
Abstract
Background:
Osteochondritis dissecans (OCD) of the elbow has almost exclusively been described in the humeral capitellum, with only a small number of reports describing secondary osteochondral changes in the radial head.
Hypothesis:
The authors hypothesized that concomitant radial head lesions (RHLs) would be seen with capitellar OCD and that patients with RHLs would present with more advanced capitellar OCD lesions and would respond better to procedures restoring articular congruity.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 86 elbows from 82 patients (39 female patients; mean ± SD age, 13.8 ± 2.2 years; age range, 9.8-23.6 years) were treated for capitellar OCD and enrolled in a prospective registry. Clinical and radiographic data were compared between those with and without RHLs, with a median follow-up of 10.8 months (interquartile range, 6.2-17.1 months). Magnetic resonance imaging was used to characterize and measure RHLs and OCD lesions. Postoperative clinical results were compared between patients who underwent drilling and those who had osteochondral autograft transplantation surgery (OATS).
Results:
RHLs were present in 26 (30%) elbows—17 in the dominant arm. Edema was seen in 22 elbows; 17 had involvement of the anterior third of the radial epiphysis. Cysts were present in 4 elbows: 2 in the anterior third and 2 in the middle third. Blunting of the normal concave contour of the radial epiphysis was present in 10 elbows in the anterior third. Demographic and presenting clinical features were similar between those with and without RHLs. RHLs were more commonly seen in Nelson grade 4 OCD lesions (P = .04) as compared with elbows without RHLs. Elbows with RHLs that underwent OATS (n = 9) trended toward greater improvement in forearm range of motion (P = .058) and fewer persistent mechanical symptoms (P = .06) postoperatively as compared with elbows having RHLs that underwent drilling. There were no postoperative differences in elbows without RHLs that underwent OATS versus drilling.
Conclusion:
RHLs were seen in one-third of elbows with capitellar OCD. Lesions predominantly occurred in the anterior RH in patients with more advanced capitellar lesions. Short-term clinical follow-up suggested greater improvement in range of motion and resolution of mechanical symptoms for patients with RHLs who were treated with OATS than with drilling.
Capitellar osteochondritis dissecans (OCD) is most commonly seen in children and adolescents who participate in sports involving repetitive compression forces and valgus torque at the elbow, such as baseball and gymnastics. 3,10,14,18,21 It is hypothesized that the capitellar chondroepiphysis is vulnerable owing to limited vascularity and that repetitive microtrauma exerted across the radiocapitellar joint leads to subchondral bone failure. The articular cartilage then becomes more susceptible to compression and shear forces exerted by the radial head, leading to eventual cartilage separation, fragmentation, and loose body formation. 20 Existing literature also suggests that a disparity in mechanical properties and thickness of cartilage in the capitellum and radial head play a role in capitellar OCD development. 19
To date, evaluation and treatment have almost exclusively focused on the capitellar lesion in OCD. Only a small number of case reports exist describing solitary or concomitant osteochondral changes in the radial head. 5,9,22 The purpose of this study was to describe the presenting clinical and radiographic characteristics of patients with capitellar OCD and concomitant radial head changes and to compare them with patients having only capitellar OCD. As a secondary aim, we compared clinical outcomes between patients with radial head lesions (RHLs) and those without. We hypothesized that patients with RHLs would present with more limited elbow motion and more advanced capitellar OCD lesions. Additionally, those with RHLs would have improved outcomes with procedures that restore articular congruity (ie, osteochondral autologous transplantation surgery [OATS]).
Methods
Between March 2014 and July 2016, 88 patients presenting to a tertiary children’s hospital and diagnosed with capitellar OCD were enrolled in an institutional review board–approved prospective registry. Six patients were excluded owing to inadequate quality imaging on presentation, resulting in 82 patients with 86 affected elbows enrolled in this study. There were 43 male patients with 46 affected elbows and 39 female patients with 40 affected elbows (Table 1). Three patients had bilateral involvement at initial presentation. One was evaluated 2 years following initial presentation with involvement of the contralateral side. The mean ± SD age at the time of clinical presentation was 13.8 ± 2.2 years (range, 9.8-23.6 years), and mean symptom duration was 12.1 ± 18.4 months. The median clinical follow-up for all patients was 10.8 months (interquartile range, 6.2-17.1 months).
