
Abstract
Background:
Several recent studies have reported that favorable clinical results and a high level of patient satisfaction can generally be obtained with no increased risk of complications after single-bundle anterior cruciate ligament (ACL) reconstruction performed in patients >40 years of age. However, no studies have yet clarified the age-based differences in clinical outcomes after double-bundle reconstruction.
Purpose:
To compare clinical outcomes after double-bundle ACL reconstruction using hamstring tendon hybrid grafts between patients in 2 different age groups: ≥40 years and <40 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective study was conducted using 96 patients (48 men, 48 women ; mean age, 37 years) who underwent unilateral ACL reconstruction between 2008 and 2011. These patients were divided into 2 groups: group M included patients ≥40 years of age (n = 40 patients), and group Y included patients <40 years of age (n = 56 patients). All patients underwent the same anatomic double-bundle ACL reconstruction procedure. Clinical outcomes were evaluated at 2 years after surgery. Tunnel enlargement was also evaluated by computed digital radiography at 1 week and 2 years after surgery.
Results:
Mean postoperative side-to-side differences in anterior laxity were 0.5 ± 1.9 mm and 1.2 ± 1.5 mm in groups M and Y, respectively; there was a significant difference between the 2 groups (P = .039). There were no significant differences between the groups in Lysholm knee scores, International Knee Documentation Committee (IKDC) scores, or peak muscle torque of the hamstring. On the other hand, peak muscle torque of the quadriceps was significantly lower in group M (81%) than in group Y (89%) (P = .025). With respect to femoral tunnel enlargement, the posterolateral tunnel in group M was significantly larger than that in group Y on anteroposterior and lateral radiographs (P = .015 and P = .002, respectively).
Conclusion:
Equivalent clinical outcomes were seen between the 2 age groups after double-bundle ACL reconstruction. Postoperative anterior laxity was significantly less in older patients than in younger patients, however, older patients had significantly less quadriceps muscle strength than younger patients. Surgeons should be aware of residual muscle weakness and tunnel enlargement when performing double-bundle ACL reconstruction in older patients.
Keywords
Physical activity levels in older people have been increasing with rising life expectancy. 9 Therefore, anterior cruciate ligament (ACL) injuries occur more frequently in the population aged >40 years. 9,30,50 Previously, nonoperative treatment has been advocated for middle-aged persons with ACL tears because some surgeons worried that ACL reconstruction in these patients could lead to complications. 43,50 Recently, however, several studies have reported that favorable clinical results and a high level of patient satisfaction can generally be obtained with no increased risk of complications after single-bundle ACL reconstruction performed in patients aged >40 or >50 years. 5,7,8,10 –12,23,39,49,51 Some of these studies compared the subjective and functional results in these patients with those of patients <39 years of age, and they reported no significant differences between them. 3,8,9,23,34,50 In such comparative studies, however, objective evaluations including arthrometry and muscle weakness are not enough to reach a conclusion about the utility of ACL reconstruction.
Recently, anatomic double-bundle ACL reconstruction procedures have attracted attention. 25,26,55 Many randomized clinical trials have shown that these procedures are significantly superior to conventional single-bundle procedures for knee stability, 1,18,19,27,37,45,54,59 although other studies have failed to show significant differences. However, no studies have clarified the age-based differences in clinical outcomes after anatomic double-bundle reconstruction to date.
The purpose of this study was to compare clinical results after anatomic double-bundle ACL reconstruction between different age groups: patients aged ≥40 years and patients aged <40 years. In the present study, the following 2 hypotheses were tested. First, we hypothesized that there would be no significant differences in clinical outcomes after anatomic double-bundle ACL reconstruction between the 2 groups. Second, we expected that postoperative quadriceps torque would be significantly weaker in patients aged ≥40 years.
