
Abstract
Background:
Obstacle course racing (OCR) has become a popular sport in recent years as it challenges participants’ mental and physical endurance through a combination of trail running and obstacles. There is currently only a limited amount of published work reporting injury types or rates at these events.
Purpose:
This study aims to build on the current literature, analyzing injury rates and patterns at OCR events.
Methods:
A secondary data analysis of deidentified medical charts from 33 OCR events in Canada from 2015 to 2017 was conducted. The scope of on-site care was first aid.
Study Design:
Descriptive epidemiology study.
Results:
A total of 1782 injuries occurred over 3 seasons from 73,366 participants, with an overall average injury rate of 2.4%; 1.0% (n = 17) of injuries required emergency medical services transport to a local emergency department, and the majority of these injuries were musculoskeletal in nature. The most common injuries treated were lacerations and musculoskeletal-related injuries; 93.9% of the injuries were able to be treated on site. These findings, in conjunction with the published literature, suggest that OCR medical teams should anticipate injury rates of up to 5.0% and a transportation rate of approximately 4.5% of those injuries to local emergency departments.
Conclusion:
The injury and transportation rates found in this study are congruent with the current literature and, most notably, they demonstrated a stable trend across a variety of course lengths (5-42 km ) and numbers of obstacles (≥20). While the majority of injuries may be treated on site, there is still a serious potential for life-threatening emergencies to occur.
Keywords
Over the past decade, obstacle course racing (OCR) has gained increased popularity in the extreme sport scene, creating a niche athletic field for those wanting an atypical racing experience. OCR has gained international attention, as seen by the increasing number of global participants, event types, diverse event locations, and television coverage. 2,14,20,24 With an estimated 5.3 million global participants in 2016 and an overall estimated revenue of US$323 million in North America alone in 2015, it is quickly becoming a flourishing sport. 19 Created on the foundations of military exercises, OCR events challenge participants’ mental and physical strength through a combination of trail running and obstacles. 18 The popularity of the sport has joined the likes of other multiple subcategories of extreme running, namely, adventure racing, obstacle courses, time-based competitive OCR, and mud runs. 16 While the purpose of these races is to challenge participants in a novel environment, these events have led to several recorded deaths internationally. 2,6,13,14,17,22 –24
As an emerging sport, OCR still lacks the medical research necessary to appropriately assess the unique risks posed by the rugged terrain and challenging obstacles. 3,4,9,14,24 The majority of OCR events are currently not officially regulated by governing bodies, and there are no established international or national standards for the medical provision of care at events. 8,16 The Fédération Internationale de Sports d’Obstacles has recently been formed to address these issues and is in the process of establishing international guidelines. 8 However, the nature of the sport and the lack of research into injury patterns specific to OCR makes this process difficult. 8
OCR events are generally outdoor events and are often held in a wilderness setting, subjecting the runners to a range of environmental factors, including temperature extremes, poisonous vegetation, animal encounters, adverse running conditions, and a multitude of different terrains on a single course. 5,11,12,14,18 With the combination of event intensity, unique obstacles, and varied environmental factors, OCR has the potential to create a variety of injuries in a range of severities unlike any other sport. 11,24
As the sport has grown, the literature has been slow to catch up. From 2009 onward, OCR studies have spanned multiple developed countries and have encompassed a range of OCR events. Currently, the published literature ranges from case studies to a review of 12 events. Study sizes have ranged from 5000 to 45,325 participants. 1,5,9,10,15,16 In Canada, Lund et al 16 encountered 1458 injuries over 6 Canadian OCR events, finding an injury rate of 3.74% and an emergency medical services (EMS) transport rate of 1.1%. Hawley et al 10 reported an injury rate of 1.2% and an EMS transport rate of 2% over 8 Canadian OCR events. Coleby and Thibeault-Rivard 5 reported the highest known EMS transport rate of 4.2% and the lowest injury rate of 0.4% after reviewing 12 Canadian Spartan Races. In Australia, Luke and Dutch 15 found that 2 Tough Mudder events resulted in an EMS transport rate of 0.4%, the lowest rate found in the literature. Agar et al 1 examined 4 United Kingdom Tough Guy OCR events with 5000 participants, reporting an injury rate of 2% and an EMS transport rate of 4%.
The findings of these studies have shown that despite event specifics, difficulty, distance, location, terrain, or environmental factors, the rate of injury has consistently been between 0.40% and 3.74%. 1,5,9,10,15,16 Similar rates were found for EMS transport, consisting of 0.13% to 4.2% of all injuries treated. 1,5,10,15,16 There is currently no consensus as to what the upper limit of injuries or hospital transfers is. Traditional road races (5K/10K and marathons) also have surprisingly little conclusively published data on injury rates/patterns, making a comparative analysis difficult to complete with confidence.