Preoperative Demographic and Clinical Features Among Patients by Sex

Patients were diagnosed with OCD based on physical examination findings, plain radiographs, and/or magnetic resonance imaging (MRI). Historical features collected included sport participation, symptom duration, pain, and mechanical history, which was defined as patient-reported locking, catching, clicking, or crepitus. Pain was assessed with an 11-point pain numeric rating scale. 8 Pre- and postoperative clinical examination findings of interest were arc of motion (shoulder, elbow, and forearm), mechanical symptoms (eg, locking, clicking, catching, and crepitus), and radiocapitellar instability. Return to sport was assessed at final clinical follow-up via a questionnaire asking patients if they had returned to their primary sport.
Plain radiographs were assessed with the Sauvegrain bone age technique to determine the skeletal age of all patients. 4 Coronal and sagittal MRI scans were used to confirm the diagnosis of capitellar OCD and classify the lesion according to the Nelson grading scheme. 16 In particular, fluid-sensitive sequences, including double-echo steady-state (DESS) and T2, were used to stage severity of OCD. The DESS sequence produces a higher T2-weighted image, more specific and sensitive in assessment of cartilage and synovial fluid. 6,7
Sagittal MRI scans were used to measure capitellar OCD width and depth, which were then reported as a percentage of the capitellar diameter (Figure 1A). Sagittal MRI sequences were chosen to best characterize subchondral bone changes; standard axial and coronal images, while helpful in identifying the OCD, do not provide easy quantitative analysis of the depth of bony involvement. Capitellar diameter was determined by drawing a best-fit circle over the humeral capitellum on sagittal MRI. The capitellar OCD area was then determined by tracing the OCD lesion with a free-hand draw tool on the imaging program (Fujifilm Synapse PACS, v 4.4) and dividing by the area of the best-fit circle (Figure 1B). All measurements were taken on the slice with the largest lesion size. DESS, T2, and T1 sequences—in this order based on imaging availability—were used to make capitellar OCD width, depth, and area measurements. Sagittal MRI was used to identify and measure RHLs located proximal to the radial physis. Lesion width and depth were taken on the sagittal MRI slice with the largest lesion size 13 and reported as a percentage of sagittal radial head width. The location of each type of lesion was determined by dividing the radial head into anterior, middle, and posterior thirds.