Methods
Study Design
A retrospective, comparative study was conducted with 96 patients (48 men and 48 women) who underwent anatomic double-bundle ACL reconstruction using hamstring tendon autografts between 2008 and 2011. The inclusion criteria consisted of patients who had unilateral ACL deficiency. The diagnosis of injured ligaments was made based on a detailed history of the knee injury, physical examinations, plain radiographs, magnetic resonance imaging scans, and findings at surgery. The contralateral knee in the patients was healthy and free of previous injuries. ACL reconstruction was recommended in patients if they wished to maintain an active lifestyle or if they had symptomatic instability with daily activities. Patients with a combined ligament injury of the posterior cruciate ligament and the lateral collateral ligament, the posterolateral corner structures of the knee, and the medial collateral ligament (grade 3) were excluded from this study. In addition, patients with any previous surgery for ligament injuries or a concurrent fracture were excluded from this study. The time from onset of injury to surgery was ≥1 month. This clinical study was accepted by the institutional review board of our hospital based on the described study design and after obtaining patients’ informed consent. Two senior orthopaedic surgeons (E.K. and K.Y.), who were sufficiently trained in the procedure, performed all surgeries.
Patient Demographics
All 96 study patients were divided into 2 age groups: ≥40 years (group M) and <40 years (group Y). Group M included 40 patients, with a mean age of 48 ± 7 years (range, 40-71 years). Group Y included 56 patients, with a mean age of 28 ± 6 years (range, 20-39 years). There were no significant differences between the 2 groups in sex, injured side, weight, body mass index, or time to surgery; there were significant differences in height, with the younger group being taller (Table 1).
Patient Demographics a
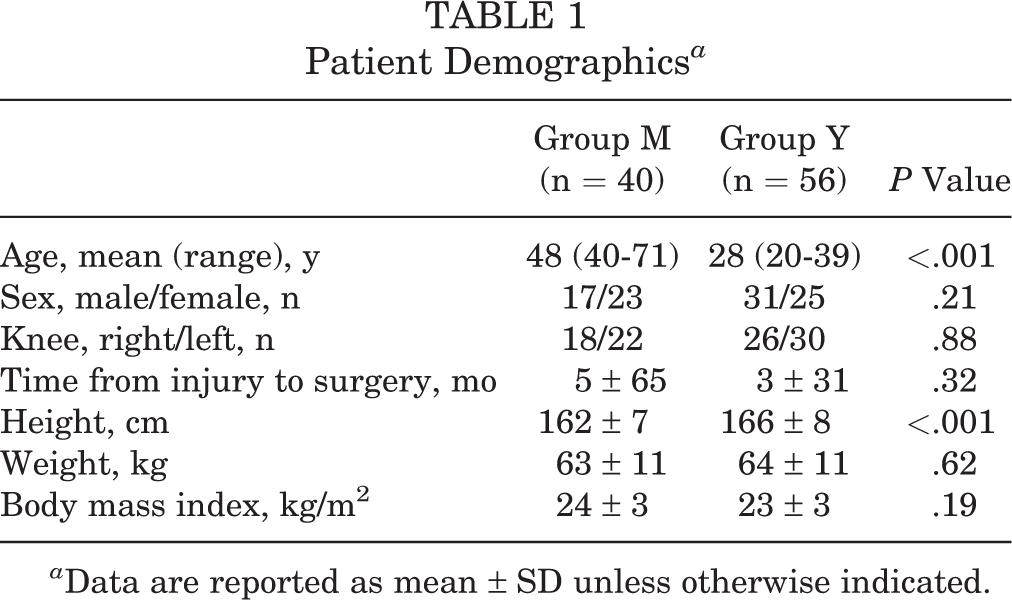
a Data are reported as mean ± SD unless otherwise indicated.
Surgical Procedure of Anatomic Double-Bundle ACL Reconstruction
In each group, the anatomic double-bundle ACL reconstruction procedure was performed with a hamstring tendon autograft using the transtibial tunnel technique. The details of the anatomic procedure have been previously described. 58,59
For graft preparation, the harvested semitendinosus tendon was cut in half and doubled over. A commercially available polyester tape (Leeds-Keio artificial ligament; Neoligaments) was mechanically connected at an unlooped end of the doubled tendon using a previously reported technique. 16,29 An Endobutton CL BTB (Smith & Nephew) was attached at the looped end. 36
To insert a guide wire, a hole-in-one guide (Wire-navigator; Smith & Nephew) was used. The tibial indicator was placed at the center of the posterolateral (PL) bundle footprint on the tibia. A guide wire was drilled through the sleeve in the tibia. Then, a guide wire for the anteromedial (AM) bundle reconstruction was inserted in the same manner. The 2 tibial tunnels were made with a cannulated drill corresponding to the measured diameter of the prepared substitute (AM: 6- to 7-mm diameter; PL: 5.5- to 6-mm diameter).
