
Abstract
Background:
The effect of microfracture (MF) or surgical debridement of concomitant full-thickness cartilage lesions in anterior cruciate ligament–reconstructed knees on patient-reported outcomes remains to be determined.
Purpose:
To evaluate the effect of debridement or MF compared with no surgical treatment of concomitant full-thickness cartilage lesions on patient-reported outcomes 5 years after anterior cruciate ligament reconstruction (ACLR).
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Included in this study were 644 patients who were registered in the Norwegian and the Swedish National Knee Ligament Registries from 2005 to 2008 as having undergone unilateral primary ACLR and having a concomitant full-thickness cartilage lesion (International Cartilage Repair Society [ICRS] grades 3-4). Of these patients, 129 were treated with debridement, 164 were treated with MF, and 351 received no surgical treatment simultaneously with ACLR. At 5-year follow-up, 368 (57%) patients completed results on the Knee injury and Osteoarthritis Outcome Score (KOOS). Multivariable linear regression was used to estimate the effect of surgical debridement or MF of concomitant full-thickness cartilage lesions on patient-reported outcomes 5 years after ACLR.
Results:
Compared with no surgical treatment, there were no unadjusted or adjusted effects of debridement or MF of concomitant full-thickness cartilage lesions on KOOS scores at 5-year follow-up.
Conclusion:
Compared with leaving concomitant full-thickness cartilage lesions untreated at the time of ACLR, debridement and MF showed no effect on patient-reported outcomes 5 years after surgery.
Keywords
Anterior cruciate ligament (ACL) injuries are commonly associated with focal cartilage lesions. In reports from large, sprospectively collected ACL cohorts, such as the Norwegian and Swedish National Knee Ligament Registries (NKLR and SKLR, respectively), concomitant full-thickness cartilage lesions (International Cartilage Repair Society [ICRS] grades 3-4) were present in 7% of ACL reconstructions (ACLRs). 23 In addition to being a significant predictor of later osteoarthritis of the knee joint, 6,15 a full-thickness cartilage lesion at the time of ACLR has been shown to have significant adverse effects on patient-reported outcomes. 7,23
Previous literature has focused on comparing different surgical interventions, to a large extent circumnavigating the need for control groups and long-term follow-up. 18 To that end, very little is known regarding the natural history of concomitant focal cartilage lesions.
There is a lack of knowledge regarding to what extent surgical interventions affect these lesions. Various surgical treatment options, ranging from debridement to advanced cell-based techniques, exist. 17 In addition to leaving the cartilage lesion untreated, debridement and microfracture (MF) are the most commonly used surgical treatment options. 10 However, only 1 randomized study 14 and 1 prospective cohort study 24 on the issue of ACLR with concomitant treatment of cartilage lesions have been published. 14,24 Hence, there is insufficient evidence to support any surgical gold-standard treatment option.
The primary objective of the present 5-year follow-up after ACLR was to evaluate the effect of surgical debridement or MF as compared with no surgical treatment of concomitant full-thickness cartilage lesions on patient-reported outcomes.
Methods
NKLR and SKLR
After obtaining approval from the Regional Committee for Medical Research Ethics of South-Eastern Norway, University of Oslo, data were assembled from the NKLR and SKLR. The 2 national registries aggregate data from all surgical procedures performed on knee ligaments and prospectively monitor outcomes on a nationwide scale. 12,13 There are no major differences in the collection of data between the 2 countries, and in both registries, the surgeons’ reporting rates are found to be satisfactory, with rates above 85%. 1,13
The surgeons report patient-, knee-, and surgery-specific variables to the registries. As a part of that registration, the surgeons grade concomitant focal cartilage lesions according to the ICRS guidelines. 4,5 Cartilage lesion size is reported as area <2 cm2 or ≥2 cm2. The treating surgeon determines the treatment of concomitant cartilage lesions.