The purpose of this study was to contribute to the growing body of research evaluating participant injury rates at OCR events. With this information, the sport may be better equipped to anticipate and possibly mitigate participant risks.
Methods
Ethics approval for this secondary data analysis was obtained from the University of Windsor Research Ethics Board. Before the event, each participant signed a waiver form allowing their deidentified medical information to be used by third parties. Study researchers were a part of the event medical team leadership and had direct access to original medical charts.
Event and Participant Information
This study analyzed the injury rates from 33 OCR events held in Eastern Canada by Spartan Race between May 2015 and September 2017. There were 73,366 total participants over 3 race seasons, which comprised 12 events in 2015, 10 in 2016, and 11 in 2017. Spartan Race is a timed event that involves all-terrain running, often on a mountainous course, while completing a variety of strategically placed obstacles. 20 A variety of environmental conditions were encountered, including snow, thunderstorms, and extreme heat. The weather ranged from 5.8°C to 33.8°C between the hours of 8:00 AM and 8:00 PM. 7
Events varied in length, number of obstacles, and difficulty, and all variations were included in the data: 19 events were 5K races (5 km, ≥20 obstacles), 10 events were 10K races (10 km, ≥25 obstacles), and 4 events were 24K+ races (24-42 km, 35-60 obstacles). Multiple 24K+ events were often run simultaneously using the same course (24-km and 42-km events); thus, data were unable to be extracted for each specific event length. Average participant numbers per race were 2365 for 5K, 1878 for 10K, and 1579 for 24K+.
The events were mostly held at rural ski resorts close to major cities, and events were named after the closest major city and difficulty level (eg, Ottawa 5K). The minimum age to participate in the adult course is 15 years in Canada. 20 The race can begin as early at 8:00 AM and can end as late as 12:00 AM at certain events due to no formal finish time. The study population included all participants injured at the event who received medical care, regardless of age.
Youth events are also held, with age-appropriate course distances and designs (0.8-3.2 km, varying number of obstacles) for youth aged 4 to 14 years. Youth injury data were excluded from this study because of difficulties tracking the number of registered youth participants.
There are currently no OCR industry-specific guidelines that outline the provision of medical care. Thus, the level of medical care delivered at events was established based on the injury rates from previous years’ events and the extensive experience of the integrated medical staff hired by Spartan Race. Unlike similar OCR events that use established commercial medical teams, the team providing care at these events was formed by independently hired contractors for each race season as well as event-day volunteers recruited by the event organizer. Those providing medical care included first aiders, first responders, lifeguards, paramedics, and registered nurses. There were no physicians on site. Medical care provided at events included basic first aid, vital signs, glucometry, oxygen, immobilization of joints, automatic external defibrillation, symptom relief (ibuprofen, acetaminophen, and antibiotic ointment; administered at some events only), and spinal precautions. The local EMS was made aware of the events before they were held but was not on standby at events. EMS transfers to local hospitals were initiated through calling the local EMS dispatch center. A medical tent was located in a central area near the start and finish lines, and participants could present themselves at any time before, during, or after the race. First responders were also placed strategically around the course.
Data Collection
Patient data were collected from the event medical charts by the lead researcher (H.R.), who entered the data into a secure database for evaluation. Data analysis was performed using Excel (Microsoft). The data included chief complaint, location of treatment, treatment provided, and patient outcome. Total event participant numbers were extracted from official timing records, publicly available on the event website. 20,21 For the purpose of this study, a “participant” was defined as anyone who crossed the start line per race; if an athlete raced more than 1 event in a season, he or she would be counted as a new participant for each event.
Injuries and disposition were categorized according to the classifications provided on the medical charts. Injuries were divided into allergic reaction, cardiorespiratory, environmental, exertion, gastrointestinal, laceration, and musculoskeletal (MSK). Laceration injuries encompassed lacerations, burns, and abrasions. MSK injuries were classified as damage to the bone or muscle and contusions. Because of the limited medical scope and lack of on-site diagnostic equipment, no formal MSK diagnoses could be made. A detailed breakdown of the specific body parts and the associated muscles most commonly injured were analyzed. The “upper arm” encompassed the shoulder and humerus; “lower arm” consisted of the radius and ulna; “torso” included the abdomen, chest, and ribs; “upper leg” was composed solely of the femur; and “lower leg” included the tibia, fibula, and knee. The “unknown” category was used for MSK injuries in which there was no descriptive information provided on the medical chart.