To create 2 femoral tunnels for the AM and PL bundles in the lateral condyle, a guide wire was first drilled at the center of the femoral attachment of the AM bundle through the AM tibial tunnel using an offset guide (Transtibial Femoral ACL Drill Guide; Arthrex). Then, the portal for the arthroscope was changed to the medial infrapatellar portal. A guide wire was inserted at the center of the PL bundle attachment on the femur through the PL tibial tunnel. Finally, 2 sockets were created for the AM and PL bundles, respectively, with cannulated drills. Then, the graft for the PL bundle was introduced through the tibial tunnel to the femoral tunnel using a passing pin. An Endobutton was flipped on the femoral cortical surface. The graft for the AM bundle was placed in the same manner. For graft fixation, an assistant surgeon simultaneously applied tension of 30 N to each graft using 2 tensiometers (Meira) at 10° of knee flexion for 2 minutes. Then, the surgeon simultaneously secured the 2 tape portions onto the tibia using 2 spiked staples (Smith & Nephew) in the turn-buckle fashion.
All patients underwent postoperative management using the same rehabilitation protocol. 27 The static squat exercise was started 1 week postoperatively, and a postoperative immobilizer was applied for 2 weeks after surgery. Full weightbearing walking was allowed with a hinged brace 2 weeks after surgery. Various kinds of athletic training were gradually allowed after 6 weeks, although no running was allowed until 9 months after surgery. Return to full sports activity was generally permitted at 12 months. The patients were followed up in our outpatient clinic for ≥2 years after surgery.
Clinical Evaluation
Side-to-side anterior laxity was measured using a KT-2000 arthrometer (MEDmetric) at 30° of knee flexion under an anterior drawer force of 133 N. An unblinded, well-trained physical therapist, who was not a coauthor of this study, collected the KT-2000 arthrometer results postoperatively. Another experienced orthopaedic surgeon (J.O.) performed the pivot-shift test, the results of which were subjectively evaluated as “2+,” “+,” and “–” using previously reported criteria. 27,59 For the overall evaluation, the Lysholm knee score (maximum score, 100), the objective International Knee Documentation Committee (IKDC) score, and the Tegner activity score were used. Peak isokinetic torques of the quadriceps and hamstring were measured at an angular velocity of 60 deg/s using Cybex II (Lumex) in both knees after surgery. Mean muscle torque, as measured 3 times postoperatively in the involved knee, is presented as a percentage of the uninvolved knee’s value. Anteroposterior (AP) weightbearing radiographs were taken for osteoarthritis grading using the Kellgren-Lawrence score. 22 During surgery, the status of the articular cartilage was graded according to the International Cartilage Repair Society classification.
Radiological Evaluation
All patients underwent a radiological examination twice: immediately postoperatively and 2 years after surgery. A radiograph in the AP view was taken in full extension so that the patella was located at the center of the distal femur and the medial third of the fibular head was partially obscured by the tibia. 32 A lateral view radiograph was taken with the knee flexed to approximately 45° so that the medial and lateral femoral condyles overlapped on the image. Computed digital radiographs (Fujifilm) of the knee were taken in the AP and lateral views to measure tunnel widening according to Webster et al. 52 Namely, the tunnel wall was enhanced in the computed digital radiograph, controlling contrast, intensity, and brightness of the image, and an experienced orthopaedic surgeon (T.O.) measured the diameter of the tunnel (Figures 1 and 2). The tunnel measurement was taken at the intra-articular outlets of the femoral tunnels in each plane, perpendicular to the direction of the long axis of the tunnels. Patients for whom the walls of the AM and PL tunnels could not be clearly identified on digital images were excluded from this portion.