Before surgery, the patients complete an informed consent form allowing for later use of their registry data, including results on the Knee injury and Osteoarthritis Outcome Score (KOOS), which is used as the patient-reported outcome measure. The KOOS questionnaire consists of 42 questions distributed between 5 separately scored subscales: Pain, Symptoms, Activities of Daily Living (ADL), Sport and Recreation (Sport/Rec), and Knee-Related Quality of Life (QoL). It is established as a valid, reliable, and responsive assessment tool for patients with ACL and cartilage injuries. 2,9,22
Patients
The current study is a longitudinal 5-year follow-up of a nationwide population-based cohort consisting of all patients who underwent unilateral primary ACLR between January 1, 2005, and December 31, 2008, and who were registered in the NKLR or SKLR with a concomitant ICRS grade 3 or 4 cartilage lesion. A total of 1012 patients were prospectively registered. This patient cohort has previously been described in a study on the effects of surgical debridement or MF of concomitant full-thickness cartilage lesions on 2-year patient-reported outcomes. 24
Apart from having a full-thickness cartilage lesion and completing the KOOS preoperatively, eligible patients had to be registered as undergoing no treatment, debridement, or MF of the cartilage lesion. Patients with more than 1 concomitant cartilage lesion were categorized according to the lesion with the highest ICRS grade. Overall, 368 patients did not meet the inclusion criteria because of missing preoperative KOOS data (n = 239) or because the treatment of the cartilage lesion was not reported or was reported as other than no treatment, debridement, or MF (n = 129). Of the 644 patients who fulfilled the inclusion criteria, 351 (54%) received no surgical treatment of their cartilage lesion at the time of ACLR, 129 (20%) were treated with debridement, and 164 (26%) were treated with MF.
