
Abstract
Background:
Ulnar collateral ligament (UCL) injury is a well-described etiology of pain and decreased performance for the overhead athlete. Despite a growing volume of literature regarding the treatment of these injuries for overhead athletes, there is a paucity of such data regarding stickhandling collision sport athletes, such as ice hockey players.
Purpose/Hypothesis:
The purpose of this study was to characterize this injury among 3 elite ice hockey players and to describe the ability of these athletes to return to play, as well as to review the unique sport-specific implications of this injury, evaluation, nonsurgical management, and considerations for return to play. The authors hypothesized that elite ice hockey players will be able to return to play at the same level following nonoperative treatment of UCL injury.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data from 3 elite professional ice hockey players who sustained a high-grade injury to the UCL were retrospectively reviewed. All athletes underwent 2 autologous conditioned plasma injections as part of their treatment and were evaluated with ultrasonography and magnetic resonance imaging.
Results:
Three consecutive elite ice hockey players were included in this study, and no patients were excluded. Players were cleared to full return to play at a mean 36 days postinjury. Follow-up examination at this time point demonstrated full range of motion of the elbow for all athletes, without tenderness to palpation over the UCL, including no tenderness over the humeral insertion site. Stability examination improved as well, demonstrating a soft to moderate endpoint with valgus stress, although this was not symmetric to the contralateral side. All athletes were able to continue to play at the same level of competition as before the injury occurred, without any complaints. No players had repeat injury during the same or following seasons.
Conclusion:
The authors present 3 elite-level ice hockey players who sustained a high-grade injury to the UCL. Successful return to play was possible after nonoperative treatment with injection of autologous conditioned plasma at a mean 36 days following injury. Athletes who injure either the top or bottom hand can return to play at the same elite level following this injury.
Keywords
Ulnar collateral ligament (UCL) injury is a well-described etiology of pain and decreased performance for the overhead athlete. The ligament runs from the medial epicondyle to the sublime tubercle and is composed of anterior oblique, posterior oblique, and transverse components, with the anterior oblique being the most significant stabilizer to valgus stress. The medial elbow experiences excessively high valgus torques and forces during many sports, such as baseball pitching, football throwing, golf, tennis, softball pitching, and javelin throwing; and the ability of the elbow to withstand these forces is critical to maintain performance. 23 Because the UCL acts as the primary stabilizer against valgus stress in the elbow, high stress is placed on it during the late cocking phase of throwing. As a result, UCL injury occurs most commonly among baseball pitchers. 1,7,12,18,32 However, given that UCL injuries occur with an excessive valgus stress across the elbow, there is a growing amount of data to suggest that this injury occurs in other athletes. Particularly susceptible to injury are athletes who experience a large degree of valgus force about the elbow, such as tennis players, wrestlers, 37 javelin throwers, 8,38 and football quarterbacks. 10
Although elbow injury is a relatively uncommon injury among ice hockey players, 33 with UCL injury reported to encompass as few as 2% of all their upper extremity injuries, 26 ice hockey players sustain significant valgus force at the elbow. While there is a paucity of literature evaluating the degree of valgus stress applied during slap shots and other ice hockey–specific forces, slap shots place a significant valgus stress at the elbow of the bottom stick hand, which is the arm that holds the stick closer to the ice and generates power for the shot. This results in a need to withstand tensile forces on the UCL and flexor-pronator mass 14 to maintain performance. Furthermore, UCL injury can occur with direct trauma during ice hockey. Thus, it follows that UCL injury is relevant to the ice hockey player.
Despite the fact that there is a growing volume of knowledge in the literature regarding the treatment of UCL injuries for overhead athletes, particularly baseball pitchers, there is a paucity of data regarding stickhandling and collision sport athletes, such as ice hockey players and lacrosse players.
We present a series of elite ice hockey players who sustained proximal UCL ruptures. The purpose of our study was to characterize this injury in a population of elite ice hockey players and to describe the ability of these athletes to return to play, as well as to review the unique sport-specific implications of this injury, evaluation, nonsurgical management, and considerations for return to play. We hypothesized that all elite ice hockey players will be able to return to play at the same level following nonoperative treatment of UCL injury.