To compare the femoral tunnel diameters in radiographs taken at 2 different periods, each diameter was shown as a percentage of the maximum joint width of the proximal tibia in the AP view, or as a percentage of the maximum diameter of the patella in the lateral view, according to Kawaguchi et al 20 (Figures 1 and 2). Then, the change in the diameter between the 2 periods was defined as the percentage of tunnel enlargement. It was difficult to determine the percentage of tunnel enlargement in the AM and PL tibial tunnels because the 2 intra-articular outlet images overlapped in the AP and lateral views. Therefore, the tibial tunnels were not measured in this study.

Computed digital radiographs of a patient in the M group 2 years after anatomic double-bundle anterior cruciate ligament reconstruction. The sclerotic lines of the tunnel wall are enhanced in the anteroposterior (left) and lateral (right) views. The small white arrows show the femoral outlet of the anteromedial tunnel, while the small black arrows show the femoral outlet of the posterolateral tunnel. The 2 femoral tunnel diameters are shown as (A) a percentage of the maximum joint width of the proximal tibia (dashed line) in the anteroposterior view or (B) a percentage of the maximum length of the patella (dashed line) in the lateral view.

Computed digital radiographs of a patient in the Y group 2 years after anatomic double-bundle anterior cruciate ligament reconstruction. The sclerotic lines of the tunnel wall are enhanced in the anteroposterior (left) and lateral (right) views. The small white arrows show the femoral outlet of the anteromedial tunnel, while the small black arrows show the femoral outlet of the posterolateral tunnel. The 2 femoral tunnel diameters are shown as (A) a percentage of the maximum joint width of the proximal tibia (dashed line) in the anteroposterior view or (B) a percentage of the maximum length of the patella (dashed line) in the lateral view.
Statistical Analysis
An a priori power analysis was performed, and the sample size was calculated to have 71% to 87% power to test the hypothesis. Statistical analyses comparing 2 groups were conducted using the unpaired t test and the chi-square test. A commercially available software program (StatView; SAS Institute) was used for statistical calculations. The significance level was set at P = .05.
Results
During surgery, there were no serious complications such as iatrogenic cartilage injuries, serious malpositioning of the tunnels, or graft fixation failure. There were no serious postoperative complications, including fractures, symptomatic deep vein thrombosis, and infections, in either group.
With respect to intraoperative arthroscopic findings, a medial or lateral meniscal tear was found in 24 patients (60%) and 36 patients (64%) in groups M and Y, respectively; this difference was not statistically significant (Table 2). Three and 7 meniscal lesions were sutured in groups M and Y, respectively, while 13 and 11 meniscal lesions were resected in groups M and Y, respectively. There were no significant differences in meniscal treatment between the 2 groups. With respect to chondral injuries, the chi-square test showed a significantly greater number of chondral injuries in group M than in group Y (P = .04) (Table 2).
Intraoperative Findings a

a ICRS, International Cartilage Repair Society.
Mean preoperative side-to-side anterior laxity was 4.0 ± 2.6 mm and 4.1 ± 2.9 mm in groups M and Y, respectively; there was no significant difference between the 2 groups. Postoperative side-to-side anterior laxity averaged 0.5 ± 1.9 mm and 1.2 ± 1.5 mm in groups M and Y, respectively; this difference was statistically significant (P = .039) (Table 3). In addition, we divided the side-to-side laxity values into 3 categories: ≤0 mm, >0 and <3 mm, and ≥3 mm; the number of patients in each category are listed in Table 3. There were no significant differences in the ratio of the 3 categories between the 2 groups. Regarding the pivot-shift test, the chi-square test showed no significant differences between the 2 groups; there were also no significant between-group differences in postoperative loss of terminal knee motion, Lysholm knee score, IKDC score, and hamstring muscle torque (Table 3). However, quadriceps muscle torque values were significantly lower in group M than in group Y (P = .025). There was a significant difference in the postoperative Tegner activity score between the 2 groups (mean score, 5.1 and 5.9 in groups M and Y, respectively). However, patients in both groups were able to return to their preinjury activity level (mean preinjury score, 5.3 and 6.0 in groups M and Y, respectively). In both groups, there were no significant differences in the change in activity level between preinjury and 2-year follow-up.
