
Abstract
Background:
Recurrent patellar instability is commonly treated with medial patellofemoral ligament reconstruction (MPFLR), and the use of allograft in anterior cruciate ligament reconstructions has demonstrated inferior outcomes.
Purpose:
To compare the outcomes of allografts versus autografts in adolescent MPFLR for patellar instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective chart review was completed on patients younger than 18 years who underwent MPFLR for recurrent instability after failed nonoperative management over an 8-year period with a minimum 2-year follow-up. Patients were divided into autograft or allograft hamstring cohorts for comparison. Primary outcome measures were return to normal activity, incidence of redislocation/subluxation, pain, stiffness, other complications, and Kujala scores. Statistical analysis using unpaired t tests was performed, with an alpha value set at P < .05.
Results:
After criteria were applied, 59 adolescents (36 allograft, 23 autograft; 38 girls, 21 boys) with a mean ± SD age of 15.2 ± 1.7 years and a mean follow-up of 4.1 ± 1.9 years (allograft, 3.3 ± 1.1 years; autograft, 5.7 ± 2.1 years; P ≤ .001) were included. Seven patients had concurrent osteotomies (3 allograft, 4 autograft), 11 patients had concurrent loose body removals (5 allograft, 6 autograft), and 9 patients had concurrent lateral release (7 allograft, 2 autograft). Between groups, no significant difference was found in change between preoperative and most recent follow-up (mean, 1.2 ± 2.1) or rate of return to sports (mean, 73.3%). In total, 9 surgeries failed (3 allograft, 6 autograft). For the surviving grafts, a statistical difference in mean Kujala scores at final follow-up was noted (allograft, 92.7; autograft, 97.4; P = .02).
Conclusion:
We identified no significant differences in return to activity, pain score changes, and incidences of failure between patients undergoing MPFLR with allograft versus autograft. Although teenagers with surviving autograft MPFLR reported statistically higher Kujala scores, the mean score difference of 5 points was not clinically significant. It appears that using allograft tendon instead of autograft tissue for MPFLR in this teenage population does not adversely affect long-term outcomes.
The overall annual incidence of lateral patellar dislocations in the United States is 5.8 per 100,000, 5 but the incidence peaks during adolescence, with a rate of 29 per 100,000. While an acute lateral patellar dislocation could be a symptom of generalized joint laxity, the most prevalent finding of recurrent patellar instability is a disruption of the medial patellofemoral ligament (MPFL). 10 Over the past decade, an MPFL reconstruction (MPFLR) to achieve stability has increased in popularity.
While most research on patellar instability has focused on various reconstructive techniques and outcomes of these procedures, longitudinal studies have not been conducted to compare outcomes of allografts and autografts in MPFLRs. 1,4,10,12 Most studies merely comment on the merits of one choice of graft or the other, instead of comparing the efficacies of the two simultaneously. 4,12 While past study in this young population has clearly demonstrated inferior results with allograft in the reconstruction of the anterior cruciate ligament (including hybrid constructs), this has not stopped the use of allografts in MPFLRs. 9,14 Although patients have shown excellent outcomes in MPFLR, it is still unclear whether using an allograft or an autograft presents a more favorable outcome. The purpose of the current study was to compare the outcomes in adolescent patients with recurrent patellar instability of MPFLRs that used either allograft or autograft hamstring tendons. Our hypothesis was that there would be no difference in the outcomes between the allograft and autograft MPFLRs, particularly concerning graft failure and recurrent instability events.
Methods
A retrospective comparative study was performed on adolescent patients with recurrent patellar instability managed with an MPFLR who underwent surgery by a single surgeon (E.W.E.) between August 2006 and November 2014. Criteria for enrollment included patients younger than 18 years at the time of surgery and a minimum of 2-year clinical or telephone follow-up. All patients had attempted nonoperative management that typically included a short duration (∼4 weeks) of immobilization and subsequent physical therapy with a focus on quadriceps, hip external rotation, and core strength. In cases where a chondral or osteochondral loose body was noted, surgery was performed more expeditiously. Exclusion criteria included patients with a neuromuscular syndrome or collagen disorder that may affect healing or normal joint mechanics as well as patients who were initially treated at an outside institution. Also, if the final outcome could not be determined at the time of study and patients had less than 2 years of follow-up, they were then excluded from analysis.