Methods
After approval from our center’s institutional review board, we reviewed a series of 3 consecutive elite professional ice hockey players who sustained a high-grade injury to the UCL. Inclusion criteria for the study were professional ice hockey players who sustained a mid- to high-grade traumatic injury to the UCL. Exclusion criteria were patients with previous elbow injuries or those who elected to undergo immediate surgical treatment. Data were collected regarding each athlete’s age, mechanism of injury, physical examination, and radiographic examinations, as well as their treatment and return to play.
Treatment Algorithm
Each athlete was immediately removed from play and the elbow protected in a brace until further imaging could be obtained. Following diagnosis, a discussion was had with each athlete and his family regarding treatment options. We discussed various treatment options, including nonoperative treatment, surgical primary repair with and without internal bracing, and ligament reconstruction. Consideration was given to the magnitude of the injury, chances of healing, risk of reinjury, timing within the season, sport-specific dysfunction, and, most important, the player’s wishes. All patients elected to attempt a trial of nonoperative treatment with a course of orthobiologics, brace support, physical therapy, and progressive return to play.
Physical Therapy and Return to Play
Athletes underwent a course of progressive therapy following the injury, with the goal of maintaining range of motion, decreasing swelling, and strengthening the common flexor-pronator muscles, as this muscle group acts as a secondary stabilizer protecting against valgus laxity of the joint. Fourteen days after injury and as a result of significantly decreased tenderness over the injury zone, diminished pain overall, and restored range of motion, the athlete was allowed to stickhandle while skating. This was progressed to puck handling, light passing and receiving, and then cross-ice passing. Every 48 hours, if progression was pain free, then increased activity was added. At 3 weeks postinjury, the player was allowed to start wrist shots and then progress to incremental velocity slap shots. At 4 to 4.5 weeks following the injury, light contact was initiated. Patients were cleared to return to play in games with similar advancement criteria of pain-free activity in full-contact practice, with full range of motion. Throughout this process, the elbow was always protected in a hinged brace, and the athlete reported minimal symptoms. Athletes were evaluated over their remaining current and following seasons.
Autologous Conditioned Plasma
Autologous conditioned plasma (ACP; Arthrex), which is a leukocyte-reduced platelet-rich plasma (PRP), was injected into the injury site under direct visualization with ultrasonography at the UCL humeral insertion site, once 2 days following the injury and again 1 week later. There were no complications with the injection.
Statistics
Simple statistics, including means and SDs, were calculated for continuous variables.
Results
All 3 players with UCL injury were included in this study, with no patients excluded. Charts of all players were reviewed, and medical history revealed no previous injury to the injured elbows and good overall health. All 3 players sustained injury to the left elbow. However, 2 players were left-handed, and 1 player was right-handed; thus, injury was to the bottom hand for 2 athletes and the top hand for the other. Mechanism of injury in all 3 cases involved a valgus stress to the elbow (Table 1). Player A was behind the net, with his affected hand and arm holding the stick. When an opposing player initiated contact for a legal check, he sustained a valgus moment across the elbow, causing immediate onset of pain. He was taken out of the game with a complaint of medial-sided elbow pain. He described feeling a “pop” in the elbow when he sustained the contact. Player B fell onto an extended left arm and experienced a valgus stress as he hit the ice; he described a “popping” sensation as well. Player C was holding his stick with an extended arm when his left elbow sustained a forceful valgus stress when he was struck by an opponent.
Demographics and Mechanism of Injury

Initial physical examination revealed that each athlete’s elbow was anatomically aligned, with no evidence of gross deformity. Range of motion was decreased at the time of injury in each player (Table 2). Additionally, although pronation for each athlete was symmetric to the contralateral side, supination was limited by 15° versus the uninjured side in all injuries. Physical examination also revealed tenderness to palpation over the proximal/humeral attachment of the UCL and over the common flexor-pronator origin. Although the moving valgus stress test was positive for medial elbow pain between 60° and 120° of flexion in all cases, examination of elbow stability varied slightly among athletes. Player A had significant laxity to applied valgus stress at full extension and 30°, without a firm endpoint. Players B and C had 2+ laxity, but a soft endpoint was present. Each player was neurovascularly intact distally and had no signs of ulnar nerve injury.