Clinical Outcomes a
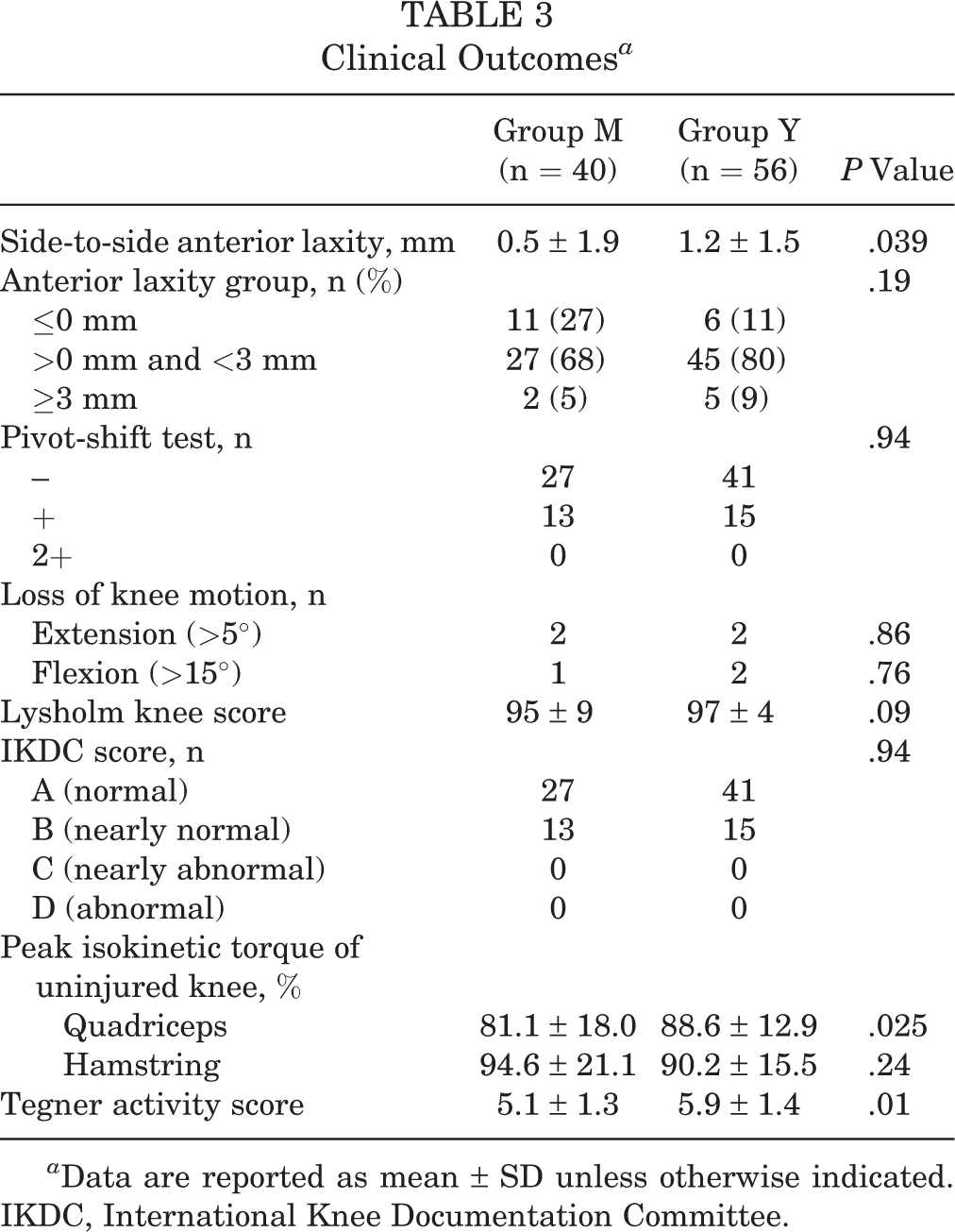
a Data are reported as mean ± SD unless otherwise indicated. IKDC, International Knee Documentation Committee.