Demographic, injury, and surgical data were collected from the patients’ charts, including date of birth, sex, date of initial injury, concurrent injuries, date of surgery, type of surgery (reconstruction technique), concurrent procedures, graft choice, and follow-up dates. Primary outcome measures included patient satisfaction, pain score (0-10), Kujala score, recurrent instability, return to normal activity, and other complications. Final Kujala and pain scores were not collected from patients with graft retears (n = 9), so as not to confound the statistical analysis. Instead, these patients’ surgeries were considered failures, as defined by a subsequent dislocation.
The surgical approach was based on a standardized treatment algorithm. In skeletally mature patients with a preoperative tibial tubercle–trochlear groove (TT-TG) distance of greater than 20 mm, a tibial tubercle transfer was performed with a goal of moving the tubercle medially and slightly anterior to correct the TT-TG to a measurement of 10 mm. The tubercle was not distalized in this cohort of patients. The next step in the algorithm was a diagnostic arthroscopy. If free osteochondral fragments were discovered, then they were removed or fixed as necessary. The patellar station and mobility were then assessed arthroscopically. If the patella could not be centralized on the trochlea without significant tilt, then a lateral release was performed arthroscopically. At this point in the procedure, the knee was drained of excess fluid and the MPFLR was performed.
The patient and his or her family made the choice between autograft and allograft after the preoperative surgical discussion concerning risks and benefits. Over the study duration, more families tended to favor allograft due to predictability of graft size and because allograft entails one less incision for hamstring harvest. This inclination then favored future patients choosing allograft, as the response to the query, “What do other people choose?” tended to shift the response further and further toward allograft.
If an allograft tendon was to be used, it was opened at the start of the case, so that the graft would have time to thaw in room temperature lactated Ringer’s solution. All grafts were nonirradiated hamstring tendons (either gracilis or semitendinosus) with a desired diameter of 4- to 4.5-mm single and 5- to 5.5-mm doubled over. If an autograft tendon was to be used, it was then harvested either through the tibial tubercle osteotomy incision (if present) or through a separate incision centered over the pes anserine. The gracilis was always the autograft used. The ends of the graft were secured through use of a No. 2 braided nonabsorbable suture.
During the study period, the surgeon’s technique evolved with respect to the fixation approach on the patella. Initially, the surgical technique involved fixation of the doubled-over side of the graft into the femur via an interference screw placed at the anatomic origin of the MPFL and its isometric point. The graft tails were then shuttled through the space between the second and third medial retinacular layers before being secured to the patella via 2 suture anchors that had been placed into a trough created within the superomedial edge of the patella. The patella was held in a central position on the trochlea with the knee bent at 30° as the graft was sutured into position, so as not to overconstrain the patellofemoral joint, as per a previously published technique. 3 Later during the study period, the technique evolved to interference screw fixation on the patella as well. In these cases, the single ends were fixed to the patella first and then the graft was shuttled through the retinacular layers and subsequently fixed at 30° on the femur. Care was once again taken to confirm that fixation on the femur was at the isometric point and that the patella was merely centralized on the trochlea and not overconstrained. The postoperative course, which did not change throughout the study period, included a range-of-motion brace locked at 10° until the first postoperative visit. Subsequently, full range of motion was allowed with physical therapy, and activity was advanced to full strength and agility; release to sports activity occurred between 3 and 6 months depending on individualized progression.
