
Abstract
Background:
Remnant-preserving anterior cruciate ligament (ACL) reconstruction was introduced to improve clinical outcomes and biological healing. However, the influences of remnant preservation on tibial tunnel position and enlargement are still uncertain.
Purpose:
To evaluate whether remnant-preserving ACL reconstruction influences tibial tunnel position or enlargement and to examine the relationship between tunnel enlargement and graft-to-bone integration in the tibial tunnel.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 91 knees with double-bundle ACL reconstructions were enrolled in this study. ACL reconstruction was performed without a remnant (<25% of the intra-articular portion of the graft) in 44 knees (nonremnant [NR] group) and with remnant preservation in the remaining 47 knees (remnant-preserving [RP] group). Tibial tunnel position and enlargement were assessed using computed tomography (CT). Comparisons between groups were performed. Furthermore, graft-to-bone integration in the tibial tunnel was evaluated using magnetic resonance imaging, and the relationship between tunnel enlargement and graft-to-bone integration at 1 year after ACL reconstruction was assessed.
Results:
A total of 48 knees (25 in NR group, 23 in RP group) were included; 19 and 24 knees in the NR and RP groups were excluded, respectively, because of graft reruptures and a lack of CT scans. There were no significant between-group differences in tibial tunnel position (P > .05). The degree of posterolateral tunnel enlargement in the axial plane was significantly higher in the RP group than that in the NR group (P = .007) 1 year after ACL reconstruction. The degree of anteromedial tunnel enlargement on axial CT was significantly smaller in knees with graft-to-bone integration than in those without integration (P = .002) 1 year after ACL reconstruction.
Conclusion:
ACL reconstruction with remnant preservation did not influence tibial tunnel position and did not decrease the degree or incidence of tibial tunnel enlargement. At 1 year postoperatively, tunnel enlargement did not affect graft-to-bone integration in the posterolateral tunnel, but graft-to-bone integration was delayed in the anteromedial tunnel.
Keywords
The importance of anatomic graft placement for successful anterior cruciate ligament (ACL) reconstruction is gaining consensus. Currently, ACL reconstruction typically uses a bone–patellar tendon–bone graft or a multistrand soft tissue graft consisting of the medial hamstring tendon, with successful outcomes at 2 years after surgery, which are comparable for both types of graft, provided that reconstruction was conducted anatomically. 25
Nevertheless, tibial tunnel enlargement remains a challenge, often complicating revision ACL reconstruction. 11,37 It has been reported that tunnel enlargement is more pronounced for hamstring grafts than for bone–patellar tendon–bone grafts. 1,7,36 Tunnel enlargement is considered to occur under the influence of biological factors, which include tunnel infiltration of synovial fluid containing osteolytic cytokines, 8 and mechanical factors, which include micromotion at the tunnel aperture (“windshield wiper” and “bungee” effects), nonanatomic tunnel placement, and aggressive rehabilitation. 16 It remains controversial whether tunnel enlargement after ACL reconstruction affects clinical outcomes 5,11,17 or graft-to-bone integration in the tibial tunnel.
Remnant-preserving (RP) ACL reconstruction has multiple theoretical advantages such as (1) the acceleration of revascularization, (2) the preservation of proprioceptive neural elements, and (3) a lower incidence of tibial bone-tunnel enlargement. 2,4,10,31 Positioning the remnant so that it closes the tibial tunnel aperture can prevent synovial fluid leakage. 39 Furthermore, micromotion at the tunnel aperture will disappear once complete graft-to-bone integration is achieved. 14 The earlier the graft is incorporated into the knee joint, the less pronounced tunnel enlargement will be. 14,39 However, few studies have investigated the relationship between remnant preservation and tibial tunnel enlargement. 9,39 Furthermore, RP ACL reconstruction may result in a different tibial tunnel position compared with that obtained using conventional ACL reconstruction, which may affect tunnel enlargement considerably.
The aims of the present study were as follows: (1) to evaluate whether remnant preservation influences tibial tunnel position or (2) enlargement and (3) to examine the relation between tibial tunnel enlargement and graft-to-bone integration in the tibial tunnel. We hypothesized that (1) RP ACL reconstruction does not influence tibial tunnel position, (2) RP ACL reconstruction decreases the degree and incidence of tibial tunnel enlargement, and (3) tibial tunnel enlargement has a negative effect on graft-to-bone integration after ACL reconstruction.