Exertional injuries encompassed diabetic emergencies, shortness of breath, dehydration, and electrolyte-related illnesses. Environmental illnesses pertained to weather- or terrain-induced injuries such as heat stroke, hypothermia, or poisonous plants. Minor injuries that required a single bandage or less were excluded from this study.
Disposition was divided into 3 categories: “treatment on site” if the patient returned to the event, “self-evacuation to emergency department (ED)” if the patient elected and was deemed medically stable enough to drive himself or herself or be transported by a friend or family member to a local ED, or “EMS transport to ED” if a local ambulance had to be called. The location of treatment was documented as either in the clinic or in the field, while patients treated in both locations were recorded as clinic patients.
Results
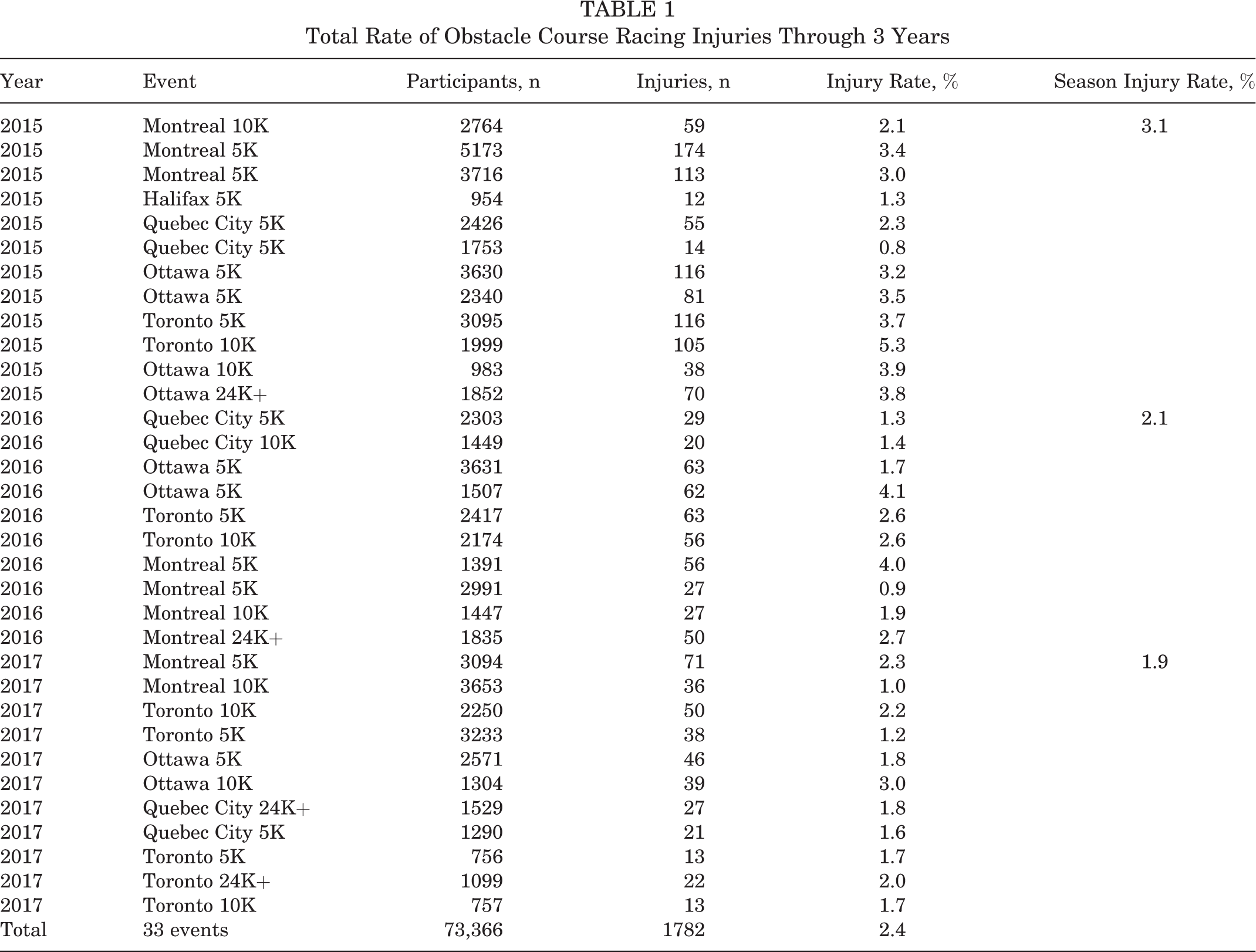
Over 3 seasons, a total of 1782 injuries arose from 73,366 participants, resulting in an average injury rate of 2.4% (Table 1), with a range of 0.8% to 5.3% for each single event. The 5K races had an average injury rate of 2.3%, the 10K races had an average injury rate of 2.5%, and the 24K+ events had an average injury rate of 2.6%. The difference in injury rates per race was found to be nonsignificant (P = .39, P > .05 ) through a chi-square test, demonstrating that race length may not significantly correlate with injury rates. These injuries were treated on site in 93.9% (n = 1674) of instances, with only 17 participants (1.0% of injuries) requiring EMS transport (Table 2).
