
Abstract
Background:
There is no standard method for the surgical treatment of acromioclavicular (AC) joint separations. Current techniques have associated complications, including need for device removal, coracoid fracture, and inadequate reduction.
Purpose:
To evaluate the clinical outcomes of an internal splint technique without graft augmentation or rigid fixation to treat acute Rockwood type IV and V AC joint injuries.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective analysis was performed of 26 patients who underwent a novel internal splint fixation technique between 2011 and 2016. Patients had type IV (n = 2) and type V (n = 24) acute AC separations. The mean time to surgery was 13.7 days (range, 1-28 days). The surgical technique included an open approach with coracoclavicular suture and tape fixation and AC suture fixation. Range of motion, strength, and radiographs were evaluated after surgery. Patient follow-up included the DASH (Disabilities of the Arm, Shoulder and Hand) questionnaire at a mean 3.3 years postoperatively (range, 6 months–8.6 years). DASH questionnaires were obtained for all patients via email. Patients were also surveyed on cosmetic appearance and willingness to undergo the operation again.
Results:
All patients regained full strength and range of motion following surgery. All postoperative radiographs demonstrated well-maintained reduction of the AC joint. The mean DASH score was 3.4 at final follow-up, and 23 of 26 respondents were satisfied with their postoperative shoulder appearance. There were no reoperations, and all patients stated that they would have the operation again given the same circumstances.
Conclusion:
The results of this study demonstrate a reliable new technique for acute fixation of type IV or V AC joint injuries via an internal splint construct. This technique enables reduction in the coronal and sagittal planes without the need for graft augmentation or a rigid implant, allowing healing of the coracoclavicular and AC ligaments.
Keywords
Despite acromioclavicular (AC) joint separations being one of the most common upper extremity injuries, there is still no current standard operative technique for surgical treatment of these injuries. It is generally accepted that nonoperative treatment is appropriate for Rockwood type I or II AC joint injuries. 18 Type III AC separations demonstrate similar shoulder function and levels of radiographic osteoarthritis of the AC joint between surgical and nonoperative management. 9 Treatment of type III AC separations frequently depends on the physical demands of the patient and his or her age and wishes. 9 The treatment options for more severe AC separations, Rockwood type IV or V, tend to be more operative but remain controversial. 18 A recent prospective multicenter randomized controlled trial indicated no difference in shoulder function or overall general health status between nonoperative treatment and operative treatment with a hook plate. 4,13 Chronic injuries are often treated with a form of graft augmentation, 23 but there is still much debate about how to best surgically address the acute type IV or V AC separation.
Over the years, a number of new techniques have been described in conjunction with the development of orthopaedic devices designed for this problem. Such devices include the hook plate or adjustable suture button. However, complications associated with the use of these and other devices have made it difficult to establish a reliable, relatively complication-free surgical treatment method for patients acutely presenting with significant AC joint injuries. 14,15,19,20
The purpose of our study was to determine the clinical and patient-reported outcomes of an internal splint technique used to treat acute type IV and V AC joint injuries at our institution. We hypothesized that patients will have return of shoulder range of motion equal to that of the contralateral shoulder and will self-report improved outcomes and a satisfactory cosmetic appearance.
Methods
Between 2011 and 2016, all patients undergoing acute surgical fixation (within 4 weeks of injury) for isolated type IV and V AC joint separations at a tertiary referral center were included. Exclusion criteria were type I to III AC joint separations and concomitant injuries. Demographic variables were recorded, including age, sex, date of presentation, mechanism of injury, type of AC injury, and date of surgery. Type of injury was determined by 1 of 3 sports medicine fellowship–trained attending physicians (B.T.F., C.B.M., or A.L.Z.) on the basis of radiographs (anteroposterior [AP] shoulder, Zanca, and axillary lateral views) and physical examination as documented in the chart. Patients with type IV and V injuries were scheduled for acute surgical repair to be performed by the diagnosing surgeon within 4 weeks of the date of injury. Given the change from paper charts to electronic medical records, an exact date of injury was missing for 4 patients. In those cases, the patients were assigned a duration of 28 days from the time of injury to surgery, based on operative reports within the month of injury. All 3 surgeons performed the repair using the surgical technique described here, which did not change over this period. This study was approved by our institutional review board, and consent was obtained from all study patients.