The entire patient cohort was from a single surgeon’s practice, and the graft choice for reconstruction was made with parental input after informed consent. The group was divided into 2 cohorts, allograft and autograft, for purposes of statistical comparison. Differences between the allograft and autograft group were evaluated with analysis of variance (ANOVA) for continuous variables or chi-square test for categorical variables. All continuous data were checked for normality and homogeneity of variances prior to application of the parametric ANOVA test. If either of these assumptions was violated, the nonparametric Mann-Whitney U test was used. Spearman rho correlation was performed to evaluate for linear relationship between Kujala score and time since surgery. All statistics were performed with SPSS (IBM SPSS Statistics for Windows, version 24.0), and alpha was set at P < .05 to declare significance.
Results
After the inclusion and exclusion criteria were applied in 108 adolescents, there remained 59 patients (36 allograft, 23 autograft; 38 girls, 21 boys) with a mean ± SD age of 15.2 ± 1.7 years at the time of surgery and a mean follow-up of 4.1 ± 1.9 years: 3.3 ± 1.1 years for allograft and 5.7 ± 2.1 years for autograft (P < .001) (Table 1). The various surgical techniques and concurrent procedures are listed in Table 2. A statistically significant between-group difference was seen in the type of patellar fixation used. All of the allografts versus only 39% of the autografts were fixed with interference screws.
Descriptive Statistics of Patients With Respect to Graft Type (Allograft vs Autograft) a
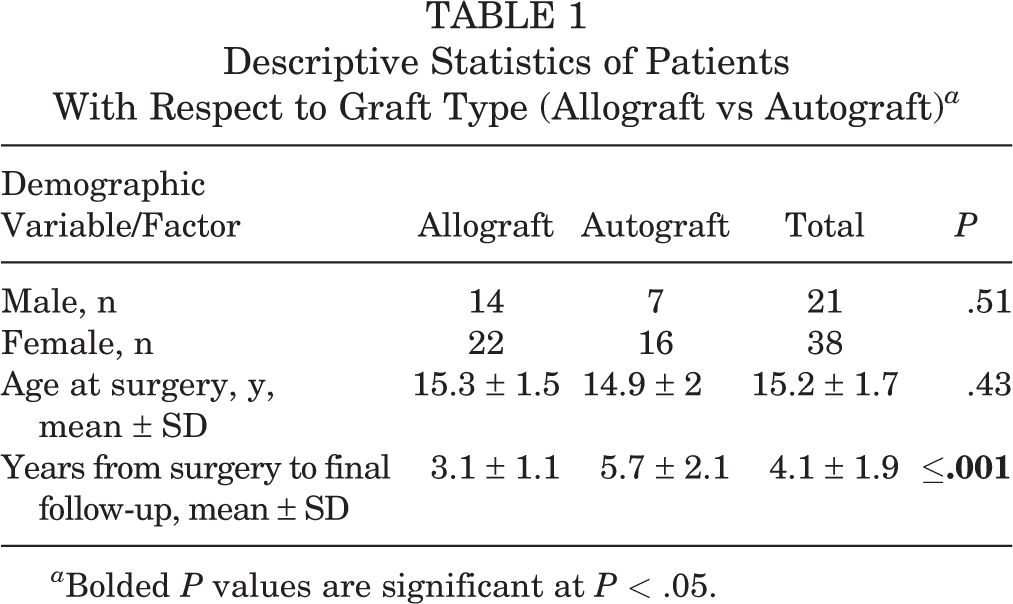
a Bolded P values are significant at P < .05.