Range of Motion of Each Athlete at Time of Injury, 2 Weeks After Injury, and Time of Return to Play a

a All athletes regained full range of motion of the elbow before return to play.
Radiographic Imaging
Radiographs taken at the time of the injury were negative for fracture. Initial sonographic examination revealed a longitudinal tear of the proximal anterior bundle of the UCL (Figure 1).

Coronal ultrasound of the left elbow of player A. “Prox” denotes the proximal aspect of the elbow, which is the medial distal humerus. The 4 arrows point to the complete rupture of the proximal ulnar collateral ligament. The white line shows gapping of the ulnohumeral joint. Dynamic valgus ultrasound at 30° of elbow flexion resulted in 2.3-mm gapping of ulnotrochlear distance (4.7 mm at rest, 7.0 mm with stress = 2.3-mm gap). The contralateral examination revealed a gapping distance of 1.2 mm.
Each athlete underwent magnetic resonance imaging (MRI) of the elbow at time of injury. Grades of UCL injury are noted in Table 3 (grade 1, a mild sprain with high signal around the ligament on T2; grade 2, severe sprain or partial tear with high signal around the ligament and partial disruption; grade 3, complete disruption of the ligament). UCL injuries ranged from grade 2 to 3, but each player had a grade 2 injury to the flexor mass. Figures 2A and 3 demonstrate the injury to one of the players (player A). There was an acute grade 3 tear of the proximal anterior bundle of the UCL (abUCL), acute grade 2 strain of the proximal myotendinous junction of the common flexor-pronator tendon, and static widening of the ulnotrochlear joint. There was no evidence of fracture, marrow contusion, or osteochondral injury.
MRI Grade of UCL Injury and Flexor Mass Injury of Each Athlete a
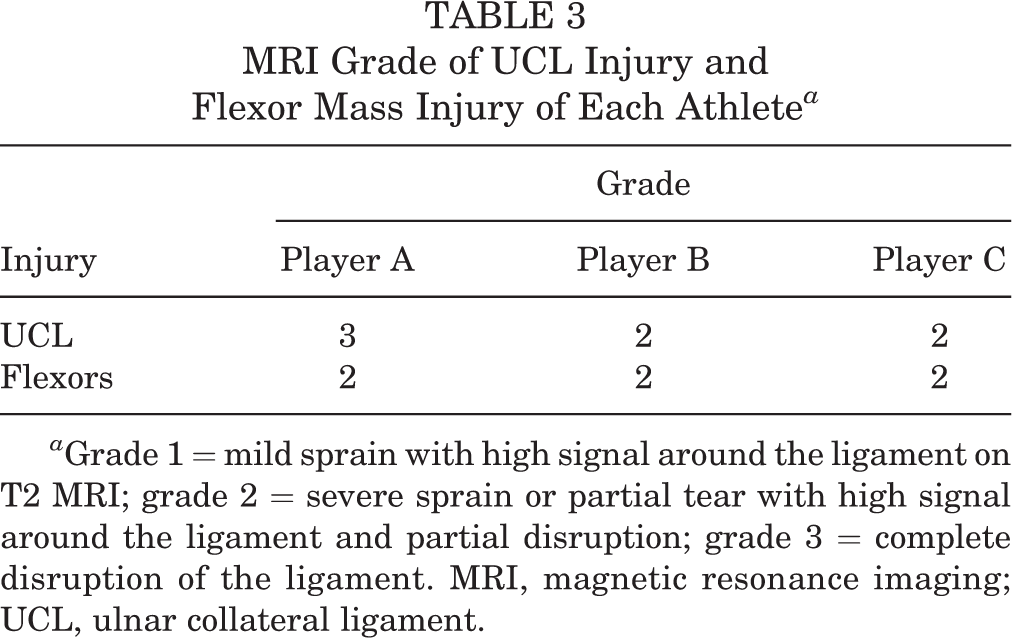
a Grade 1 = mild sprain with high signal around the ligament on T2 MRI; grade 2 = severe sprain or partial tear with high signal around the ligament and partial disruption; grade 3 = complete disruption of the ligament. MRI, magnetic resonance imaging; UCL, ulnar collateral ligament.