At a mean follow-up of 5.1 ± 0.1 years, KOOS data were available for 368 (57%) of the included patients, who had a mean age of 41.2 ± 10.4 years. There were 276 (43%) patients who did not return their 5-year follow-up KOOS questionnaire and were considered lost to follow-up. Patient flow during inclusion and follow-up is shown in Figure 1, and baseline characteristics at the time of ACLR for the patients available for follow-up and those lost to follow-up are shown in Table 1. Patients lost to follow-up tended to be younger, and a higher proportion of them were male. Except for a difference in the proportion of grade 4 lesions and the prevalence of >1 full-thickness cartilage lesions, there were no substantial differences between these groups in baseline characteristics.
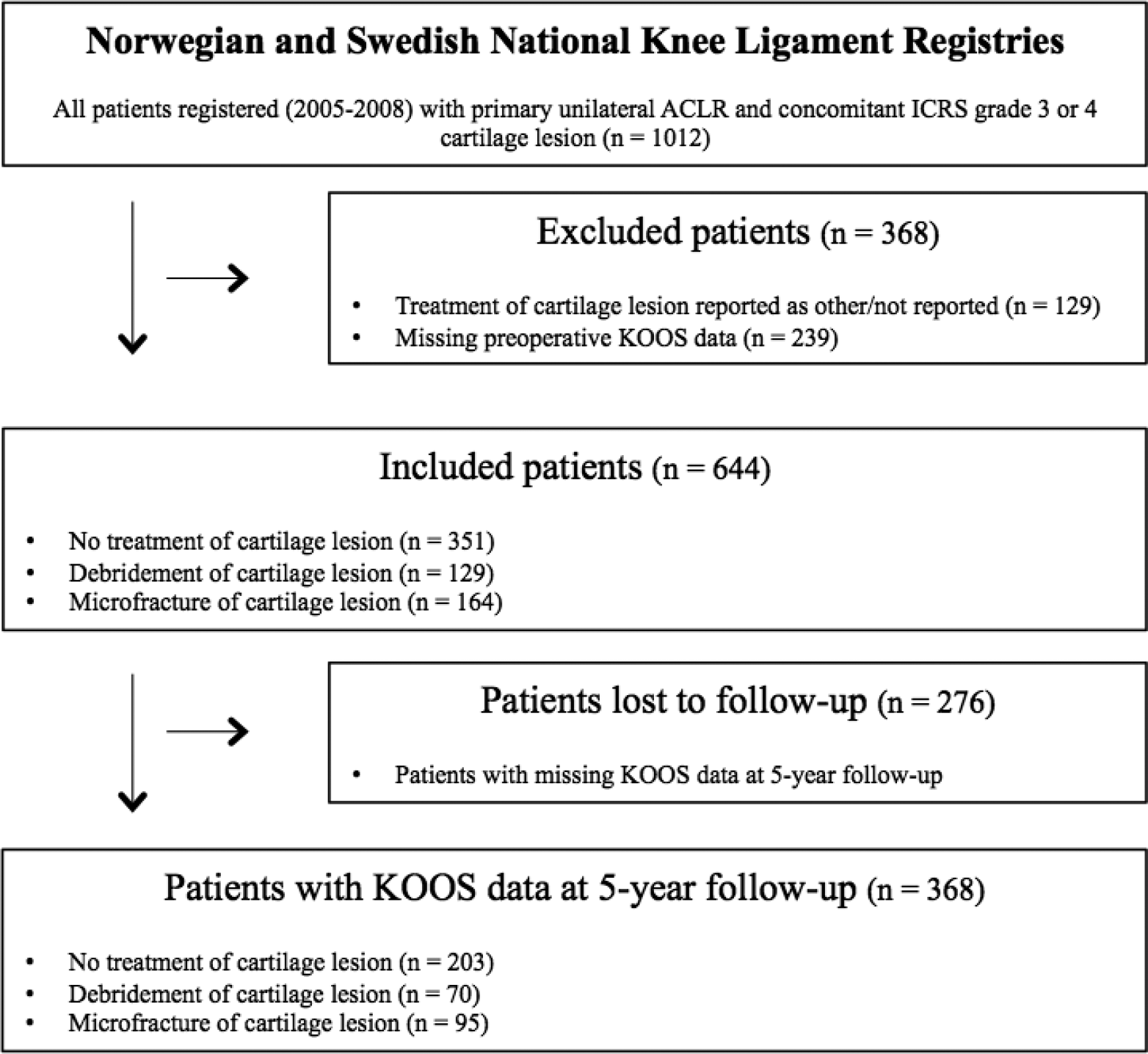
Flowchart of the patients during inclusion and follow-up. ACLR, anterior cruciate ligament reconstruction; ICRS, International Cartilage Repair Society; KOOS, Knee injury and Osteoarthritis Outcome Score.
Baseline Characteristics at the Time of ACL Reconstruction a
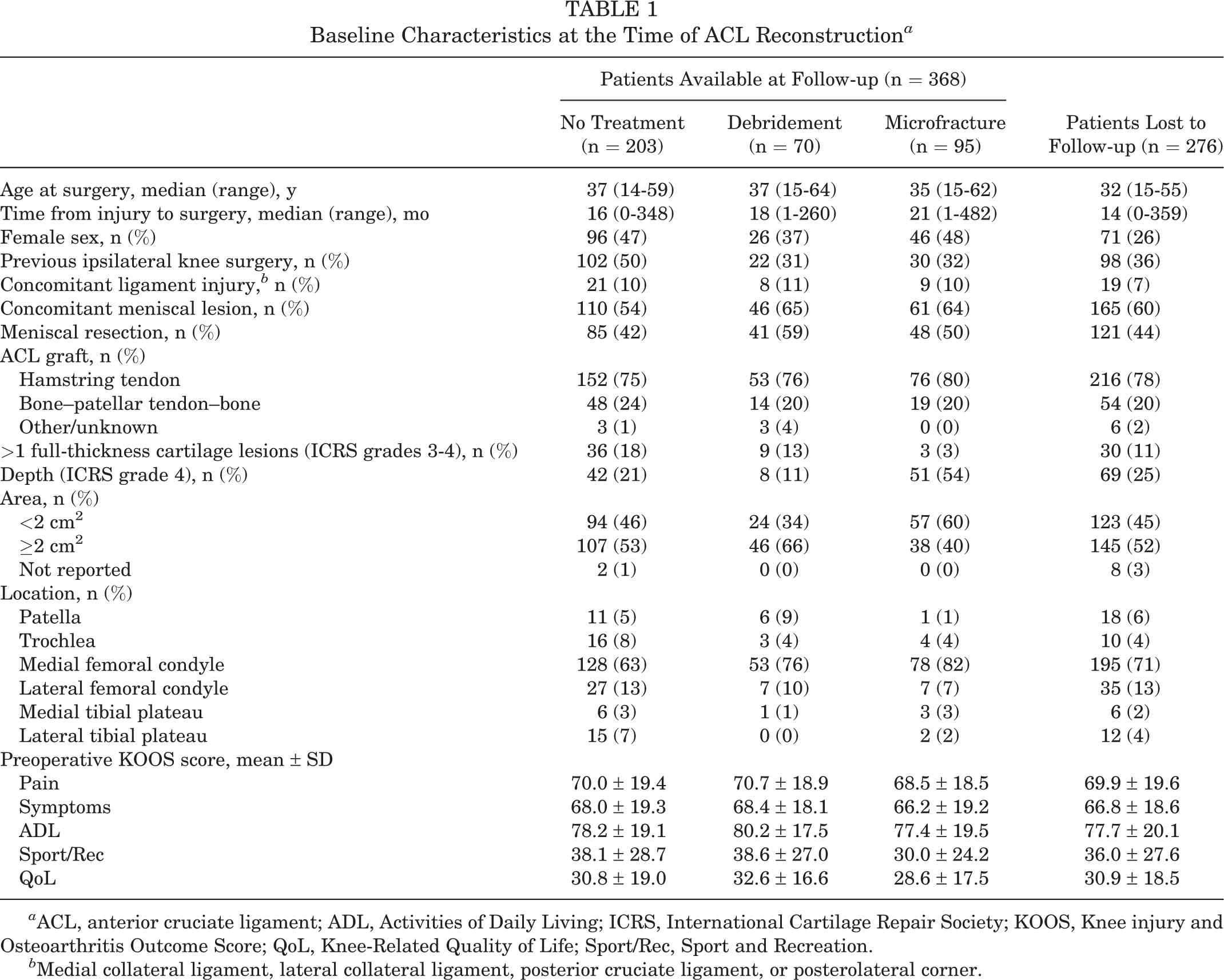
a ACL, anterior cruciate ligament; ADL, Activities of Daily Living; ICRS, International Cartilage Repair Society; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Knee-Related Quality of Life; Sport/Rec, Sport and Recreation.
b Medial collateral ligament, lateral collateral ligament, posterior cruciate ligament, or posterolateral corner.
Statistical Analysis
SPSS software version 24.0 (IBM) was used for all statistical analyses. P values <.05 were considered statistically significant. Crude mean KOOS scores and standardized regression coefficients are presented with 95% CIs.