Surgical Fixations and Concurrent Procedures of Medial Patellofemoral Ligament Reconstructions a
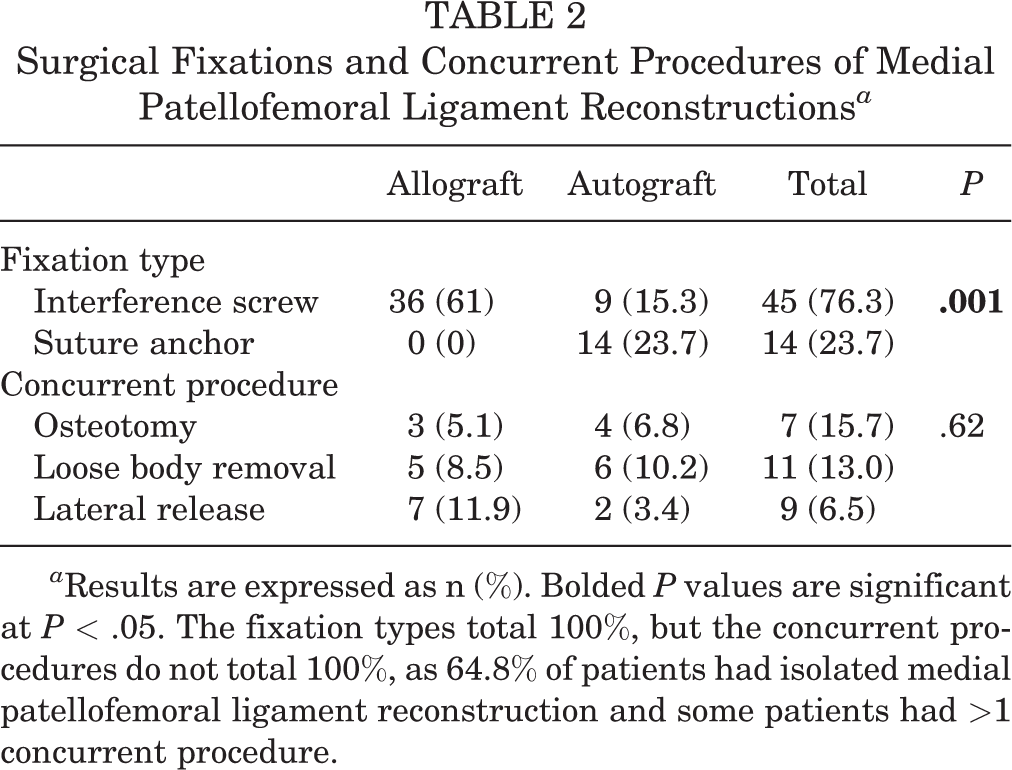
a Results are expressed as n (%). Bolded P values are significant at P < .05. The fixation types total 100%, but the concurrent procedures do not total 100%, as 64.8% of patients had isolated medial patellofemoral ligament reconstruction and some patients had >1 concurrent procedure.
When the allograft and autograft cohorts were compared, no significant difference was found in pain score improvements from preoperative to most recent follow-up (mean, 1.2 ± 2.1; P = 1.2) (Table 3). Only 45 of the 59 patients participated in high-intensity sports before their injury; therefore, only these 45 patients were used to compare the rate of return to sports, and no significant difference was found between the cohorts (73.3% returned; P = .47) (Table 4).
Kujala and Longitudinal Pain Scores With Respect to Graft Type

a Results are expressed as mean ± SD. Bolded values are significant at P < .05. Final Kujala and pain scores were not collected from patients with graft retears (n = 9).
Return-to-Sport and Failure Findings With Respect to Graft Type a
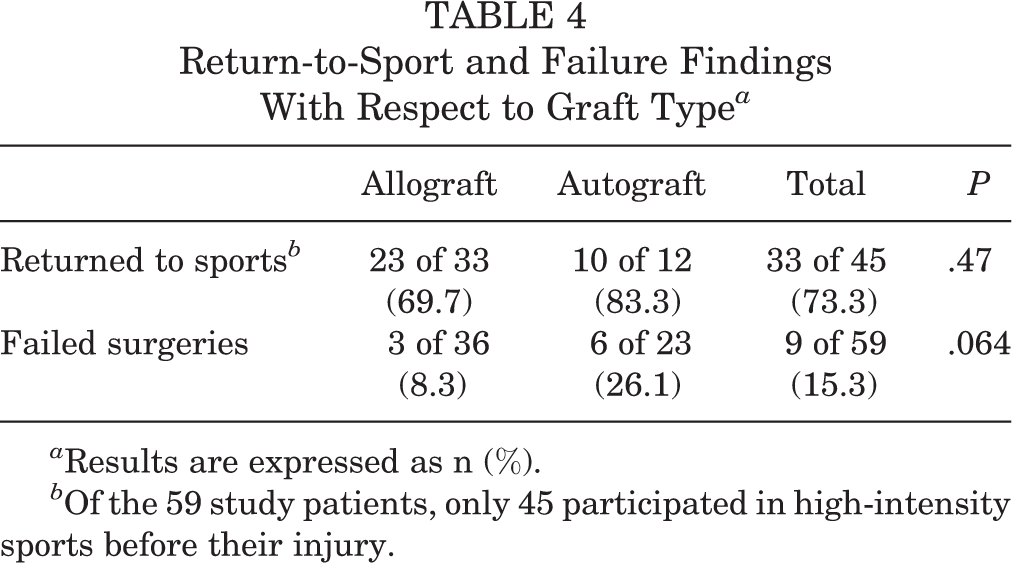
a Results are expressed as n (%).
