis in the finger joints, 25 but the Kellgren-Lawrence system and its modified interpretation, as performed in the present and prior studies, 40 are widely used in climbing studies. 1,11,25,29,40 Another weakness may be the fact that we obtained AP radiographs of the hands and only the fourth finger in the lateral view. As Allenspach et al 1 reported that lateral radiographs have shown to be more accurate in finding, localizing, and rating osteophytes than AP radiographs, future studies should incorporate lateral views of all finger radiographs as well. Also, during the continuation of our study, digital radiographs became available, which have a higher resolution and accuracy in distance measurements. While all initial radiographs were on film and measurements were performed with a translucent scale using a magnifying glass, 92% of the re-evaluation radiographs could be analyzed digitally.
Conclusion
In analyzing the training regimen of our climbers for more than 11 years, we found a correlation between intensive finger training, such as campus board training, and the onset of osteoarthritic changes of the hand. We also demonstrated that a high UIAA climbing level correlates with the risk for early-onset osteoarthritic changes of the hand and therefore may be seen as a high risk factor for developing early-onset osteoarthritis of the finger joints.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported in part by the German Alpine Club, who financed the initial radiographic examinations in 1999 and 2011. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethics Commission of RWTH Aachen University (No. 332/16).