Methods
Patients
Between April 2012 and March 2014, 115 consecutive double-bundle ACL reconstructions using semitendinosus grafts were performed at our institution. The inclusion criteria were primary ACL reconstruction, unilateral ACL reconstruction, use of semitendinosus grafts with adequate length (>24 cm before halving) and diameter (>5 mm when doubled), minimum follow-up of 1 year, computed tomography (CT) at 1 week and 1 year postoperatively, and magnetic resonance imaging (MRI) at 1 year postoperatively. The exclusion criteria were revision surgery, multiligament injuries, osteoarthritis, chondral lesions requiring treatment, and previous knee surgery. Twenty-four knees were excluded (revision surgery, 18 knees; osteoarthritis, 3 knees; multiligament injury, 2 knees; and requiring chondral treatment, 1 knee). This left 91 knees for the present study. All patients provided signed informed consent forms to participate in the study, and the study protocol was approved by our institutional review board.
Patient Assignment
Patients were divided into 2 groups based on the arthroscopic appearance of the ACL remnant after graft transplantation. 23 Knees in which the length of the remnant was <25% of the intra-articular portion of the anteromedial (AM) graft were assigned to the nonremnant group (NR group), while knees in which the remnant was larger (≥25% of the intra-articular portion of the AM graft) were assigned to the RP group (Figure 1). Arthroscopic assessment of the remnant size and subsequent patient assignment were performed by 1 of 3 surgeons (E.T., Y.Y., and Y.I.) intraoperatively.

Arthroscopic views of anatomic double-bundle anterior cruciate ligament reconstruction. (A) Representative knee managed via reconstruction without preservation of the ligament remnant (<25% of the intra-articular portion of the graft). (B) Representative knee managed via reconstruction with preservation of the ligament remnant (≥25% of the intra-articular portion of the graft).
Surgical Technique
After anesthesia was induced, the knee was evaluated, and a longitudinal skin incision of about 3 cm was made on the upper pes anserinus. Only the semitendinosus tendon was harvested. The harvested semitendinosus tendon was halved and folded, and the distal half was used for AM bundle reconstruction, while the proximal half was used to create the posterolateral (PL) bundle. An EndoButton CL device (Smith & Nephew) was used for femoral graft fixation, and a Mini-Suture Disc (B. Braun Aesculap) was used on the tibial attachment site. Before graft passage, the grafts were pretensioned using a Graftmaster System with Suture Vise and Tensiometer (Smith & Nephew). In parallel with graft preparation, the ruptured ACL was inspected arthroscopically, and any meniscal injury observed was managed according to the injury status. Remnant tissue of the ruptured ACL on the tibial surface was left as it was, while remnant tissue on the femoral side was removed so that the ACL femoral footprint, the resident’s ridge, and the posterior cartilage margin of the lateral femoral condyle could be identified.
Using a transportal technique, the femoral tunnels of the AM and PL bundles were created just behind the resident’s ridge. 24,28 The tibial tunnel of the AM bundle was made posterior to the Parsons knob and just lateral to the medial intercondylar eminence. 32 The tibial tunnel of the PL bundle was made between the medial intercondylar eminence and the point of insertion of the anterior horn of the lateral meniscus. After 2 femoral and 2 tibial tunnels were created, the grafts were introduced from the tibial tunnel to the femoral tunnel through any remnant tissue. Finally, both the PL bundle and the AM bundle were fixed simultaneously at 15° of knee flexion.
After surgery, all patients underwent postoperative management according to the same rehabilitation protocol, which included 1-week splint immobilization of the extended knee, followed by the initiation of passive and active range of motion exercises. Full weightbearing was allowed immediately after surgery, while jogging was allowed at 3 months postoperatively. Return to strenuous activity was allowed at 6 to 8 months postoperatively.