Sequential coronal T2-weighted images showing acute complete ulnar collateral ligament rupture in player A, with (A) surrounding edema. Magnetic resonance imaging (B) 4 weeks after injury and 3 weeks after second platelet-rich plasma injection and (C) 3 months after injury. Note the static widening on the ulnar side of the joint from the image (A) at the initial injury as compared (B, C) with subsequent scans with healing of the injury. Also note the interval decrease in soft tissue edema on the medial side of the elbow, consistent with healing of the flexor-pronator injury, as well as the formation of granulation tissue with interval healing of the ulnar collateral ligament.

Sequential axial T2-weighted images at the time of injury for player A. Note the absence of the ulnar collateral ligament at the attachment on the humeral origin, with reconstitution as the scan moves distally toward the insertion on the sublime tubercle, as well as significant soft tissue edema. Posterior fibers of the flexor-pronator mass are noted to be injured.
Clinical History and Return to Play
Each athlete was closely observed throughout his recovery, with progress in range of motion noted in Table 2. ACP was injected into the proximal insertion of the UCL at a mean 3 days postinjury, with a repeat injection at a mean 9 days postinjury, which is noted in Table 4.
Duration From Time of Injury to Return to Play and Until ACP Injections to the Injured Proximal UCL a

a ACP, autologous conditioned plasma; UCL, ulnar collateral ligament.
At 4 weeks postinjury, physical examination revealed resolution of the elbow effusion, bilaterally symmetric range of motion, and minimal tenderness over the proximal origin of the UCL. Joint laxity examination improved for all athletes, and moving valgus stress demonstrated significantly diminished pain between 70° and 120°. Flexor-pronator strength was nearly symmetric. Repeat MRI of the elbow showed a persistent fluid cleft between the UCL and its humeral attachment but with some evidence of bridging scar tissue (representative athlete noted in Figure 2B). There was also resolution of the static widening of the ulnotrochlear joint. Likewise, decreased edema within the common flexor-pronator suggested progressive partial healing of the injury. Repeat sonographic dynamic valgus confirmed the finding as well as decreased stress widening of the joint space.
Players were cleared to full return to play at a mean 36 days postinjury (Table 4). Follow-up examination at that time demonstrated full range of motion of the elbow for all athletes, without tenderness to palpation over the UCL, including no tenderness over the humeral insertion site. Stability examination improved as well, demonstrating a soft to moderate endpoint with valgus stress, although this was not symmetric to the contralateral side. All athletes were able to continue to play at the same level of competition as before the injury occurred, without any complaints. Repeat MRI of the elbow revealed a healing UCL (representative athlete noted around time of return to play in Figure 2B and at 3 months in Figure 2C). No repeat injuries occurred during the remainder of the current season or the following season.
Discussion
We found that in 3 mid- to high-grade UCL injuries, elite ice hockey players were able to return to play at a mean 36 days after the time of injury when treated nonoperatively with a series of ACP injections. Additionally, these athletes were able to return to the same level of play, regardless whether their top stick hand or bottom stick hand was affected. However, neither the stability on physical examination nor the radiographic imaging of the UCL improved to the preinjury level.
All 3 elite ice hockey players in our study sustained UCL injury via a significant trauma causing valgus stress at the elbow, which is one way that treatment of this injury differs among stickhandling and contact athletes and overhead athletes. Baseball pitchers generally experience an acute rupture of the UCL following chronic repetitive microtrauma, leading to changes in the mechanical properties of the ligament over time. 3 Even though 2 players injured the UCL of their bottom stick hand, which experiences valgus stress during slap shots, imaging in our study did not show chronic changes to the UCL at the time of injury. This difference is pertinent to the treatment choice. Since chronic degenerated ligaments generally require reconstruction, UCL injuries among baseball pitchers are most commonly treated with reconstruction, 4,5,19,37 and only a minority of pitchers can return to the same level of competition without surgery. 31 However, ice hockey players, even those at an elite level, may require different considerations. Athletes who have an acute tear to an otherwise normal ligament may respond to other therapeutic modalities, as the traumatically injured structure has the potential to heal.