With respect to the radiological osteoarthritis grade, the preoperative and postoperative Kellgren-Lawrence scores were significantly higher in group M than in group Y (P < .0001). However, there were no significant differences between preinjury and 2-year follow-up in both groups M and Y (Table 4).
Pre- and Postoperative Kellgren-Lawrence Osteoarthritis Grades

A total of 17 patients (6 patients and 11 patients in groups M and Y, respectively) were excluded from this portion of the study because the walls of the AM and PL tunnels could not be clearly identified on digital images. Therefore, radiological tunnel enlargement was evaluated in the other 79 patients (34 patients and 45 patients in groups M and Y, respectively). The percentage of tunnel enlargement of the AM femoral tunnel averaged 21.0% and 18.2% in the AP view and 14.8% and 14.5% in the lateral view in groups M and Y, respectively (Table 5). There were no significant differences between the 2 groups. The percentage of tunnel enlargement of the PL femoral tunnel averaged 14.1% and 7.3% in the AP view and 15.0% and 5.7% in the lateral view in groups M and Y, respectively; these percentages were significantly greater in group M than in group Y (P = .015 and .002 for the AP and lateral views, respectively). However, tunnel enlargement did not significantly affect the clinical results in each group on Spearman correlation analysis.
Radiological Percentage of Tunnel Enlargement

Discussion
This is the first study to compare clinical results after anatomic double-bundle ACL reconstruction between patients in different age groups. Aside from height, there were no significant differences in the background factors, including preoperative knee laxity, between the 2 groups. Subjectively, there were no significant differences in the Lysholm and IKDC scores between the 2 age groups after anatomic double-bundle ACL reconstruction. Postoperative anterior knee laxity was significantly less for older patients compared with younger patients, however, older patients had significantly less quadriceps muscle strength compared with younger patients. Also, PL femoral tunnel enlargement was significantly greater in older patients than in younger patients, although tunnel enlargement did not affect the clinical outcomes.
There were no serious complications in either group. Recently, Mall et al 33 reported a systematic review of results after single-bundle ACL reconstruction in patients aged >40 years. They concluded that ACL reconstruction can be recommended to patients >40 years of age who wish to maintain an active lifestyle or who have symptomatic instability with daily activities. Complication rates were low in this patient population, and the outcomes were similar to those in younger patients. The results of the present study in patients ≥40 years of age with double-bundle hamstring hybrid autografts showed a mean Lysholm score of 95 and 68% with an IKDC grade A. These findings were comparable with those in the younger control group and the results already reported by other authors. 6,14,44 Therefore, double-bundle reconstruction is also an option for active patients aged ≥40 years.
Postoperative side-to-side anterior laxity measured with the KT-2000 arthrometer averaged 0.5 mm and 1.2 mm in the older and younger age groups, respectively. In the study of Plancher et al, 44 a postoperative side-to-side difference of 1.4 mm was seen in patients >40 years of age when measuring with the KT-1000 arthrometer and using bone-tendon-bone grafts. Barber et al 3 and Bohnsack et al 6 found AP translations of 1.5 mm and 1.2 mm in >40-year-old patients when measuring with the KT-1000 arthrometer. This is in contrast to the majority of articles in the literature, in which no differences were found between the 2 groups.3,6,30,33 However, Conteduca et al 9 reported that greater knee stability was found in patients aged >40 years when compared with younger patient groups.