Radiographic and CT Evaluations
After ACL reconstruction, the tibial tunnels were evaluated on radiography by a single orthopaedic surgeon (Y.K.) blinded to surgical and postoperative clinical data. Anteroposterior and lateral digital radiographs (FCR; Fujifilm) of the ACL-reconstructed knees were obtained postoperatively. On coronal and sagittal views, the divergence angle of the tibial tunnel from the long axis of the tibia was measured using a DICOM viewer (Figure 2). The long axis of the tibia was defined as the long axis of the diaphysis of the tibia, which could be measured on each radiograph.
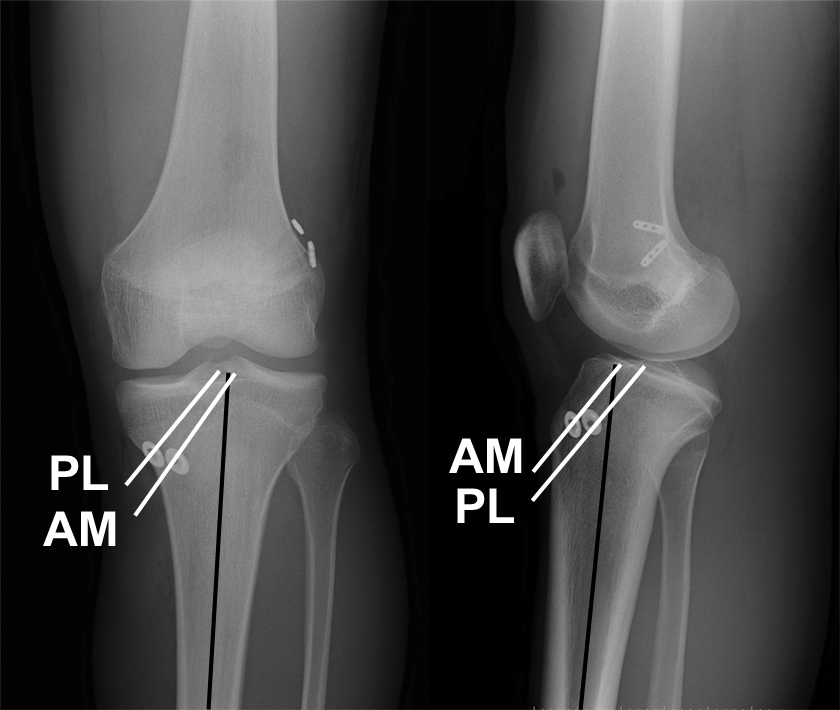
Evaluation of the divergence angle. The angle was defined as the angle between each tunnel axis (white lines) and the long axis of the tibia (black lines) on each radiograph. AM, anteromedial; PL, posterolateral.
To evaluate the position and potential enlargement of the tibial tunnels, CT was performed at 1 week and 1 year after surgery using a 64-detector CT scanner (Discovery CT750 HD; GE Healthcare) and the same scanning protocol (section thickness, 0.625 mm; beam pitch, 1.0; section spacing, 0.625 mm). Three-dimensional reconstruction of 2-dimensional images was performed in the operator console. The tibial tunnel position was evaluated on images of the surface of the tibial plateau. The quadrant method described by Tsuda et al 34 was applied for evaluating the tibial tunnel position using specialized software (Canvas X; ACD Systems) (Figure 3). The anteroposterior length of the tibial plateau (AP) and the distance from the anterior edge of the tibial plateau to the center of the tibial tunnel (APt) were measured perpendicularly to the posterior reference line. The mediolateral width of the tibial plateau (ML) and the distance from the medial edge of the tibial plateau to the center of the tibial tunnel (MLt) were measured parallel to the posterior reference line. Finally, the tibial tunnel position was defined in terms of the percentage ratios APt/AP and MLt/ML.

Schematic representation of the quadrant method used to evaluate the tibial tunnel position. The center of the tibial tunnel is defined in terms of the percentage ratios MLt/ML and APt/AP. MLt/ML is calculated as the distance from the most medial contour (MLt) relative to the mediolateral width of the tibial plateau (ML). APt/AP is calculated as the distance from the most anterior contour (APt) relative to the anteroposterior length of the tibial plateau (AP).