As the protocol for treatment of these acute injuries among elite hockey players was PRP, all 3 hockey players in our study received 2 injections of ACP. PRP was described as a potential therapy for partial UCL rupture among baseball pitchers, and it has demonstrated good results in the literature. 9,11,17,29 PRP contains increased concentrations of growth factors—such as platelet-derived growth factor, epidermal growth factor, insulin-like growth factor, transforming growth factor β-I, vascular endothelial growth factor, hepatocyte growth factor, and basic fibroblast growth factor—that help modulate the healing of tissue through enhancement of anabolism, cell proliferation, angiogenesis, inflammation control, cell differentiation, and coagulation. 25,28 Podesta et al 29 treated 34 pitchers with partial-thickness UCL tears with PRP under ultrasound guidance. Patients were placed in a physical therapy program and allowed to return to play only when symptoms had completely resolved: 88% of the athletes returned to play at the same level of play at a mean 12 weeks following the injection, while only 1 patient required UCL reconstruction. Dines et al 9 evaluated a series of 44 baseball players treated with between 1 and 3 PRP injections for partial UCL ruptures. With regard to the professional pitchers, 67% returned to the same level of play at a mean 12 weeks postinjury. These authors do, however, recommend surgery for complete UCL rupture. Furthermore, these studies were not powered to evaluate the clinical utility of PRP for these injuries, and there is even evidence that PRP may hinder healing of injured tissues. 21 While our study was not designed to evaluate the utility of PRP in complete injury, the ability of elite athletes to expeditiously return to play following UCL injury, in some cases complete rupture, suggests that investigation may be helpful to determine the utility of PRP in a population of nonthrowing athletes with significant injury to the UCL.
Every athlete in our study had injury to the flexor-pronator mass and medial elbow soft tissues, with a partial injury to the flexor-pronator mass (grade 2). Additionally, we observed healing of this injury on MRI before athletes returned to play. The flexor-pronator mass provides dynamic stabilization to valgus torque across the elbow, which can help an athlete stabilize the elbow despite UCL injury. 13,36 Following return to play without symptoms among hockey players with UCL injury treated nonoperatively, it is important to consider the consequence of chronic fatigue of the dynamic stabilizers to valgus that can occur over the course of a game or season. Fatigue may lead to a decreasing ability of the flexor-pronator mass to compensate for an absent UCL and thus to symptoms of pain and instability. These symptoms should be monitored and considered before players are advanced through rehabilitation and return to play. Furthermore, since elbow bracing has been demonstrated to decrease medial elbow joint gapping, 16 this should be considered in the rehabilitation protocol to facilitate healing of the UCL and flexor-pronator structures as well as to protect these injuries from trauma or fatigue. Hockey players, including the 3 elite players in our study, are amenable to competitive play in a hinged brace in the early phase of return to play, which may play a role in the expedient return to play (36 days on average) as well as an absence of reinjury.
It is also important to note that none of the players in our study experienced injury to the ulnar nerve. This structure plays a critical role in the function of the upper extremity of athletes, and injury is a predictor of poor outcome of nonsurgical treatment. 24,30 The absence of injury to this structure may help explain the reliable and similar return-to-play times among athletes in our study.