We speculated as to the reasons why postoperative knee stability was significantly better in the older patients in the present study. In anatomic double-bundle reconstruction, anterior tibial translation is slightly overconstrained immediately after surgery. 25,26 Biomechanical studies have shown no difference in knee stability between younger and older cadaveric knees. 25,26 However, after ACL reconstruction, the structural properties of a tendon autograft deteriorate during the remodeling phase, and the reduced properties are not completely restored even at 12 months after surgery. 28 Knee laxity may be influenced subsequently by graft remodeling, which has been demonstrated to affect the fate of ACL reconstruction. 38 In addition, after ACL reconstruction, stress relaxation occurs after surgery, even after rigorous preconditioning. 2 The postoperative Tegner activity score averaged 5.1 in older patients in the current study. In our opinion, the difference compared with the younger patients, in whom a mean of 5.9 was obtained, seems reasonable because patients may become less active at a high sports level when they are older. 15 Therefore, we speculate that knee laxity in the younger patients was gradually increasing during postoperative rehabilitation based on their activities and lifestyle.
On the other hand, osteoarthritis is certainly a factor in an older population and could modify articular structures in some patients, resulting in a more rigid knee. This could certainly influence the arthrometric results obtained in this series, with more rigid knees found in patients aged ≥40 years. The radiological evaluation showed a significant difference between the 2 age groups, with higher osteoarthritis grades in group M. Osteoarthritis is a well-known consequence after ACL reconstruction. However, it must also be considered that restoring knee stability can decrease further osteoarthritis progression from chronic knee instability after nonoperative treatment; this is because of a lower risk of subluxations or further injuries.
There may be a criticism that a mean difference of 0.7 mm in knee laxity is not clinically meaningful for the patient, even though it is statistically significant. However, this does not mean that postoperative knee laxity was improved only by 0.7 mm in each knee. Thus, we should regard the 0.7-mm improvement in laxity in group M as an indication that double-bundle reconstruction could significantly increase the number of knees with normal laxity in older patients. We believe that it is clinically important to restore normal knee stability because knee instability may cause meniscal injuries and osteoarthritic changes in the long term after ACL reconstruction, resulting in poorer functional outcomes. We should note that all of the patients who underwent ACL reconstruction simply hoped to achieve the same stability and functionality as in their contralateral knee. We consider that the ideal goal of ACL reconstruction is to simultaneously restore normal knee stability and normal knee function. From this perspective, we expect that the improvement in knee stability will show subjective and functional benefits to patients in future long-term follow-up studies.
In this study, a commercially available polyester tape (Leeds-Keio artificial ligament) was used in ACL reconstruction. However, this tape was not used as an artificial ligament or an augmentation device but as one of the fixation devices for the hamstring tendon graft to the bone. Namely, the tape was connected in series with the doubled tendon using our original technique, 60,61 and only the autogenous tendon portion was placed across the joint. It is well known that the weak points of a hamstring tendon graft fixed with sutures to the bone are (1) low stiffness of the graft-suture-bone complex, (2) rapid relaxation of graft tension after surgery, and (3) difficulty in tension control during graft fixation. 38,56,61 The “hybrid graft” was used to improve upon these weak points. Namely, the femur graft–tibia complex with the hybrid graft involves the following advantages according to biomechanical properties with the tensile test and the cyclic loading test 24,35,56 : (1) higher stiffness and stronger ultimate loads than the complex with the suture method; (2) more resistance to graft tension relaxation; and (3) clinically, an acceptably long and thick hybrid graft that can be fashioned by surgeons with a relatively short or thin autogenous tendon and a hybrid graft that can be more easily fixed to the bone, applying tension quantified using a tensiometer to the graft. We understand that the hybrid graft technique is not commonly used for ACL reconstruction at the present time.