Tunnel enlargement was determined based on CT in standard sagittal and axial views. Sagittal reconstruction was performed parallel to the lateral aspect of the lateral femoral condyle. Tunnel enlargement was assessed by measuring the sagittal and axial widths of the tibial bone tunnel at 10 mm from the intra-articular outlet of the tunnel, perpendicular to the long axis of the tunnel, as described in previous studies (Figure 4). 18,29 All measurements were taken from the sclerotic bony margins. The degree of tunnel enlargement was defined as the percentage change in tunnel diameter between the scans performed at 1 week and 1 year after surgery. The incidence of tunnel enlargement was defined as the number of tibial tunnels noted to have enlarged by >20%. 18

Measurement of the tibial tunnel width (white arrows) on computed tomography. The tunnel width was measured at 10 mm from the intra-articular outlet of the tibial tunnels, perpendicular to the long axis of the tunnels. (A) Sagittal view and (B) axial view.
MRI Evaluation
Graft-to-bone integration in the tibial tunnel was evaluated on MRI performed at 1 year after surgery using a 1.5-T MRI unit (GE Healthcare). The knee was placed in a relaxed extended position in an extremity coil. Graft-to-bone integration was assessed on fast spin-echo proton density–weighted images from axial MRI sections, which were evaluated by an orthopaedic surgeon blinded to tunnel enlargement status (Y.K.). The evaluation of graft-to-bone integration in the tibial tunnel was based on a protocol described previously. 12 The presence or absence of synovial fluid at the tunnel-graft interface was assessed (Figure 5). If an area of higher signal intensity was observed between the graft and bone tunnel, the knee was classified as positive for the presence of synovial fluid at the tunnel-graft interface. Knees with no findings were classified as negative for synovial fluid at the tunnel-graft interface. The kappa coefficient for intraobserver and interobserver reliabilities in the assessment of graft-to-bone integration has been reported previously. 23 We assessed the relationship between the degree of tunnel enlargement and graft-to-bone integration.

Magnetic resonance imaging of graft-to-bone integration in the tibial tunnel. The evaluation was based on the (A) presence or (B) absence of synovial fluid (high signal intensity) at the graft-tunnel interface.
Statistical Analysis
Statistical analysis was performed using SPSS version 22.0 (IBM). A t test was used for between-group comparisons of age, graft diameter, tunnel position, divergence angle, and degree of tunnel enlargement, and the chi-square test was used for other demographic data and the incidence of tunnel enlargement. A t test was also used to compare the degree of tunnel enlargement between the positive bone-to-graft integration group and negative integration group at 1 year after surgery. Pearson correlation coefficients were used to assess the association between patient age and degree of tunnel enlargement and to assess the association of tunnel enlargement between the AM tunnel and PL tunnel. A previous power analysis indicated that a sample size of at least 26 patients per group was necessary to detect an intergroup difference in each parameter with an alpha of .05 and a power of 80%. For all analyses, statistical significance was set at P < .05. All data were reported as the mean ± SD.
Results
Patient Assignment Based on Remnant Preservation
Of the 44 and 47 knees assigned to the NR and RP groups, respectively, 19 knees in the NR group and 24 knees in the RP group were further excluded from the analysis. Specifically, a graft rerupture occurred in 3 (1 occurred at 4 months and 2 occurred between 6 and 12 months after surgery) and 4 (1 occurred at 4 months and 3 occurred between 6 and 12 months after surgery) patients of the NR and RP groups, respectively (graft failure rate: 6.8% and 8.5%, respectively; P = .537), while a lack of CT scans was noted regarding 16 and 20 knees in the NR and RP groups, respectively. Ultimately, 48 knees (25 in the NR group, 23 in the RP group) were included in the present analysis (Figure 6). With the exception of mean patient age at the time of ACL reconstruction, there were no significant differences in demographic characteristics between the 2 groups (Table 1). The degree of AM tunnel enlargement in the sagittal plane was positively correlated with patient age (r = 0.35, P = .040). There was no statistical correlation between age and other parameters.