b Of the 59 study patients, only 45 participated in high-intensity sports before their injury.
In total, 9 surgeries failed: 3 allograft and 6 autograft (P = .064) (Table 4). For the surviving grafts, a statistical difference in mean Kujala scores was noted at final follow-up: 92.7 (allograft) and 97.4 (autograft) (P = .02) (Table 3). Spearman rho analysis showed no linear correlation between duration of follow-up and the Kujala score (rho = 0.005, P = .97). We further analyzed outcomes based on fixation type. We found no difference in Kujala scores between the suture anchors (mean score, 97.5) and the interference screw (mean score, 93.5) constructs (P = .151). No significant difference was found in current pain scores between suture anchors (mean, 0.14) and interference screw (mean, 0; P = .977). The difference in return-to-sport rate (suture anchor, 87.5%; interference screw, 70%; P = .32) and failure rate (suture anchor, 29%; interference screw, 11%; P = .19) did not reach statistical significance. No fractures or reoperations secondary to infection or stiffness were recorded in this entire cohort.
Discussion
Given that a significant majority of patients with patellar instability are adolescents, 5 it is important to evaluate the factors that play a role in this pathologic condition by age. Recurrent patellar instability in adolescents can be due to poor morphologic features, such as trochlear dysplasia, patella alta, and excessively rotated TT-TG intervals, and they are often characterized by multiple acute dislocations. 7,11 It is unclear whether this risk for patellar instability is inherent in the participation in high-intensity sports, but it can be presumed that the decline in instability rate with adulthood is attributable to activity modification with age or perhaps settled mechanics after growth ceases with musculature development. Therefore, it is important to identify all the factors that affect dislocation events and to evolve surgical techniques appropriate for this high-risk population. A single report, with a very short follow-up, is available describing the use of allograft for MPFLR in children. 6 The current study improves our understanding of allograft use for this surgery by presenting longer term follow-up and by comparing allograft directly with autograft techniques.
A study by Hohn and Pandya 6 in 2017 observed children for a minimum of 1 year and noted a 92% success rate regarding recurrent instability. Of their 25 adolescent patients 16% had a complication (2 with recurrent dislocation, 1 with a patellar fracture, and 1 with symptomatic hardware requiring implant removal). The investigators did not record any patient-derived outcome scores. Our results suggest decreasing success with duration from surgery for this high-risk group, with a combined recurrent dislocation rate of about 15% that appeared to worsen in the longer duration cohort. With a mean 3-year follow-up, the allograft cohort had the same 8% failure rate that the previous report 6 indicated for a mean 2-year follow-up. However, our autograft cohort, with a mean 6-year follow-up, had a higher failure rate of 26%. Although this could be attributed to a difference in graft choice or fixation type, we believe that this should be considered an overall rate of attrition regarding survivability of ligament reconstructions, particularly since the autograft is considered the gold standard in most ligament reconstruction surgeries.