On the basis of biomechanical studies and clinical trials, a double-bundle reconstruction technique has recently been proposed to better restore the anatomy and biomechanics of the native ligament. 45 Biomechanical studies have found that anatomic double-bundle ACL reconstruction can restore knee stability significantly more closely to the normal level than conventional single-bundle reconstruction. 25,26,55 In previously published original trials using hamstring tendons, anterior and/or rotatory stability of the knee was significantly better after anatomic double-bundle ACL reconstruction than after conventional single-bundle reconstruction. 1,18,19,27,37,45,54,59 Reports have shown that the reconstruction of both bundles of the ACL leads to improved knee stability, especially with regard to rotatory loads. 13,54 However, the clinical outcomes of the 2 procedures are still controversial, 42,47,53 and objective data documenting a difference between the 2 reconstruction methods are still lacking because studies have shown statistically significant differences only with respect to the pivot-shift test. 54
In the present study, the strength of the quadriceps muscle was significantly lower in older patients than in younger patients. In such comparative studies, 3,9,23,34,50 however, objective evaluations concerning muscle weakness are not enough to reach a conclusion about the utility of ACL reconstruction. Previous studies have shown that quadriceps weakness may be a risk factor for the development of knee osteoarthritis. 40,46,48 Quadriceps muscle weakness, which is often seen after ACL injuries, 41 has been shown to increase knee joint loading patterns and reduce shock absorption, and it has thus been suggested as a significant risk factor for the development of knee osteoarthritis. 40,46 Atrophy of the quadriceps and hamstring often occurs after ACL reconstruction. Even if static stability is restored, return to sports activities and recovery of normal knee function are difficult. 31 Iriuchishima et al 17 reported that age was the only predictor of muscle recovery after ACL reconstruction. We speculated on the reasons why older patients had weaker quadriceps muscles than younger patients. In the older patients, muscle atrophy was quicker after injury and surgery. Muscle recovery was slower after surgery. The risk of muscle recovery delay increased with age. Therefore, careful and continuous rehabilitation should be performed for muscle strength recovery in older patients after ACL reconstruction.
Using computed tomography, Kawaguchi et al 21 reported tunnel enlargement after double-bundle ACL reconstruction with a hamstring tendon autograft. They noted that the degree of tunnel enlargement of the AM femoral tunnel averaged 11.1%, 9.8%, and 10.7% on the coronal, sagittal, and axial images, respectively, while that of the PL femoral tunnel averaged 7.0%, 8.9%, and 7.6%, respectively. There was no significant correlation between the degree of each tunnel enlargement and the clinical outcome. Yanagisawa et al 57 reported that age was a preoperative factor associated with tunnel enlargement after double-bundle ACL reconstruction. They also noted that the percentages of enlargement of the AM femoral tunnel, PL femoral tunnel, and AM tibial tunnel were associated with patient age, although there was no significant difference in the PL femoral tunnel between patients aged <40 years and >40 years. However, in the present study, PL femoral tunnel enlargement was significantly greater in older patients (14.1%-15.0%) than in younger patients (5.7%-7.3%). Recently, it has been postulated that postoperative periarticular loss of bone mineral density might be associated with tunnel enlargement. 4 Biological and bony density differences may explain why PL femoral tunnel enlargement was more likely to be found in older patients than in younger patients after double-bundle reconstruction.
There are several limitations to this study. The first is that the number of patients was not truly equal in the 2 different age groups. Although sex, weight, and time from injury to surgery were not completely the same between the 2 groups, there were no significant differences. The second limitation is that we only evaluated the peak isokinetic torque of the quadriceps and hamstring at an angular velocity of 60 deg/s after ACL reconstruction with hamstring tendon grafts. Ideally, the muscles would also be tested at higher speeds. The third limitation is that we did not check bone density. The fourth is that the follow-up period was only 2 years. Therefore, at the present time, we cannot speculate as to whether there will be differences between the 2 age groups in terms of long-term outcomes of knee function and return to sports or whether quadriceps weakness will improve over time in the M group. In the future, we will conduct a long-term follow-up study to compare clinical outcomes between the 2 groups. However, despite these limitations, the present study provides orthopaedic surgeons with important information on double-bundle ACL reconstruction with hamstring tendons.
Conclusion
The results of this study demonstrated that there were no significant differences in postoperative outcomes between patients <40 years and those ≥40 years after anatomic double-bundle ACL reconstruction. However, recovery of the quadriceps muscle was significantly decreased in older patients than in younger patients. Furthermore, PL femoral tunnel enlargement was greater in older patients than in younger patients. Although postoperative anterior knee laxity was significantly less in older compared with younger patients, osteoarthritic changes were significantly greater and there were significantly more chondral lesions in the older patient group.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Hokkaido University Hospital, Sapporo, Japan.