Total Rate of Obstacle Course Racing Injuries Through 3 Years
Patient Disposition a
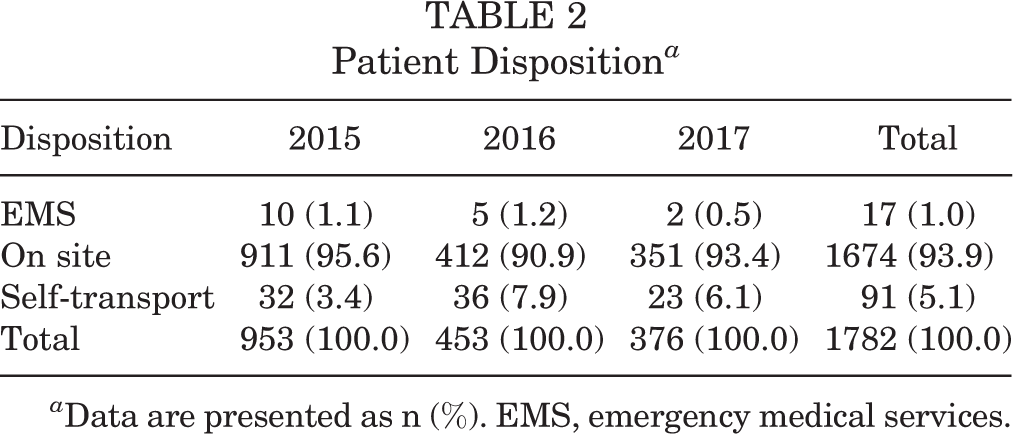
a Data are presented as n (%). EMS, emergency medical services.
Patients were most often transported by EMS for fractures or dislocations (n = 10). Bones/joints involved included the ankle (n = 2), forearm (n = 1), knee (n = 1), shoulder (n = 1), spine (n = 2), tibia (n = 1), and unspecified (n = 2). The only laceration requiring transport by EMS was for facial trauma. Other reasons for EMS transport were severe allergic reaction (n = 2), dehydration (n = 1), and heat stroke (n = 1). Two patients were also transported for “cardiorespiratory” illnesses that were diagnosed in a hospital as exertional hyponatremia (n = 1) and myocardial infarction (n = 1).
The overwhelming majority of injuries (70.5%, n = 1236) were able to be treated on the race course by first responders. Lacerations were the most common injury, accounting for 59.0%, followed by MSK injuries at 33.4% (Table 3). The most prevalent locations of an MSK injury, within the body sections outlined in Table 4, were the ankle (n = 238), knee (n = 118), shoulder (n = 36), and wrist (n = 24).
Chief Complaint for Patients Presenting to the Medical Team a

a Data are presented as n (%). MSK, musculoskeletal.
Musculoskeletal Injury by Body Section

Discussion
This study examined patient data encompassing 3 race seasons (33 events; 73,366 participants), at venues across 3 Canadian provinces, hosted by an individual OCR company from 2015 to 2017, making it one of the largest studies of OCR injury rates conducted to date.
This study found that the average injury rate of approximately 2.4% was stable, regardless of the event length or number of obstacles. These results are congruent with previously reported results internationally, which demonstrate rates of less than 5.0% (0.4%-3.74%), regardless of event specifics or country of origin. 1,5,9,10,15,16 The EMS transport rate of 1.0% found in this study also aligns with currently published findings, which have demonstrated that less than 4.5% (0.13%-4.2%) of injures require an EMS transfer off site. 1,5,10,15,16 In summary, these findings, in collaboration with the previous studies cited, may indicate a stable trend in injury rates across the sport; up to 5.0% of participants will suffer an injury during OCR events, and less than 4.5% of all sustained injuries will require ambulance transport to an ED.