Surgical Technique
The patient was positioned supine in the modified beach-chair position with the head of the bed angled approximately 35° to 40°. Intra-articular pathology was evaluated on preoperative radiographs and intraoperatively with fluoroscopy and direct visualization throughout the case. A 6- to 7-cm saber-type incision was centered over the distal clavicle 1 cm medial to the AC joint in line with the coracoid process. Upon the deltoid fascia, a transverse incision to bone was made in line with the distal clavicle and acromion, raising a deltoid muscular flap anteriorly in conjunction with releasing the coracoacromial ligament. A trapezial muscular flap was raised posteriorly to expose the posterior border of the clavicle. The released coracoacromial ligament was used as a guide to bluntly dissect to the coracoid. Once the coracoid was exposed, a right-angle clamp or Satinsky clamp was passed on either side of the coracoid to retrieve a No. 2 FiberWire (Arthrex), which was then used as a shuttling suture to pass a No. 5 FiberWire and 5-mm Mersilene tape (Johnson & Johnson). These were later used for reduction and fixation. A 3.5-mm drill bit was then used to drill holes at 3.0 and 4.5 cm medial to the distal clavicle to approximate the locations of the coracoclavicular ligaments. Drill holes were centered (anterior-to-posterior direction) on the clavicle and drilled in a superior-inferior direction. A Hewson suture passer was used to pull the ends of the No. 5 FiberWire and 5-mm Mersilene tape through the clavicle. A 2.5-mm drill was used to create a hole centered in the acromion (anterior-to-posterior direction) just lateral to the AC joint and drilled in a superior-inferior direction. Another No. 5 FiberWire was passed through this acromial drill hole. This No. 5 FiberWire was also shuttled through the lateral hole in the clavicle, but sometimes an entirely new 2.5-mm hole was created in the distal clavicle for this suture, depending on the amount of anterior-to-posterior translation required for reduction. The No. 5 FiberWire sutures (1 for coracoclavicular, 1 for AC) were then tied down sequentially to reduce the distal clavicle in the coronal and sagittal planes (Figure 1). Each AC joint was reduced under direct vision and accepted only once the anterior and superior borders of the clavicle were collinear with the respective borders of the acromion.
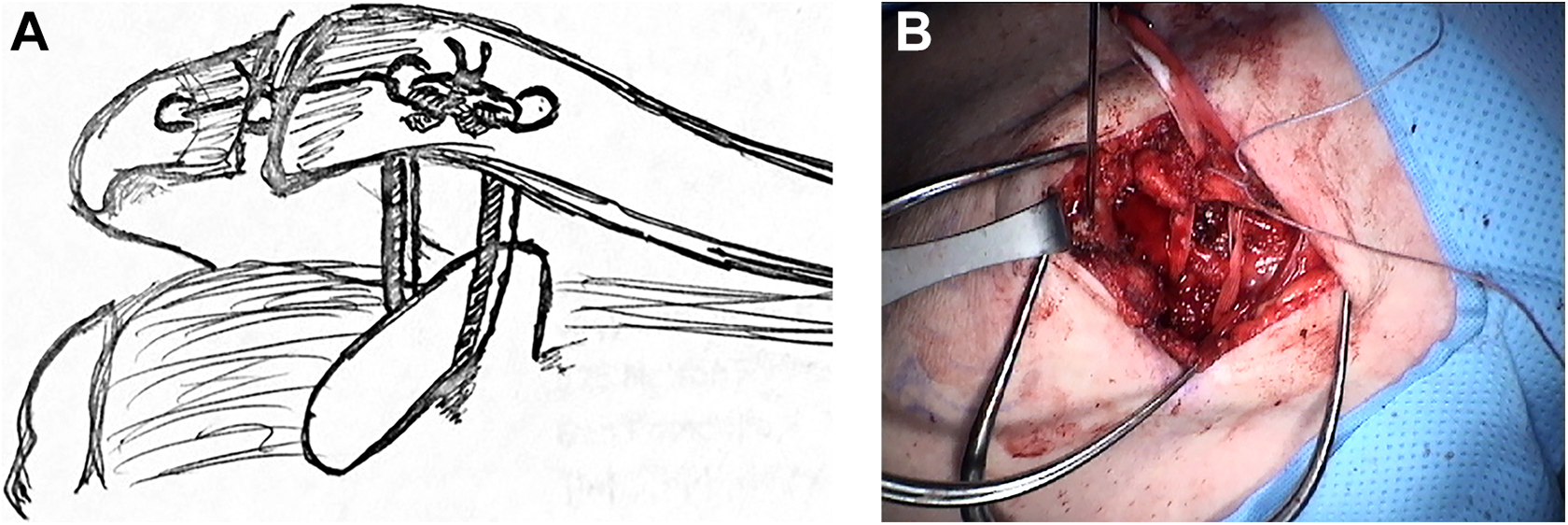
(A) Artist rendition of acromioclavicular acute repair technique. (B) Intraoperative photo of technique. A 5-mm Mersilene tape (Johnson & Johnson) and No. 5 FiberWire (Arthrex) are looped around the coracoid for reduction in the coronal plane. A separate No. 5 FiberWire is looped around the distal clavicle and acromion for reduction in the sagittal plane.