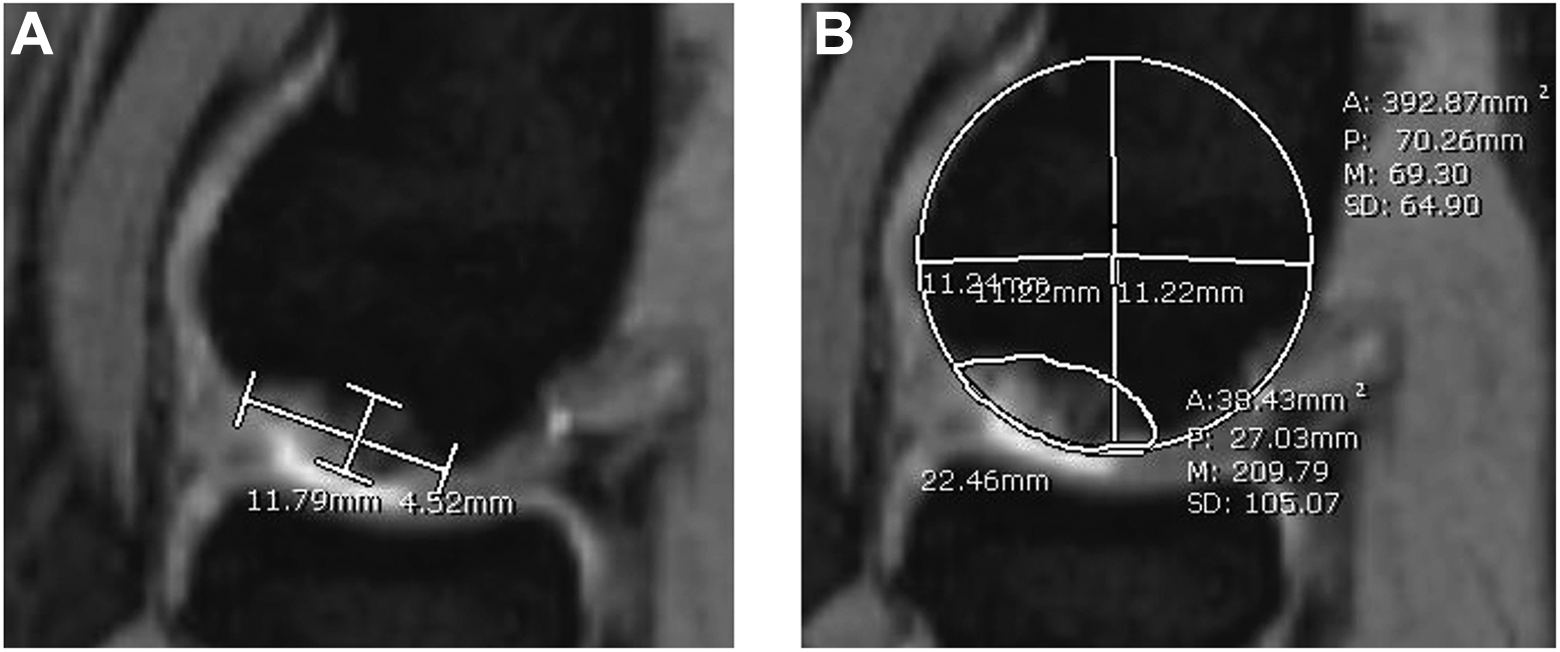
Capitellar osteochondritis dissecans lesion on sagittal double-echo steady-state magnetic resonance imaging. (A) Lesion width and depth reported as a percentage of the best-fit circle’s diameter. (B) Lesion area determined by drawing the best-fit circle around the capitellum and tracing the lesion with a free-hand draw tool. Images courtesy of Children’s Orthopaedic Surgery Foundation, 2017.
Surgery was performed by 1 of 4 fellowship-trained orthopaedic surgeons (D.S.B.) at our institution for symptomatic patients with unstable OCD lesions and/or those with persistent OCD despite 6 months of nonoperative care. Depending on OCD lesion characteristics (stable vs unstable, lesion displacement), patients underwent drilling, microfracture, OATS, fragment fixation, and/or loose body removal. In general, patients with uncontained or deep lesions—for whom the subchondral plate was not intact and the subchondral bone was fibrinous or necrotic—underwent OATS. We specifically report on outcomes in drilling and OATS. In the group with RHLs on preoperative imaging, 22 underwent surgery, with 8 and 9 undergoing drilling and OATS, respectively. In the group without RHLs, 49 underwent surgery, which included 14 drilling and 22 OATS procedures (Figure 2). Patients lost to follow-up after surgery were excluded from the study cohort. There was 1 patient with only an initial visit, but we included him to look at RHLs and clinical presentation, since he was not one of our surgical patients requiring postoperative clinical results.

Clinical course of patients (A) with and (B) without radial head lesions. OATS, osteochondral autograft transplantation surgery; RHL, radial head lesion.
Descriptive statistics included frequency counts and percentages for categorical variables and means and standard deviations for continuous variables. Because some patients had bilateral elbow involvement, repeated-measures analysis was performed with generalized estimating equations of score test results. Presenting clinical and radiographic features were compared between those with and without RHLs. Additionally, postoperative clinical features of elbows with RHLs that underwent OATS were compared with elbows having RHLs that underwent drilling. The same comparison between OATS and drilling was made for elbows without RHLs. A P value <.05 was considered statistically significant. SAS (v 9.4; SAS Institute) and SPSS (v 22.0; IBM) software were used.
