
Abstract
Background:
Surgical repair of an Achilles tendon rupture has been shown to decrease rerupture rates. However, surgery also increases the risk of complications, including infection.
Purpose:
To determine the risk factors for infection and rerupture after primary repair of Achilles tendon ruptures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was performed on 423 patients who underwent operative treatment of Achilles tendon ruptures between the years 2008 and 2014. The primary outcome of interest was the total rate of infection, and the secondary outcome of interest was the incidence of rerupture within 2 years of operation.
Results:
A total of 423 patients were analyzed, with a mean age of 46 years (range, 16-83 years) and a mean body mass index of 31.4 kg/m2 (range, 17-55 kg/m2). The overall infection rate was 2.8%, and the rerupture rate was 1%. The median time between surgery and superficial surgical site infection was 30 days, and the median time between surgery and rerupture was 38 days. Longer tourniquet times (100.3 ± 34.7 minutes vs 69.9 ± 21.4 minutes; P = .04) and greater estimated blood loss (15.0 ± 9.1 mL vs 5.1 ± 12.0 mL; P = .01) were associated with an increased rate of deep surgical site infections. Patients who had longer operation and tourniquet times trended toward higher rerupture rates (P = .06 and .08, respectively). When compared with nonsmokers, current and previous smokers had an increased incidence of superficial or deep surgical site infections (6.25% vs 1.42%; P = .02). Age, sex, race, body mass index, alcohol use, diabetes, past steroid injections, and mechanism of injury did not contribute to complication rates.
Conclusion:
Achilles tendon repairs were associated with a low risk of infection and rerupture. Patients with longer tourniquet times, higher estimated blood loss, and a history of smoking were at increased risk for surgical site infections. Patients with longer operative times had increased rates of rerupture.
The Achilles tendon is the largest and strongest tendon in the body; however, it is subject to significant stresses during athletic activity—up to 12.5 times body weight during running. 17 As a result of these stresses, Achilles tendon ruptures account for approximately 20% of all large tendon injuries, and the incidence of ruptures has recently increased. 12 Treatment with primary Achilles tendon repair is often associated with good outcomes, with decreased rerupture rates and increased power as compared with nonoperative treatment. 8
Although open repair of the Achilles tendon has been shown to reduce the risk of rerupture as compared with nonoperative treatment, it is associated with a significantly higher risk of wound infections. 1 A meta-analysis by Wilkins and Bisson 32 corroborated these findings and demonstrated that operative management of acute Achilles tendon ruptures significantly reduces the risk of reruptures and increases the incidence of infections when compared with nonoperative management. Previous studies have cited the thin soft tissue envelope, tenuous blood supply, and large resident microbial environment as contributing to the high rate of infection in ankle surgery. 25 Because of this risk, some have recommended nonoperative treatment and have been less aggressive with surgical treatment. This approach, however, can exclude the benefit of surgical treatment, including lower rerupture rates and increased power, to the potential detriment of the active population. 15
While complication rates of Achilles tendon repairs are low, the implications of complications are devastating. Traditional risk factors that lead to infection and rerupture include corticosteroid use, smoking, diabetes, and delay in treatment. 26 While many patient factors contributing to poor outcomes are nonmodifiable, there are factors that surgeons can control, although the data are limited regarding surgeon-controlled factors and concomitant patient factors as they relate to complications of Achilles tendon repair. The purpose of this study was to determine risk factors for infection and rerupture after primary repair of Achilles tendon ruptures. The primary outcome of interest was the rate of infection (superficial and deep) within 2 years of surgery. Secondary outcomes of interest included the rate of rerupture within 2 years of surgery as well as complications that were correlated with patient- and surgery-specific factors.
Methods
After institutional review board approval was obtained, a retrospective review was performed of 423 patients who underwent primary operative repair of Achilles tendon rupture at our institution between January 2008 and June 2014. Patients were identified by searching with Current Procedural Terminology code 27650 (Achilles tendon repair) from 2 academically affiliated hospitals: a large urban tertiary care center and a suburban community hospital in a large metropolitan area. All operations were performed as open procedures with an end-to-end repair. Five patients required augmentation with a graft.