The Mersilene tape was then tied over the No. 5 FiberWire to augment the fixation around the coracoid (see Figure 1). The arm was then ranged to check for stability. The wound was irrigated and, after ensuring good deltotrapezial muscular coverage over the suture knots, was then closed. Postoperative radiographs (AP shoulder and Zanca views) were obtained to confirm maintenance of reduction (Figure 2).

(A) Preoperative radiograph demonstrating a type V acromioclavicular separation. (B) Postoperative radiograph demonstrating complete reduction of the acromioclavicular joint. Drill holes in the distal clavicle are visible.
Rehabilitation
Each patient was placed in a sling with an abduction pillow for 6 weeks. No shoulder motion was allowed until the sling was removed. Passive and active-assisted shoulder motion was started with physical therapy at 6 weeks, progressing to active motion by week 12. At 12 weeks, strengthening exercises were started with physical therapy. Patients were cleared for all activities between 4 and 6 months from surgery.
Data Collection
Physical examination documenting strength and range of motion at final clinic follow-up 6 months after surgery, as well as final postoperative radiographs, was performed by 1 of the 3 treating sports medicine surgeons. Range of motion assessment included shoulder forward flexion, abduction, external rotation, and internal rotation. Full range of motion was defined as being equal to that of the contralateral shoulder. Deltoid and rotator cuff strength was graded per the Oxford scale, with 5 of 5 indicating normal strength versus the contralateral side. Radiographs (AP, Zanca views, and axillary views) were compared with preoperative imaging for maintenance of reduction. Maintenance of reduction was determined by measuring the percentage of displacement (vs the superior-inferior width of the distal clavicle) in relation to the acromion and the Zanca and AP views. Horizontal displacement was measured on the axillary view as the percentage of displacement in the anterior-posterior direction of the distal clavicle in relation to the acromion. Additionally, charts were reviewed for any complications or reoperations.
Patients completed self-reported outcome measures, including the DASH (Disabilities of the Arm, Shoulder and Hand) questionnaire, via email or standard mail at latest follow-up. Added to the DASH questionnaire were 2 questions: “Are you happy with the appearance of your shoulder?” and “Would you have the operation again given the same circumstances?” DASH scores were graded on a scale from 0 to 100, with 0 being the best score and 100 being the worst.
Results
All 26 patients treated with this technique between 2011 and 2016 were included for analysis. Two patients had type IV injuries, and 24 had type V. There were 24 male and 2 female patients, with a mean age of 38.2 years (range, 22-56 years). The mean time to treatment was 13.7 days (range, 1-28 days).
Final clinic follow-up was at postoperative 6 months. At final clinic follow-up, all patients had regained full range of motion (forward flexion, abduction, internal rotation, and external rotation) and full strength (5 of 5) as compared with the contralateral side. Postoperative radiographic alignment demonstrated no displacement in the superior-inferior direction on final AP and Zanca radiographs.
Questionnaire follow-up occurred at a mean of 3.3 years (range, 6 months–8.6 years). Patients were contacted for verbal assessments after 1 year. There was an 100% response rate to questionnaires. The mean DASH score was 3.4 (mean, 0-16.7) (Table 1). Of 26 patients, 23 (88.5%) were happy with the appearance of their shoulders. All patients (26 of 26) said that they would have the operation again given the same circumstances.