The results of this study also demonstrate that a considerable number of injuries can effectively be treated in the field, not requiring patients to present to the medical clinic or leave the course. It was beyond the scope of the data collected to evaluate how many of these participants continued the event (vs self-selected to stop the race after treatment); however, field treatment of these injuries did mitigate the need for the patient to present to the medical tent for further evaluation. Many current OCR medical providers do strategically place medical assets around courses, and based on the study results, this practice should be continued and encouraged, as it provides a quicker response time for injured participants.
Lacerations and MSK injuries were the most common injuries seen. They were minor in nature and were successfully treated on site in nearly all cases. These injury types were likely seen because of the inherent features of OCR events, which require participants to run, crawl, climb, and roll across uneven, natural terrain. 18,20 Participants are also often required to carry and handle metal and wooden objects to complete obstacles, which likely increases the risks for lacerations. A common minor injury seen at events is “rope burn” to the hands and lower legs, most often caused by manipulating wet, muddy ropes. Injury prevention methods may include wearing gloves, wearing garments that cover the lower body, and staying hydrated to help maintain muscle strength. Further research should explore injury types relative to obstacles to examine the risk that each obstacle poses to the participants.
Environmental and exertional injuries were found to be infrequent, which may be attributed to the course design, hydration stations around the course, or general participant preparation (ie, hydration packs, electrolyte gel, food, etc). OCR events are unique in design: continual elevation and terrain changes, with obstacles methodically placed around the course. This may affect the running tempo of the participants, forcing them to run slower and take more frequent breaks, which may in turn play a role in decreasing environmental and exertional injury rates. It is important to note that environmental injuries are a product of the event location; for instance, northern climates may produce different injuries compared with southern climates because of differences in temperature, elevation, or humidity.
Serious injuries requiring an EMS response only occurred for a small number of participants over the 33 events. MSK injuries were the most common reason for EMS transport, again likely because of the prevalence of MSK injuries at OCR events and the difficulty associated with treating severe MSK injuries in the field. MSK injuries also present with significant pain for the injured participant, a symptom that is difficult for a first response team to manage without pharmacological support. EMS was also required for potentially life-threatening medical illnesses on multiple occasions: for allergic reactions, cardiorespiratory illnesses, and environmental exposures. These illnesses, although rare across the 33 events, are difficult for a field medical team to manage without advanced medical support and access to more advanced evaluation tools, such as electrolyte testing or electrocardiographic capabilities. As the sport continues to grow, OCR events and governing bodies will need to evaluate the risk of rare serious injuries with the potential benefits of having more expensive advanced medical care on site.
Study Limitations and Future Areas of Research
Study limitations included the potential for documentation errors due to provider-specific discretion, such as selecting “cardiorespiratory illness” versus “environmental.” While this did not affect the overall rate of injuries or disposition of participants, it may affect the medical preparation for anticipated illnesses/injuries at future events. This study also lacked demographic information on participants/patients, making a subanalysis of injury rates by sex, fitness level, and age, among other variables, beyond our scope. An evaluation of youth injury patterns was not possible, as youth participant numbers were not accurately tracked by the event organizers.
This study did not include participants who may have self-presented to local medical services without being seen by the event medical team. Future studies may consider reviewing charts at local area hospitals to establish information regarding the number of participants who bypass event medical teams. Future research is also needed to understand the risks of specific obstacles and to evaluate and establish the level of medical care that is required on site at OCR events.
Conclusion
The results of this study indicate an injury rate at OCR events of 2.4% and an EMS transport rate of 1.0% of all injuries. These results were similar regardless of event specifics (length, terrain, number of obstacles) or event location. Lacerations and MSK injuries comprised the majority of injuries; however, nearly all were minor in nature. Although many injuries incurred were treated in the field by an experienced first responder, there were still a considerable number of injured participants who required either self-transport or EMS transport to a local hospital for advanced-level care and further evaluation.
Footnotes
Acknowledgment
The authors thank and acknowledge the members of the Spartan Race Eastern Canada Medical Team for their continued dedication and exceptional patient care during the 2015-2017 seasons. They also thank both St Clair College and the University of Windsor for their support in this project.
One or more of the authors has provided the following potential conflict of interest or source of funding: H.R. was employed by Spartan Race as a course medic and director of medical operations. J.C. was employed by Spartan Race as medical director and serves as the deputy chair for the Medical Commission of the Fédération Internationale de Sports d’Obstacles. Her spouse was also employed by Spartan Race as director of medical operations.
Ethical approval for this study was obtained from the University of Windsor Research Ethics Board (No. 34300).