After patients were identified, a chart review was performed. Recorded demographic data for each patient included body mass index, age, sex, and race. Injury data were collected to determine the mechanism of injury, which was classified by sport or as due to walking, stairs, fall, or other. Patient risk factors were also recorded, such as previous steroid injection, smoking status, alcohol use, and diabetes mellitus. Ex-smokers and smokers were analyzed as 1 cohort, owing to literature suggesting only partial reversal of smoking-related pathology upon quitting. 5,19,22 Surgical data were collected and included procedure and side, type of skin preparation used, estimated blood loss, tourniquet time, and operative time. Patients who were not at least 2 years from the date of surgery were not included in the analysis, and all complications were noted.
Postoperatively, all patients followed the same standardized institutional rehabilitation protocol. Patients were instructed to be nonweightbearing for the first 2 weeks. Partial weightbearing in an elevated boot commenced during weeks 2 to 6, and patients progressed to full weightbearing by 6 weeks. Patients participated in active dorsiflexion and passive plantar flexion during this time. After 6 weeks, patients continued work on proprioceptive and range of motion exercises. Functional exercises began during weeks 12 to 16, with an emphasis on isometric exercises. Most patients were discharged from physical therapy by 6 months postoperatively, after demonstrating normal gait patterns and performing functional tests within 85% of the uninvolved leg (single-leg balance reach, hop for distance, and isokinetic strength).
Statistical Analysis
All continuous data are described as means with ranges or SDs as appropriate, while all categorical data are described as counts and column percentages. Risk factors were assessed with Wilcoxon rank-sum and Fisher exact tests. Statistical significance was set at P < .05, and all analyses were performed with SAS (v 9.4; SAS Institute Inc).
Results
A total of 423 patients were included, with a mean age of 46 years (range, 16-83 years) and a mean body mass index of 31.4 kg/m2 (range, 17-55 kg/m2) (Table 1). A greater number of patients requiring Achilles tendon repair were ≤40 years old versus >40 years old (66.5% vs 33.5%). The cohort had a mean operative time of 79.3 minutes (range, 35-281 minutes), tourniquet time of 70.2 minutes (range, 23-170 minutes), and estimated blood loss of 5.2 mL (range, 0-150 mL). Basketball was the most common mechanism of injury, followed by tennis. Thirty-three percent of patients were active or former smokers; 62% reported alcohol use; 12% had a medical history of diabetes mellitus; and 3% had a prior steroid injection.
Demographic Data for Patients Undergoing Surgical Reconstruction of Achilles Tendon (N = 423) a

a Because of incomplete reporting, not all subgroups represent the entire cohort.
The overall infection rate was 2.8% (12 of 423), and the rerupture rate was 1% (3 of 423). The deep surgical site infection rate was 1% (4 of 423), and the superficial surgical site infection rate was 2% (10 of 423). Two patients had both superficial and deep infections. The median time between surgery and superficial surgical site infection was 30.0 days, and the mean time between surgery and rerupture was 38.0 days. When evaluating patient and surgical risk factors, we found that longer tourniquet times (100.3 ± 34.7 minutes vs 69.9 ± 21.4 minutes, P = .04) and higher estimated blood loss (15.0 ± 9.1 mL vs 5.1 ± 12.0 mL, P = .01) were associated with an increase in deep surgical site infections (Table 2). Patients who had longer operative times (101.7 ± 19.2 minutes vs 79.1 ± 28.5 minutes, P = .06) and longer tourniquet times (93.3 ± 23.0 minutes vs 70.0 ± 21.7 minutes, P = .08) had a higher rate of reruptures; however, this was not statistically significant (Table 3). When compared with nonsmokers, current and previous smokers had an increased incidence of superficial surgical site infections (6.3% vs 1.4%, P = .02).
Superficial and Deep Surgical Site Infection in Achilles Tendon Repair a

a Values are presented as mean ± SD or n (%). Bolded values indicate statistically significant differences between patients with and without an infection.