Patient Data a
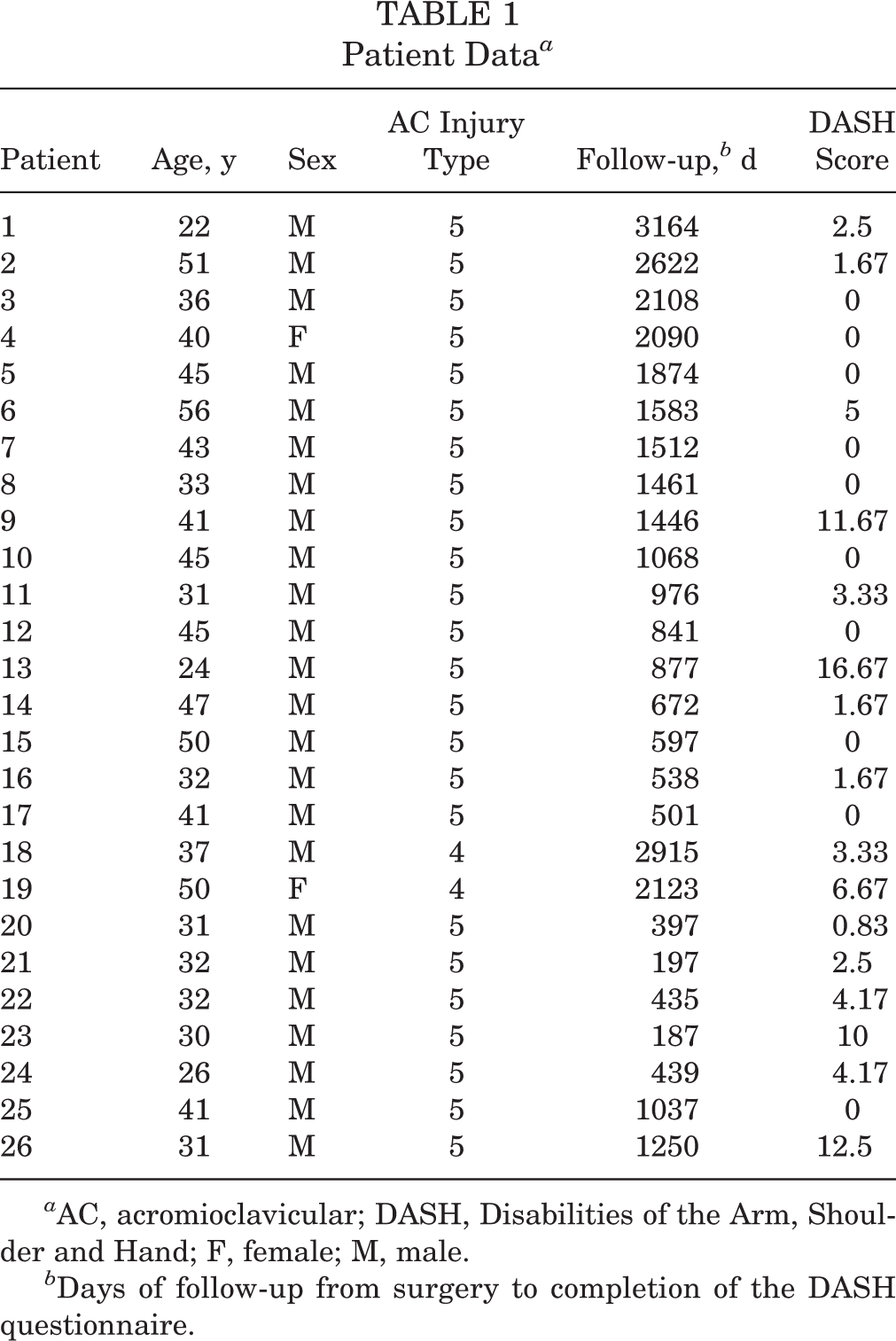
a AC, acromioclavicular; DASH, Disabilities of the Arm, Shoulder and Hand; F, female; M, male.
b Days of follow-up from surgery to completion of the DASH questionnaire.