When assessing complication rates within our cohort, we found that the overall rate (15%) compares well with that identified in a previous study reporting a rate of 16.2% in a similarly aged population with 3-year follow-up. 8 This previous study reported multiple different complications, including recurrent patellar dislocations, patellar fractures, and arthrofibrosis, whereas our only complications were recurrent instability. This same report found that nearly 50% of the complications were related to technical errors and therefore were potentially preventable. This is a potential limitation to our study, as we did not assess tunnel position with advanced imaging. During the evolution of our MPFLR technique, suture anchors were initially used to secure the graft to the patella, but this later changed to a potentially more secure fixation device with an interference screw. During the early years of this study, significantly more autograft tendons were fixed with suture anchors, and this could be another source for the higher failure rate (besides longer follow-up duration) in this cohort.
Another limitation of this study was not excluding the patients who required concomitant surgical intervention; however, excluding these patients would have significantly decreased the cohort sizes. Further, no significant differences were present in the secondary procedures (tibial tubercle transfers, lateral release, and loose body removal) between the allograft and autograft cohorts, either in the algorithm used to decide on a procedure or in the outcomes of the procedures. Therefore, it is unlikely that these secondary procedures affected the overall outcomes of each cohort. Finally, our results are underpowered (by definition of not having statistical significance). However, the effect size of comparing failure between the 2 graft types is 0.16, and the post hoc power analysis reports that we would need 307 patients to have 80% power. This suggests that our results are representative of a true nonsignificant difference between the allograft and autograft failure rates.
Despite the difference in duration to follow-up, we did not identify significant differences in return to sports. Depending on how this is evaluated, patients had reasonable success in returning to high-intensity athletics. If we consider all 59 adolescent patients (including those whose primary MPFLR failed), then the return-to-sports rate was 55.9%. But if we exclude those who did not experience failure with recurrent instability, then the rate was 66%. Moreover, if we exclude those who never played any sports (including before the initial injury), then the success rate was even better, with 73.3% of athletes able to return to their desired level of play.
A significant difference of 4.7 points was noted between the Kujala scores of the allograft and autograft cohorts. Yet the meaningful clinical difference between a mean score of 92.7 (allograft) and 97.4 (autograft) was not significant. The minimal clinically important difference in the Kujala score is between 7 and 14 points. Therefore, the difference seen here (although statistically different) was not clinically different.
The results of this study indicate that there are no clinically significant advantages of using an autograft tendon compared with an allograft tendon when reconstructing the MPFL in an adolescent patient. However, only a prospective randomized trial would be able to definitively compare the outcomes between these graft choices, as this would allow for control over concomitant procedures, follow-up durations, and isokinetic strength testing of the hamstring to assess harvest morbidity in the population. Although the graft choice does not appear to affect long-term outcomes with respect to recurrent patellar instability, pain, and return to activity, there is a clear trend toward questioning the long-term survival of MPFLR in the adolescent patient, independent of graft selection. As with all stabilizing surgeries in this high-risk population (shoulder instability, anterior cruciate ligament reconstruction 2,13 ), time may be a significant player in driving the reporting of unsuccessful outcomes.
Our hypothesis was proven correct, in that no differences were noted between the use of hamstring autograft versus allograft for MPFLR in teenage patients experiencing recurrent instability. The intangibles of faster surgery times (no need to harvest a graft) and the potential for reduced morbidity from hamstring harvest (posterior thigh pain, hamstring strength) may pose an arguably good reason for choosing allograft over autograft, yet the cost of allograft could be a valid reason for choosing autograft over allograft. Although our results need to be tempered by the high-risk population being studied, it appears clear that extra-articular MPFLR when performed with allograft tendon fares no worse than reconstruction with autograft tendon, and reconstructions with either tendon can have equally successful outcomes. Therefore, tendon choice can be based on either surgeon or patient preference in the teenage athlete with patellar instability.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.T.P. has received educational support from Smith & Nephew, Arthrex, and SportsTek Medical. E.W.E. is a consultant for OrthoPediatrics Corp and is a paid speaker/presenter for Arthrex.
Ethical approval for this study was obtained from the institutional review board at the University of California, San Diego.