Crude mean KOOS scores preoperatively and at 5-year follow-up were estimated and stratified by treatment (ie, no treatment, debridement, or MF) of concomitant cartilage lesions. Multivariable linear regression was used to assess the possible impact on 5-year follow-up KOOS scores of surgical debridement or MF for concomitant full-thickness cartilage lesions. No surgical treatment of full-thickness cartilage lesions was used as a reference in all regression analyses. Results are presented as both unadjusted and adjusted for possible confounding from sex, age at surgery (continuous variable), previous ipsilateral knee surgery (yes/no), concomitant ligament injury (yes/no), concomitant meniscal injury (yes/no), concomitant meniscal resection (yes/no), time from injury to surgery (continuous variable), area of cartilage lesion (<2 cm2 or ≥2 cm2), depth of cartilage lesion (ICRS grade 3 or 4), location of cartilage lesion (patella, trochlea, medial femoral condyle, lateral femoral condyle, medial tibial plateau, or lateral tibial plateau), type of ACL graft (hamstring, patellar tendon, or other), and preoperative KOOS subscale scores (continuous variable).
Results
Of the 368 patients available for follow-up at 5 years, 203 (55%) patients received no surgical treatment of their full-thickness cartilage lesion at the time of ACLR, 70 (19%) were treated with debridement, and 95 (26%) were treated with MF. The crude mean KOOS scores for the 3 study groups (ie, no treatment, debridement, and MF) are shown in Table 2. Figure 2 illustrates the changes in mean KOOS scores from preoperatively to 5-year follow-up for the 3 study groups. The results for the unadjusted and adjusted effects of debridement and MF on each of the KOOS subscales at 5-year follow-up are shown in Table 3. With no treatment of concomitant cartilage lesions as the reference, there were no significant effects of debridement or MF detected in the unadjusted or adjusted regression analyses on any of the KOOS subscales at 5-year follow-up. However, based on the 95% CIs, there was a trend in both the unadjusted and the adjusted analyses toward negative effects of MF on the KOOS Sport/Rec and QoL subscales.