Of the 26 patients, there were no reoperations. One patient sustained a reinjury to the ipsilateral shoulder. This patient fell onto the shoulder approximately 7 years after AC repair, fractured the distal clavicle in relation to the previous drill hole, and was subsequently treated nonoperatively. Despite the reinjury, this patient had a DASH score of 3.33, was satisfied with the appearance of the shoulder, and would have the operation again given the same circumstances. There were no instances of the FiberWire cutting through the coracoid process (per radiographs).
Discussion
In this study, we reported outcomes for an internal splint technique in the open treatment of acute AC separations that includes a simple coracoclavicular and AC repair. This addition of suture fixation of the AC repair adds horizontal stability (anterior to posterior) to the construct. At >3-year mean follow-up, patients were highly satisfied with the results and suffered no significant complications. At our institution, we consider injuries >4 weeks to be chronic. Therefore, only patients who underwent acute repair within 3 weeks from the date of injury were included. At our institution, we do perform the internal splint repair at 4 weeks without graft.
Previous studies regarding acute AC repair with or without suture augmentation included type III AC separations. 5,17,20,21 The inclusion of this group confounds the overall outcomes of acute repair. By excluding type III AC separations, this allows the current cohort to better reflect patients who would require surgical fixation, although it does make it harder to compare the results with other studies.
Unique to our internal splint technique is the use of Mersilene tape to augment the No. 5 FiberWire looped around the coracoid and through the clavicle. Blatter and Meier 3 looked at coracoclavicular augmentation techniques in acute repair of grade III AC injuries, evaluating 3 groups: 1.2-mm wire cerclage, 3 mm–wide Vicryl tape, and 1.5-mm polydioxane suture (PDS) cord. At a mean 4.4 years of follow-up, clinical evaluation revealed AC joint dislocation in 23% of the cerclage group, 58% of the PDS group, and only 20% of the Vicryl tape group. Additionally, weighted radiographic evaluation (8 kg) showed a 45% loss of reduction in the cerclage group, 58% loss in the PDS group, and only a 23% loss in the Vicryl tape group. Despite their use of resorbable tape augmentation, their success with tape lends support for our use of nonresorbable Mersilene tape.
A portion of our fixation technique involves coracoclavicular loop suture. Note that in this technique we did not perform a direct repair of the coracoclavicular ligament. To get exposure to pass the sutures around the coracoid, we thought that a reliable repair of the ligament was not possible. Furthermore, as this technique is used in acute injuries, reducing the AC joint will allow for natural healing of the coracoclavicular ligaments, which is the internal splint portion of the described technique. Prior studies, however, have indicated that there may be anterior displacement of the clavicle relative to the acromion with these constructs. 1,15 Baker et al 1 performed a biomechanical study examining orientation of the drill holes through the clavicle to determine how best to reduce sagittal plane deformity. However, even with anterior-superior to anterior-inferior drill hole orientation, which proved to be the best, the authors still noted between 2 and 3 mm of anterior displacement on average. In this series, the addition of an AC joint suture fixation appeared to also support horizontal stability, as all patients maintained their anterior-posterior as well as superior-inferior alignment at final radiographic follow-up.
In a 2011 study, Lädermann et al 11 described AC and coracoclavicular cerclage reconstruction for acute AC joint dislocations. Their technique also aimed to control the displacement of the AC joint in the coronal and sagittal planes. However, their technique included use of Ethibond suture (Ethicon) for AC and coracoclavicular fixation, and their suture knots were placed inferior to the clavicle. They showed good outcomes, with a mean DASH score of 7 and only 1 reoperation for suture irritation among 37 patients. However, while that study included type III AC separations, our study solely evaluated type IV and V AC injuries. Operative treatment of type III injuries is controversial, as some studies have shown excellent outcomes with nonoperative treatment. 2,8,12,21 In one of the longest-studied cohorts, which comprised 46 type III AC joint injuries treated nonoperatively, 42 of 44 patients had good outcomes at 5 years, and of the 30 patients available for evaluation at a mean 12.5 years after injury, 14 and 15 had excellent and good results, respectively, with only 1 having a fair outcome. 6,17 As type V injuries may require stronger fixation than that of type III injuries—given the greater energy associated with the injury through the deltotrapezial fascia, leading to disruption of the fascia and larger displacement of the distal clavicle—the current study’s focus of the internal splint technique in type IV and V injuries better applies to current surgical practices.