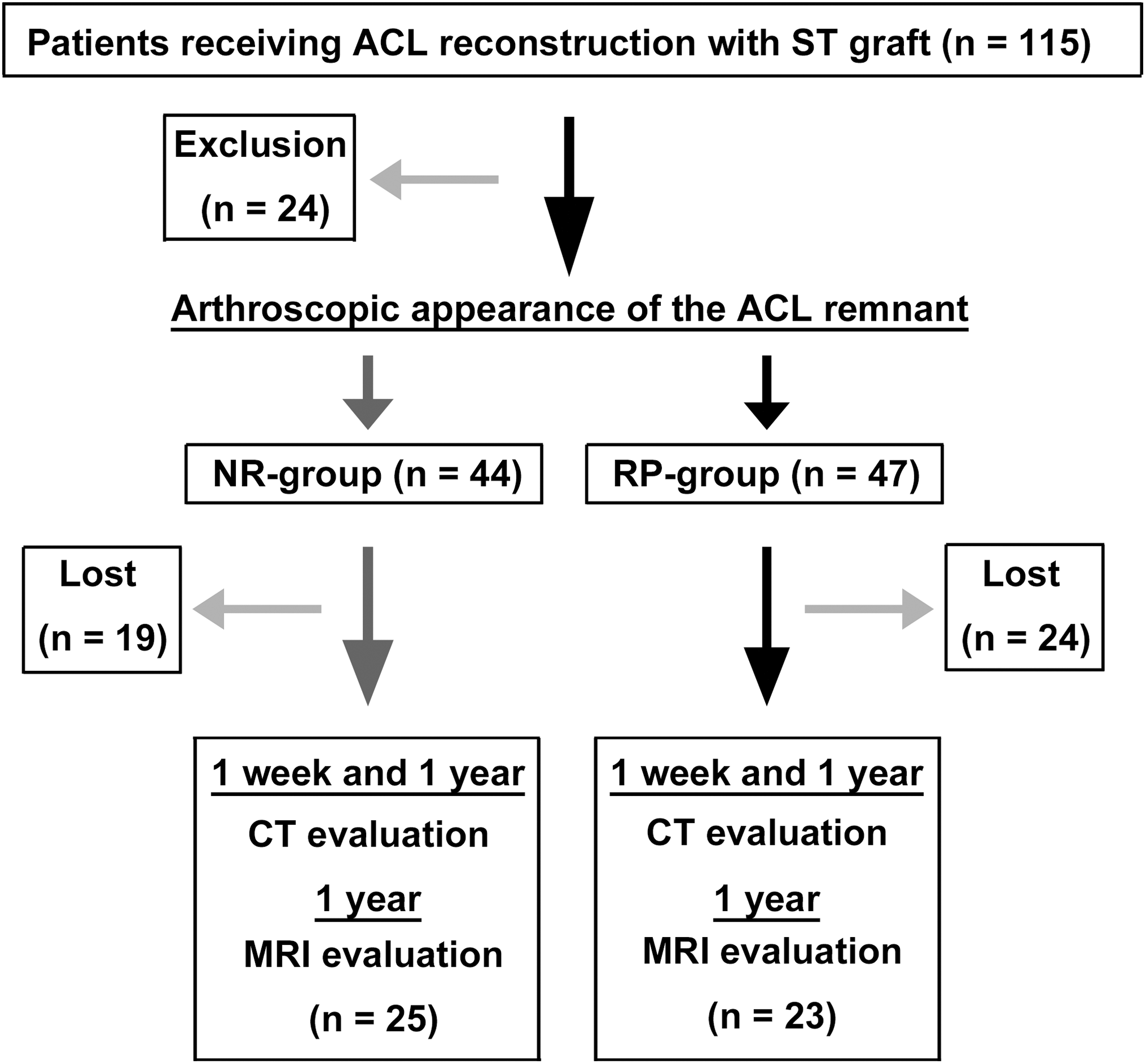
Study design. Patients were stratified into 2 groups according to the arthroscopic appearance of the anterior cruciate ligament (ACL) remnant after graft transplantation. CT, computed tomography; MRI, magnetic resonance imaging; NR, nonremnant; RP, remnant-preserving; ST, semitendinosus.
Patient Demographic Data a

a Data are reported as mean ± SD unless otherwise specified. AM, anteromedial; NR, nonremnant; PL, posterolateral; RP, remnant-preserving.