Crude KOOS Scores by Treatment of Cartilage Lesions at 5-Year Follow-up After Anterior Cruciate Ligament Reconstruction a

a Values are shown as mean (95% CI). ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Knee-Related Quality of Life; Sport/Rec, Sport and Recreation.
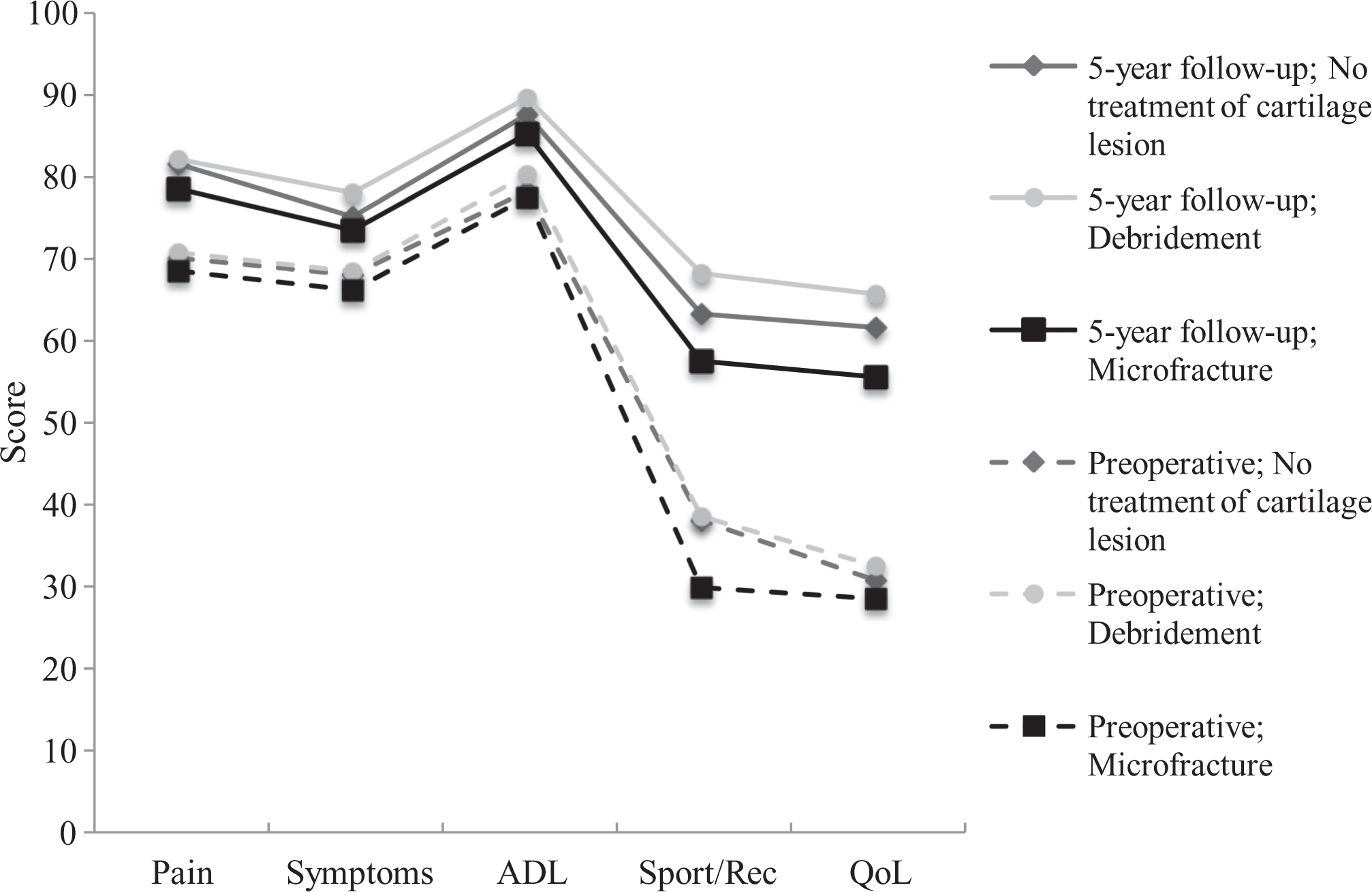
Profiles of mean Knee injury and Osteoarthritis Outcome Score values of patients undergoing no treatment, debridement, or microfracture of concomitant full-thickness cartilage lesions preoperatively and at 5-year follow-up after anterior cruciate ligament reconstruction. ADL, Activities of Daily Living; QoL, Knee-Related Quality of Life; Sport/Rec, Sport and Recreation.