Another advantage of our technique is the low reoperation rate, as none of the respondents underwent a reoperation for failure of fixation or recurrent clavicular displacement. These low numbers are in contrast to the hook plate method, which is commonly used to address acute AC injuries or displaced distal clavicle fractures. By its very nature and the risk of acromial osteolysis, 7 the hook plate generally necessitates a second operation for removal. Metzlaff et al 15 compared hook plate fixation with minimally invasive cortical button fixation, and they removed all hook plates at a mean 11.9 weeks. Kumar and Sharma 10 removed hook plates at 16 weeks. Eschler et al 7 compared hook plate fixation with PDS fixation, and all hook plates were removed at 12 weeks. Similar to the hook plate, coracoid screw fixation requires a second operation for removal, 5 and Motamedi et al 16 demonstrated its significantly decreased failure load versus looped suture configurations. Recent studies of type III and IV AC separations, however, have indicated no difference in shoulder function or general health of patients between nonoperative management and operative open reduction and internal fixation with a hook plate. 4,13
Devices have been produced for minimally invasive anatomic repairs of AC separation, such as the adjustable suture button. 22 However, despite potentially avoiding the need for a second operation to remove hardware, this technique has demonstrated significant complications. Salzmann et al 19 observed 23 patients for 2 years after minimally invasive anatomic repair of acute AC injuries with 2 TightRope (Arthrex) devices. There was a significant improvement in visual analog scale pain scores and Constant scores, but postoperative radiographic alignment was unsatisfactory for 35% of their patients. Additionally, 1 patient sustained a coracoid fracture requiring revision, and 4 patients had subsidence of the clavicular buttons into the distal clavicle, leading to coronal displacement. A study by Martetschläger et al 14 evaluated 13 patients who underwent acute AC repair with cortical button fixation, and they noted complications for 23.1% of patients, including coracoid fracture and hardware failure. Scheibel et al 20 had an 89.3% (25 of 28) rate of implant migration in a dual TightRope technique for acute repair of type V AC injuries, and despite overall good patient-reported outcomes, 42.9% of patients had postoperative posterior AC instability, with significantly worse clinical outcomes as compared with those without postoperative posterior instability.
In this study, 1 patient had a complication of a distal clavicle fracture that was in relation to the drill holes. Fractures through clavicle drill holes, particularly for athletes in contact sports, are a risk of the internal splint technique. The described technique adds only 1 additional drill hole when compared with previously described techniques. This is a small hole (2.5 cm) in the acromion for anterior-posterior stabilization. In addition, because the described technique does not require graft placement, the 2 holes in the distal clavicle are small (3.5 cm). Although an additional drill hole likely increases the risk of fracture, the small-diameter holes reduce this risk. Moreover, the prescribed rehabilitation protocol—6 weeks in a sling and no return to activities until 4 to 6 months—provides ample time for bony ingrowth of the drill holes to further decrease risk of fractures.
Limitations
This was a retrospective study, which did not allow for a protocol-based evaluation. The sample size is limited in the cohort, but the goal of the study was to present pilot data for a novel fixation technique. Larger comparative cohort studies may be needed to compare outcomes and complications of this technique with others. Furthermore, the same operative treatment was used for all patients in this study, but there was variation in the duration of follow-up as well as the time from surgery to when each patient completed outcome questionnaires.
Conclusion
The internal splint technique acutely performed on type IV and V AC separations provided full return of range of motion and strength as compared with the contralateral side, as well as excellent patient-reported outcomes at midterm follow-up, with no reoperations. Additionally, radiographic reduction was maintained in the coronal and sagittal planes, and patients were satisfied with the appearance of their shoulders. The internal splint technique may be a treatment option for acute treatment of type IV and V AC separations.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A.L. has received educational support from Smith & Nephew, Arthrex, DJO, and Encore Medical. B.T.F. has received research support from Ceterix Orthopaedics and Zimmer-Biomet. A.L.Z. is a paid consultant for Stryker, receives research support from Zimmer-Biomet, and has received educational support from Arthrex.
Ethical approval for this study was obtained from the UCSF Human Research Protection Program Institutional Review Board (15-15788; reference 168852).