Rerupture After Achilles Tendon Repair a
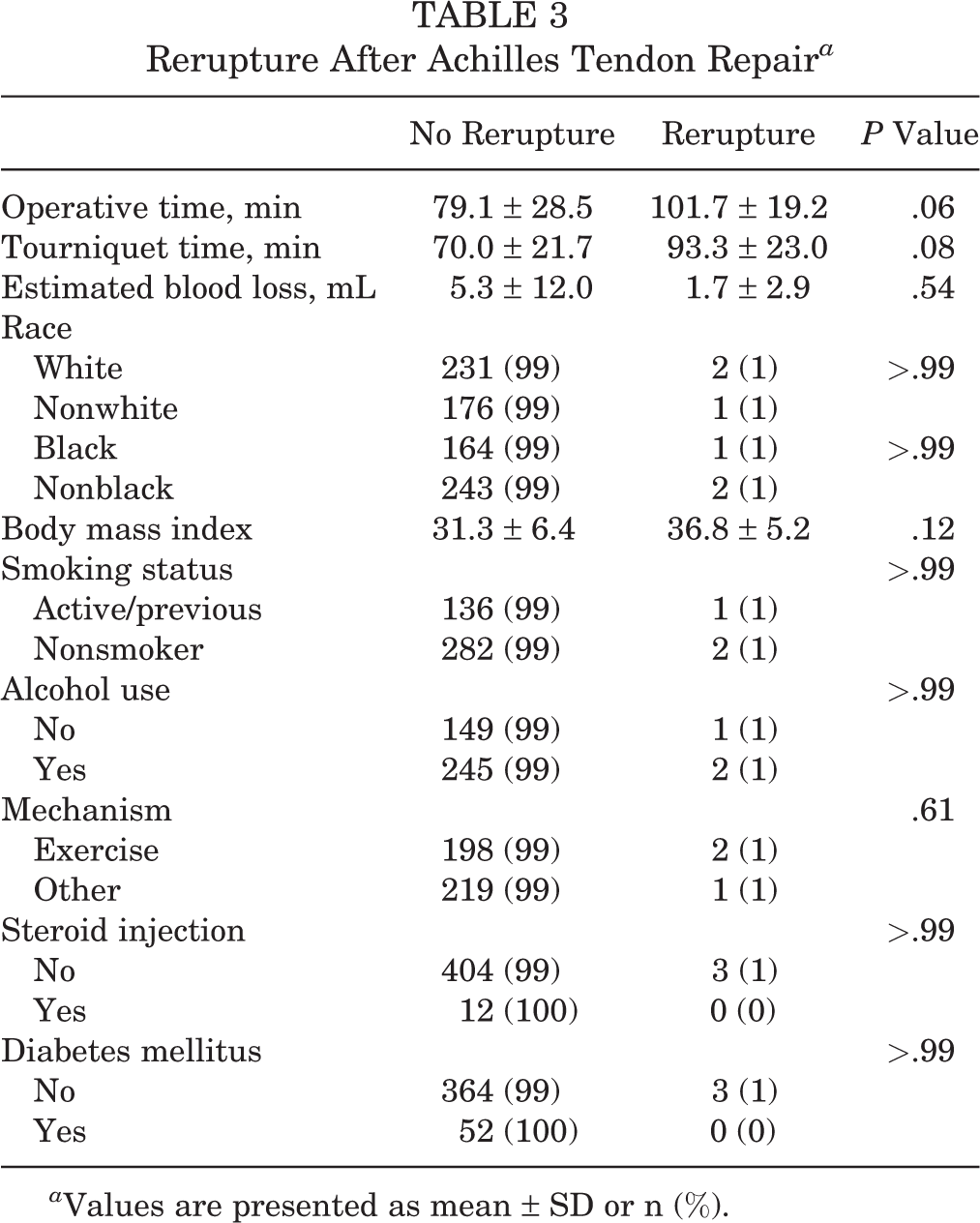
a Values are presented as mean ± SD or n (%).
In our study, age, sex, race, body mass index, alcohol use, diabetes, past steroid injections, and mechanism of injury did not have any effect on the incidence of surgical site infections or rerupture.
Discussion
Achilles tendon ruptures are a source of significant functional impairment, especially for an athlete. Current research shows that athletes in professional basketball, football, and baseball experience a significant decrease in games played, as well as a decrease in performance, 1 season after surgery as compared with the preinjury season. 20,21 Athletes with an Achilles tendon injury also have a high rate of dropout from sport in subsequent seasons. While many patient factors that contribute to poor outcomes are nonmodifiable, it is imperative that surgeons are mindful of factors that they can control. Our study confirms that Achilles tendon repairs are associated with a low overall risk of infection and rerupture. However, patients with longer tourniquet times, higher blood loss, and a history of smoking were found to be at increased risk for surgical site infections. Patients with longer tourniquet and operative times also had an increased rate of rerupture.