Unadjusted and Adjusted Regression Analyses of the Associations Between KOOS Subscales and Treatment of Cartilage Lesions at 5-Year Follow-up After ACL Reconstruction a

a Adjusted for sex, age, previous ipsilateral knee surgery, time from injury to surgery, concomitant ligament injury, concomitant meniscal lesion, meniscal resection, type of ACL graft, area of cartilage lesion, depth (International Cartilage Repair Society) of cartilage lesion, location of cartilage lesion, and preoperative KOOS scores. ACL, anterior cruciate ligament; ADL, Activities of Daily Living; β, regression coefficient; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Knee-Related Quality of Life; Sport/Rec, Sport and Recreation.
b No treatment of cartilage lesions used as the reference.
Discussion
The main finding of the present study is that, compared with patients who received no surgical treatment of their concomitant full-thickness cartilage lesion at the time of ACLR, surgical debridement and MF had no effect on patient-reported outcomes as measured by the KOOS at 5-year follow-up. To date, this is the largest multivariable model assessing the midterm outcomes of the surgical treatment of these concomitant injuries and the only study to have included a control group with the cartilage lesion left untreated.
The findings from the present 5-year longitudinal follow-up indicate a loss of magnitude of the adverse effects of MF over time, as significant negative effects of MF on KOOS scores were observed at 2-year follow-up in the same cohort. 24 Nevertheless, there was a trend in the analyses toward negative effects of MF on the KOOS Sport/Rec and QoL subscales in the present study as well, thus adding support to the view that there should be a restrictive use of MF as a first-line treatment of full-thickness cartilage lesions in the setting of ACLR. Compared with the 2-year follow-up of the current cohort, the crude mean KOOS Sport/Rec and QoL subscores improved for all 3 patient categories, but no significant between-group differences in change over time were observed.
In the only randomized study on the concomitant treatment of cartilage lesions in the setting of ACLR, Gudas et al 14 compared the 3-year patient-reported outcomes after debridement, MF, and osteochondral autograft transfer (OAT). Those authors reported significantly better outcomes, as measured by the International Knee Documentation Committee (IKDC) form, in patients treated with OAT than in patients treated with MF or debridement. Moreover, no differences were detected between patients treated with MF and debridement. 14 However, the absence of a control group of patients with the cartilage lesion left untreated in that study makes it difficult to evaluate the actual effect of MF or debridement.
Despite an emerging recognition that the results after MF deteriorate over time, 16,20 it remains the most commonly performed cartilage procedure. 11,18 In addition to the inferior biochemical and histological properties associated with the resultant fibrocartilaginous repair tissue, more recently, subchondral bone overgrowth has been suggested as another factor in the deterioration of knee function seen in some patients after MF. 19 However, the current observational study design does not allow for assessments regarding those aforementioned factors. Even if debridement usually is understood as a removal of unstable or loose flaps of cartilage to leave stable edges of the lesion, the potential of variation and diversity during surgery is present. There are indications that aggressive, deep removal of the calcified cartilage layer represents a significant risk factor for subchondral bone overgrowth. 19 As subchondral bone overgrowth has been associated with postoperative failure after MF, one might hypothesize that this phenomenon might play a role in the postoperative course after debridement as well. Nevertheless, when compared with no treatment of full-thickness cartilage lesions, debridement showed no effect on KOOS scores at 2-year and 5-year follow-up in the current cohort. That finding is in line with the findings in a recent randomized controlled trial demonstrating no benefit of debridement of chondral lesions encountered during arthroscopic partial meniscectomy. 3 However, as pointed out in a recent systematic review, 10 considerable heterogeneity in patients, injuries, surgical factors, outcome measurements, and observation periods exists among the different reports, making it difficult to directly compare the findings from these studies.