Radiographic and CT Evaluations of the Divergence Angle and Tunnel Position
Table 2 shows the mean angle between the tibial tunnel and the tibial long axis on coronal and sagittal radiographs for each bundle and each group. There were no significant between-group differences concerning divergence angle on radiography.
Divergence Angle of the AM and PL Tunnels a

a Data are reported as mean ± SD in degrees. AM, anteromedial; NR, nonremnant; PL, posterolateral; RP, remnant-preserving.
On 3-dimensional CT of the tunnel position in the NR group, the mean MLt/ML and APt/AP of the AM bundle were 47.2% ± 2.7% and 37.4% ± 5.7%, respectively, while those of the PL bundle were 48.0% ± 2.6% and 50.6% ± 7.4%, respectively (Table 3). In the RP group, the mean MLt/ML and APt/AP of the AM bundle were 48.2% ± 2.0% and 36.8% ± 5.4%, respectively, while those of the PL bundle were 48.0% ± 2.7% and 50.2% ± 5.9%, respectively. There were no significant between-group differences concerning tunnel position on CT.
Position of the Tibial Tunnel a

a Data are reported as mean ± SD in percentages. MLt/ML is calculated as the distance from the most medial contour (MLt) relative to the mediolateral width of the tibial plateau (ML). APt/AP is calculated as the distance from the most anterior contour (APt) relative to the anteroposterior length of the tibial plateau (AP). AM, anteromedial; NR, nonremnant; PL, posterolateral; RP, remnant-preserving.
CT Evaluation of the Degree and Incidence of Tunnel Enlargement
At 1 year after surgery, tibial tunnel coalition at 10 mm from the joint surface was observed in 5 knees (20.0%) in the NR group and 9 knees (39.1%) in the RP group (P = .145). Therefore, only the remaining 20 knees in the NR group and 14 knees in the RP group were included in the assessment of tunnel enlargement. A post hoc power analysis indicated that power was 60% with an alpha of .05.
In the NR group, the mean degree of tunnel enlargement for the AM bundle was –1.5% ± 16.7% and 0.8% ± 22.4% in the sagittal and axial planes, respectively; for the PL bundle, these values were 0.8% ± 20.4% and –6.6% ± 27.3%, respectively (Table 4). In the RP group, the mean degree of tunnel enlargement for the AM bundle was 6.9% ± 22.1% and 3.3% ± 20.7% in the sagittal and axial planes, respectively; for the PL bundle, these values were 0.2% ± 20.6% and 31.9% ± 50.8%, respectively. The degree of PL tunnel enlargement in the axial plane was significantly higher in the RP group than in the NR group (P = .007). AM tunnel enlargement was positively correlated with PL tunnel enlargement in both the sagittal and axial planes (sagittal: r = 0.40, P = .017; axial: r = 0.35, P = .036). AM tunnel enlargement in the sagittal plane was positively correlated with patient age (r = 0.35, P = .040), with no significant correlation between age and other tunnel enlargement parameters.
Degree of Tunnel Enlargement at 1 Year After ACL Reconstruction a

a Data are reported as mean ± SD in percentages. ACL, anterior cruciate ligament; AM, anteromedial; NR, nonremnant; PL, posterolateral; RP, remnant-preserving.
In the NR group, the incidence of tunnel enlargement for the AM bundle was 10.0% and 25.0% in the sagittal and axial planes, respectively; for the PL bundle, these values were 10.0% and 10.0%, respectively. In the RP group, the incidence of tunnel enlargement for the AM bundle was 35.7% and 14.2% in the sagittal and axial planes, respectively; for the PL bundle, these values were 14.2% and 50.0%, respectively. There were no significant between-group differences in the incidence of AM tunnel enlargement (sagittal: P = .083; axial: P = .378) or PL tunnel enlargement in the sagittal plane (P = .574). The only significant difference was noted for the incidence of PL tunnel enlargement in the axial plane (P = .014).