The effect of length of surgery and patient smoking on wound healing was previously evaluated in the literature. 6,7,10,23,24,27,29 Wiewiorski et al 30 evaluated 290 elective foot and ankle procedures and found an increase in postoperative wound-healing complications with higher tourniquet times (odds ratio = 7.02) and smoking (odds ratio = 48.77). Using a registry of 56,216 total knee arthroplasties, Namba et al 24 found a nearly 9% increased risk of infection per 15-minute increase in surgical time. Our study found that patients with longer operative times and tourniquet times and a higher estimated blood loss had increased rates of deep surgical site infection. Despite the fact that a tourniquet may portend better surgical exposure, it is thought that the tissue hypoxia and inflammation caused by the tourniquet predispose patients to surgical site infections. 28,31 Increased rates of estimated blood loss are thought to increase the deep surgical site infection rate because the Achilles tendon is natively in a precarious hypovascular state and is sensitive to any variation in blood and nutrient delivery. It is thought that an increase in estimated blood loss may create aberrations in wound healing and may increase tissue degeneration, leading to infection. 9,13 Furthermore, in animal models, frank acute anemia during a procedure has been shown to decrease the healing potential of tissues. 4,16 These findings suggest that the duration of an operation and host susceptibility contribute to infection rates.
Patients in our study who were current or previous smokers had a 40% increased rate of superficial surgical site infections. Smoking is known to increase tissue hypoxia and inflammation through vascular vasospasm and a global increase in systemic inflammation, and it has been shown to increase the risk of infection in tendon repair by up to 30%. 2,3,11,22
Current literature reports an approximate 3.6% rerupture rate after repair of a primary ruptured Achilles tendon. Studies on modifiable risk factors that contribute to rerupture after Achilles tendon repairs are sparse; however, in a study evaluating 1000 consecutive rotator cuff repairs, Le et al 18 found that increased operative time had a statistically significant correlation with retear of the rotator cuff tendon. In our study, 1% of patients had a rerupture. The patients in our study with longer tourniquet or operative times experienced a trend toward an increased rate of rerupture. Longer operative and tourniquet times are likely surrogate measurements for the difficulty of the case and tenuous repair, which may have implications on the ability of the tendon to heal through intrinsic methods (inflammatory cells and fibroblasts) and extrinsic methods (migration of cells), increasing the risk of future rerupture. 33 Alternatively, the longer operative and tourniquet times may represent inexperienced primary surgeons performing the repairs.
This study has many potential limitations. The retrospective nature of the study and inclusion of multiple surgeons did not allow for standardization of the repair method. Patients who were diagnosed with a complication at another health care system could not be accounted for. However, we limited our data collection to only patients who were at least 2 years from the date of surgery, in an attempt to ensure collection of pertinent information. In addition, the number of study patients who experienced a complication was low, thereby limiting our sample size in evaluating risks for complications. However, our rates of infection and rerupture are similar to rates reported in the current literature. 14 We suspect that more severe injuries would require greater blood loss, operative times, and tourniquet times and, subsequently, more surgical site infections and reruptures; however, the injury severity was not consistently documented in the patient charts. Last, a multivariate analysis was not feasible; that is, when based on a small number of events (<10), a regression analysis is simply not an effective measure. Strengths of the study include a large cohort of patients who underwent Achilles repair at a single institution. This allowed consistency of treatment protocols as well as postoperative therapy protocols.
Conclusion
Our study revealed Achilles tendon repairs to be associated with a low risk of infection and rerupture. Patients with longer tourniquet times, higher estimated blood loss, and a history of smoking were at increased risk for surgical site infections. Patients with longer operative times also had increased rates of reruptures. When repairing Achilles tendon ruptures, surgeons should be mindful of patient and surgeon factors to decrease the rate of complications.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: T.R.J. receives education support from DePuy Synthes. F.Z. has received hospitality payments from Wright Medical. V.M. has received hospitality payments from Stryker and Pinnacle and educational support from Arthrex and Pinnacle.
Ethical approval for this study was obtained from Henry Ford Health System.