Considerations for Evaluation of UCL Injuries in Ice Hockey Players
Initial evaluation of this injury should begin with a complete history and physical examination, including evaluation of stability of the elbow at 0° and 30°. Care should be taken to discern the location of maximal pain along the UCL, specifically at the humeral or ulnar insertion or the midsubstance of the ligament. Given the high stresses that can occur along the medial side of the elbow, examiners should be cognizant of possible injury to the ulnar nerve at the elbow but also at the cervical spine and brachial plexus. 15
Imaging should begin with plain radiographs to evaluate for bony ligament avulsion injuries, valgus alignment, UCL calcification, and posteromedial osteophytes, as well as to assess for other possible pathology about the elbow. Stress radiography or fluoroscopy can be used to assess for laxity about the elbow. Stress radiography of the dominant elbow of baseball players with UCL injuries has shown a 0.4 mm–greater opening as compared with the nondominant arm. 3 Larger mean openings (0.6 mm) can be expected with full-thickness UCL tears versus partial-thickness tears (0.1 mm). 3 Additionally, stress ultrasonography of the UCL can add valuable information in diagnosing partial and complete UCL injury. 2,6 Ciccotti et al 6 demonstrated increased valgus joint gapping of 2.0 mm, 1.4 mm, and 3.4 mm with valgus stress via release of the anterior band, posterior band, and entire abUCL, respectively, as compared with the contralateral extremity.
Ultimately, MRI should be obtained as the gold standard for diagnosis of this injury, and it can provide additional data regarding the severity of the injury, including the presence of intraligamentous calcifications, T-sign presence, and localization of the injury. 20 The abUCL is visualized along its long axis on coronal images and in cross section on oblique axial images, when the elbow is imaged in extension. On coronal proton density– and T2-weighted images, the intact abUCL is seen as a continuous structure originating from the caudal aspect of the humeral epicondyle and inserting upon the medial aspect of the coronoid process, the sublime tubercle. Along the majority of its length, the abUCL demonstrates low signal on proton density– and T2-weighted images. The deep and proximal-most fibers of the UCL may interdigitate with fat and appear striated and mildly heterogeneous on T1-, proton density–, and T2-weighted images, in the absence of injury. The distal UCL inserts along the medial aspect of the sublime tubercle, within 3 to 4 mm of the proximal articular margin of the sublime tubercle. 22,27 The transverse band may be seen on axial images contributing to the floor of the cubital tunnel. The transverse and posterior components of the UCL are less consistently visualized in their entirety but are clinically and functionally less significant. In the setting of injury, abnormally increased signal is seen within and around the UCL on T1- and T2-weighted images because of edema and hemorrhage and/or granulation tissue. Abnormalities of morphology may be present, including disorganization of fibers, laxity, or discontinuity.
Since UCL pathology often develops insidiously as sequela of repetitive microtrauma for the throwing athlete, magnetic resonance arthrography may be preferred. Although it involves a minimally invasive procedure, magnetic resonance arthrography offers the benefit of joint capsular distension, and it has been shown to increase conspicuity of partial-thickness articular-sided tears, particularly in the subacute or chronic setting. 34,35 However, in the setting of an acute traumatic valgus injury to the elbow, as in hockey players, there is often autodistension of the joint capsule by traumatic effusion, obviating this benefit of arthrography. Similar to ligamentous injury elsewhere, in the acute setting, intra- and periligamentous edema and hemorrhage result in foci of signal hyperintensity on T2-weighted and proton density imaging, increasing soft tissue contrast and lesion conspicuity, despite the lack of intra-articular contrast.
Limitations
We were able to describe the history of UCL injury and nonoperative treatment in a population of elite athletes who can have a high demand for valgus stability, as in the instance of slap shots, which is poorly described to date in the literature. This study is not, however, without limitations. As we had a small sample size, further study is needed to validate our results. Additionally, we had no control group, so we were unable to attribute any benefit that the ACP injection may provide with regard to recovery in this particular injury. However, given that we are describing the course of injury of elite athletes, it is difficult to validate this question with a control group; hence, further study is required to elucidate the influence that ACP plays in this pathology.
Conclusion
We present 3 elite-level ice hockey players who sustained a high-grade injury to the UCL. We demonstrate a successful return to play after nonoperative treatment with injection of ACP at a mean 36 days following injury. We found that ice hockey players who injure either their top or bottom hand can return to play at the same elite level following this injury.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: C.L.M. has received educational support from Arthrex and Smith & Nephew.
Ethical approval for this study was obtained from the University of Pittsburgh Institutional Review Board.