Relation Between Tunnel Enlargement on CT and Graft-to-Bone Integration on MRI
To evaluate the relationship between tunnel enlargement and graft-to-bone integration, the 48 knees were divided again into 2 groups according to the presence or absence of tunnel integration at 1 year after surgery (nonintegration vs integration). For the 34 knees that did not show tunnel coalition at 1 year postoperatively, 17 AM tunnels and 22 PL tunnels were found to exhibit graft-to-bone integration on MRI. The degree of AM tunnel enlargement on axial CT was significantly smaller in the integration group than in the nonintegration group (12.5% ± 15.6% [n = 17] vs –8.7% ± 21.5% [n = 17], respectively; P = .002), but no significant between-group differences were noted for AM tunnel enlargement on sagittal CT (5.0% ± 18.0% [n = 17] vs –1.0% ± 20.6% [n = 17], respectively; P = .386) or for PL tunnel enlargement on sagittal (–5.8% ± 17.3% [n = 12] vs 3.6% ± 20.8% [n = 22], respectively; P = .190) and axial CT (13.9% ± 62.1% [n = 12] vs 3.1% ± 23.9% [n = 22], respectively; P = .476) (Figure 7).

Comparison of the degree of tunnel enlargement between the graft-to-bone integration group (−) and nonintegration group (+) at 1 year after surgery. The degree of enlargement is shown for the anteromedial (AM) and posterolateral (PL) tunnels in axial and sagittal views. Error bars represent SDs. Only statistically significant differences are mentioned. CT, computed tomography; MRI, magnetic resonance imaging.
Discussion
The impact of remnant preservation on the outcomes of ACL reconstruction remains debatable. A previous meta-analysis suggested that RP single-bundle ACL reconstruction could prevent tibial tunnel enlargement, although it did not affect functional recovery. 33 However, in the present study, RP double-bundle ACL reconstruction did not have any beneficial effect on tunnel enlargement. Furthermore, we found that tibial tunnel enlargement at 1 year after reconstruction did not affect graft-to-bone integration in the tibial tunnel, the only exception being AM tunnel enlargement on axial CT.
Tibial tunnel position is important for achieving stability after ACL reconstruction, 6 and consequently, relevant bony/anatomic landmarks around the tibial footprint have been described. 32 Furthermore, 1 study showed that, in RP ACL reconstruction, surgeons could reproducibly create anatomic tibial tunnels based on these landmarks. 26 Kondo et al 20 reported no significant differences concerning the tunnel position between RP and remnant-resecting ACL reconstruction. In our present study, the RP technique did not influence tibial tunnel position, which is consistent with previous observations 20,26 and suggests that tunnel enlargement is not related to deviations in the tunnel position. Our first hypothesis was therefore confirmed.
RP ACL reconstruction is expected to prevent or minimize tunnel enlargement by inhibiting synovial fluid influx into the bone tunnel, resulting in accelerated biological healing of the graft-tunnel interface. 31,38 Nevertheless, it is important to note that the hamstring graft may become partially detached from the tibial tunnel wall because of the force pulling the graft posterolaterally. 27 This space between the graft and bone may allow the influx of synovial fluid containing elevated levels of cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor–α, leading to osteolysis and tunnel enlargement. 40 On the other hand, if the remnant covers the tibial tunnel aperture completely, synovial fluid influx into the tunnel may be prevented.
Graft micromotion at the tunnel aperture represents another potential cause of tunnel enlargement. 16,37 If the remnant promotes graft-to-bone integration, such detrimental motion may resolve sooner. Indeed, Wu et al 38 reported that remnant preservation in ACL reconstruction improved tendon-to-bone integration in a rabbit model, while Matsumoto et al 21 showed that remnant tissue enhanced tendon-bone healing in a canine ACL reconstruction model. However, a previous clinical study reported that RP ACL reconstruction minimized tunnel enlargement, which is opposite to our present observations. 39
A recent anatomic study showed that the tibial ACL midsubstance and the “direct” insertion are flat and “C” shaped, measuring 3.9 and 3.3 mm in thickness, respectively, with “indirect” fibers extending from the direct insertion site anteriorly and broadly spreading toward the anterior rim of the tibial plateau. 30 The findings of our study indicate that it is practically impossible for the remnant to cover tunnel apertures with diameters of 5.6 to 6.1 mm. In fact, a previous clinical study employing fast spin-echo proton density–weighted MRI reported that, at 3 months postoperatively, higher signal intensity between the graft and bone was observed in almost all tibial tunnels with remnant preservation, suggesting that RP ACL reconstruction did not promote graft-to-bone integration. 23 While it remains uncertain why PL tunnel enlargement in the axial plane was higher in the RP group than in the NR group, we conclude that our second hypothesis was rejected.