The observational study design has limitations, as is the case in the present study as well. The main limitation of the present study is the rate of loss to 5-year follow-up (43%), with the potential of introducing attrition bias. Even though the baseline characteristics of the study cohort and those lost to follow-up were comparable in the majority of the reported baseline variables, patients lost to follow-up were younger, had a higher proportion of men, and had a shorter time from injury to surgery than the patients available for follow-up. As cartilage surgery tends to be more successful in young patients with fewer long-standing cartilage lesions, there is a possibility that those patients lost to follow-up have affected the results. 8 On the other hand, those factors, together with other factors most likely to have affected the prognosis and outcomes after surgery, were adjusted for in the multivariable regression analyses. Moreover, in a validation of the Danish Ligament Reconstruction Register, the KOOS scores from nonresponders were comparable with those of responders, thus indicating that registry data could be valid despite a high rate of loss to follow-up. 21 Other limitations are the lack of randomization and the use of the KOOS as the only outcome measure. Supplementary outcome measures, such as radiographic assessments of osteoarthritis and activity level scales, would have strengthened the present study and reduced the potential risk of unmeasured predictors and confounders. Randomization would have reduced the potential risk of uneven distribution of such hidden confounders and predictors.
The main strengths of the present study are the large sample size and the inclusion of a control group of patients with the concomitant cartilage lesion left untreated. Thus, we were able to investigate the actual treatment effect of debridement and MF on patient-reported outcomes. Moreover, the inclusion of patients from nationwide population-based registries ensures the representation of a wide range of patients, hospitals, and surgeons. This should in turn provide results that are relevant to most clinical settings. Finally, the comprehensive adjustment for predictors and confounders in the analyses should provide valid estimates of the effect of the different surgical treatment options. However, it will often be a matter of discussion whether the appropriate confounders have been controlled for. There are no standardized or validated sets of possible confounding variables considered to be requisite, so the included variables had to be based on the current literature, clinical assumptions, and available parameters recorded by the 2 national registries. Possible confounding variables such as smoking status, body mass index, and energy of the initial trauma were not included in the current regression model. However, because of the even distribution of patients lost to follow-up between the groups, the demographic similarities between the groups, and the comprehensive adjustment for possible confounders in the regression analyses, it is not likely that additional adjustments would alter the results substantially. At least, it is highly unlikely that the results would be altered to the extent that they would demonstrate a beneficial effect of MF.
In summary, the findings in the present study should be taken into account and assist patient counseling and decision making regarding the surgical treatment of concomitant cartilage lesions. The findings in the present study suggest that the concomitant treatment of full-thickness cartilage lesions with MF or debridement does not show the anticipated effect on patient-reported outcomes at midterm follow-up after ACLR. More research is needed to optimize the clinical management of these combined injuries and, in addition to including a control group with the cartilage lesion left untreated, should focus on identifying whether there are any subgroups of patients that benefit from debridement or MF.
Conclusion
Compared with leaving concomitant full-thickness cartilage lesions untreated at the time of ACLR, debridement and MF showed no effect on patient-reported outcomes at 5-year follow-up. Taking into account the fact that MF showed significant adverse effects on KOOS scores at 2-year follow-up in the current cohort, 24 MF should probably be used with caution in the setting of ACLR.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partially funded by the Norwegian Regional Health Authorities and Akershus University Hospital.
Ethical approval for this study was obtained from the Regional Committee for Medical Research Ethics of South-Eastern Norway, University of Oslo (ID: 2017/12).
Acknowledgment
The authors thank the NKLR and the SKLR for providing data for the current study, the Oslo Sports Trauma Research Center for advisory support, and Akershus University Hospital for economic support while the study was being constructed.