The impact of tunnel enlargement on graft-to-bone integration after ACL reconstruction remains largely unclear, while the effect of tunnel enlargement on clinical outcomes has been discussed and is still under debate. 5,11,17,19,39 Harris et al 15 demonstrated that tunnel enlargement did not adversely affect the histological incorporation of the graft in a goat model. In the present study, we also found no association between tunnel enlargement and graft-to-bone integration at 1 year after ACL reconstruction, the only exception being for AM tunnel enlargement on axial CT. Tunnel enlargement has been reported to typically occur within 6 months after ACL reconstruction 5,19 and particularly within the first 6 weeks. 13,15 While it is possible that not only graft-to-bone integration but also bone ingrowth into the tunnel continued after tunnel enlargement reached a maximum (at 1 year after ACL reconstruction), we found that only AM tunnel enlargement on axial CT affected graft-to-bone integration. Araki et al 3 reported that the largest amount of migration was observed in the centroids of the tibial AM bundle’s articular third. It was possible that the degree and direction of tibial tunnel transposition affected this in our results. Our third hypothesis was partially confirmed.
There are several limitations to this study. First, remnant tissue was not completely resected even in the NR group using a shaver or radiofrequency device so as not to damage bone tissue, potentially leading to reduced tunnel enlargement in the NR group, which would partially account for our conclusion regarding the lack of beneficial effect of remnant preservation. However, there were few residual stumps in almost all cases in the NR group, and ≥50% of the remnant was left in the RP group. Second, the mean patient age differed significantly between the NR and RP groups, which may have introduced bias related to age-specific effects. However, the patients were selected consecutively. Moreover, only AM tunnel enlargement in the sagittal plane was positively correlated with patient age (r = 0.35, P = .040). It is likely that there was a significant difference in bone mineral density, which may have affected the results. Nevertheless, a previous study showed that there was no correlation between tunnel enlargement and bone mineral density in an animal model of ACL reconstruction. 22 Therefore, the between-group difference in mean age is unlikely to have significantly affected our conclusions regarding the degree of tunnel enlargement.
Another limitation concerns the fact that patients in both groups were placed in a full extension brace for 1 week. A previous study showed that the increase in tibial tunnel diameters observed in a brace-free accelerated rehabilitation group was significantly higher than that observed in those immobilized for 2 weeks. 35 Immobilization for 1 week would reduce the widening differential between the 2 groups. A fourth limitation is that the sample size was relatively small for the purpose of comparing tunnel enlargement between the NR and RP groups because we excluded patients with tunnel coalition, thus having an underpowered test population (power was 60%). In the patients with tunnel coalition, it was impossible to precisely measure the widths of the bone tunnels. Moreover, the follow-up rate was low because of a high number of reruptures and because not all patients provided informed consent to undergo CT.
Our series contained many senior high school students. The patients with reruptures had returned to competition earlier than we intended because it was the last season of high school sports. Also, because many patients later moved to another area for college or employment after high school graduation, some patients were lost to follow-up at 1 year after surgery. Furthermore, a few female patients indicated a possibility of pregnancy. Fifth, the follow-up period was just 1 year, although previous studies have suggested that tunnel enlargement typically occurs within the first year after ACL reconstruction. 5,13,15,19 Finally, tunnel migration was not evaluated in this study. Despite these limitations, the present study provides orthopaedic surgeons with important information on ACL reconstruction with remnant preservation.
Conclusion
ACL reconstruction with remnant preservation did not influence tibial tunnel position and did not decrease the degree or incidence of tibial tunnel enlargement. At 1 year postoperatively, tunnel enlargement did not affect graft-to-bone integration in the PL tunnel, but graft-to-bone integration was delayed in the AM tunnel.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the ethical committee of Hirosaki University Hospital.