Results
RHLs (edema, cysts, or blunting) were seen in 26 (30%) of 86 elbows (Figure 3). Of these 26 elbows, 8 (31%) had more than 1 type of lesion present. Edema specifically was present in 22 (26%) elbows, with a mean width and depth of 41% ± 21% and 13% ± 5%, respectively. Of 22 edematous lesions, 17 involved the anterior third of the radial head, and 5 involved only the middle third or posterior third.
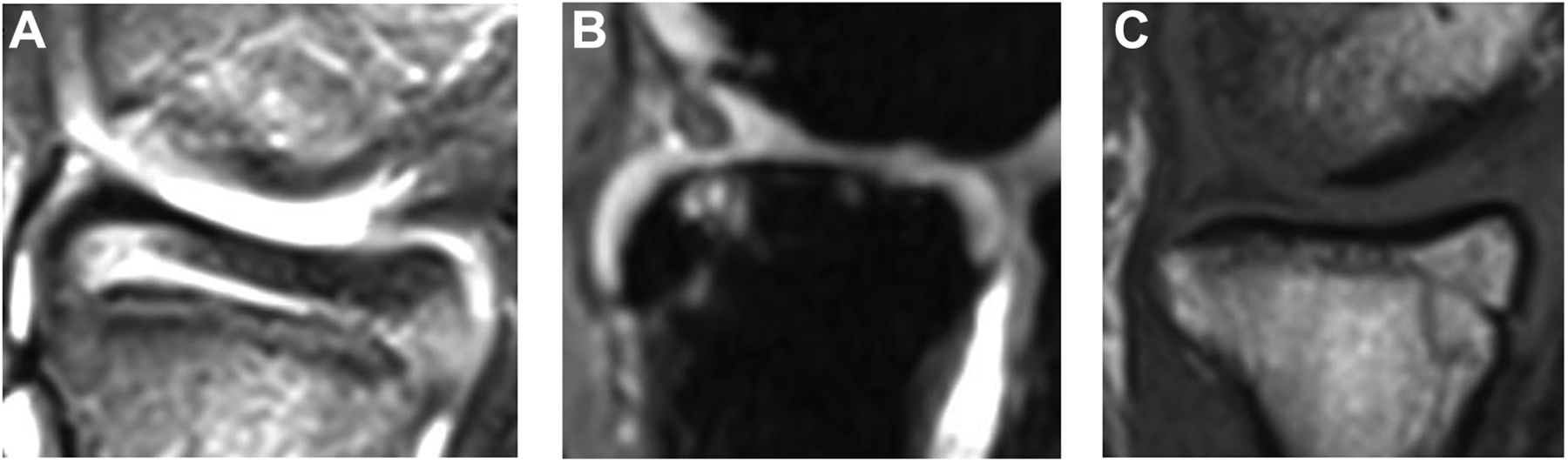
Types of radial head lesions identified on sagittal magnetic resonance imaging. (A) Edema in the anterior third of the radial head. (B) Cysts in the anterior third of the radial head on double-echo steady-state magnetic resonance imaging sequence. (C) Blunting of the anterior radial head. Images courtesy of Children’s Orthopaedic Surgery Foundation, 2017.
Cystic RHLs were present in 4 (5%) elbows. The mean width and depth were 11% ± 5% and 8% ± 5%, respectively. Two cystic lesions were located in the anterior third and 2 in the middle third.
Blunting—or loss of the sharp concave margin of the radial epiphysis—was present in 10 (12%) elbows, all in the anterior third. Cystic lesions were best appreciated on sagittal DESS sequences or T2 sequences if DESS was unavailable. Edema was best visualized on T2 sequences. Blunting was identified on T1, T2, or DESS sequences. Of note, subchondral sclerosis was appreciated in many radial heads, although this was difficult to quantify.
Clinically, patients with RHLs presented similarly with respect to patient age (chronological and skeletal), sex, symptom duration, lesion laterality, pain scores, and range of motion (Table 2). Although 74% (17 of 23) of elbows with RHLs presented with a history of mechanical symptoms, as compared with 58% (31 of 53) of those without RHLs, this was not statistically significant (P = .18).
Preoperative Demographic and Clinical Features in Patients With and Without RHLs a
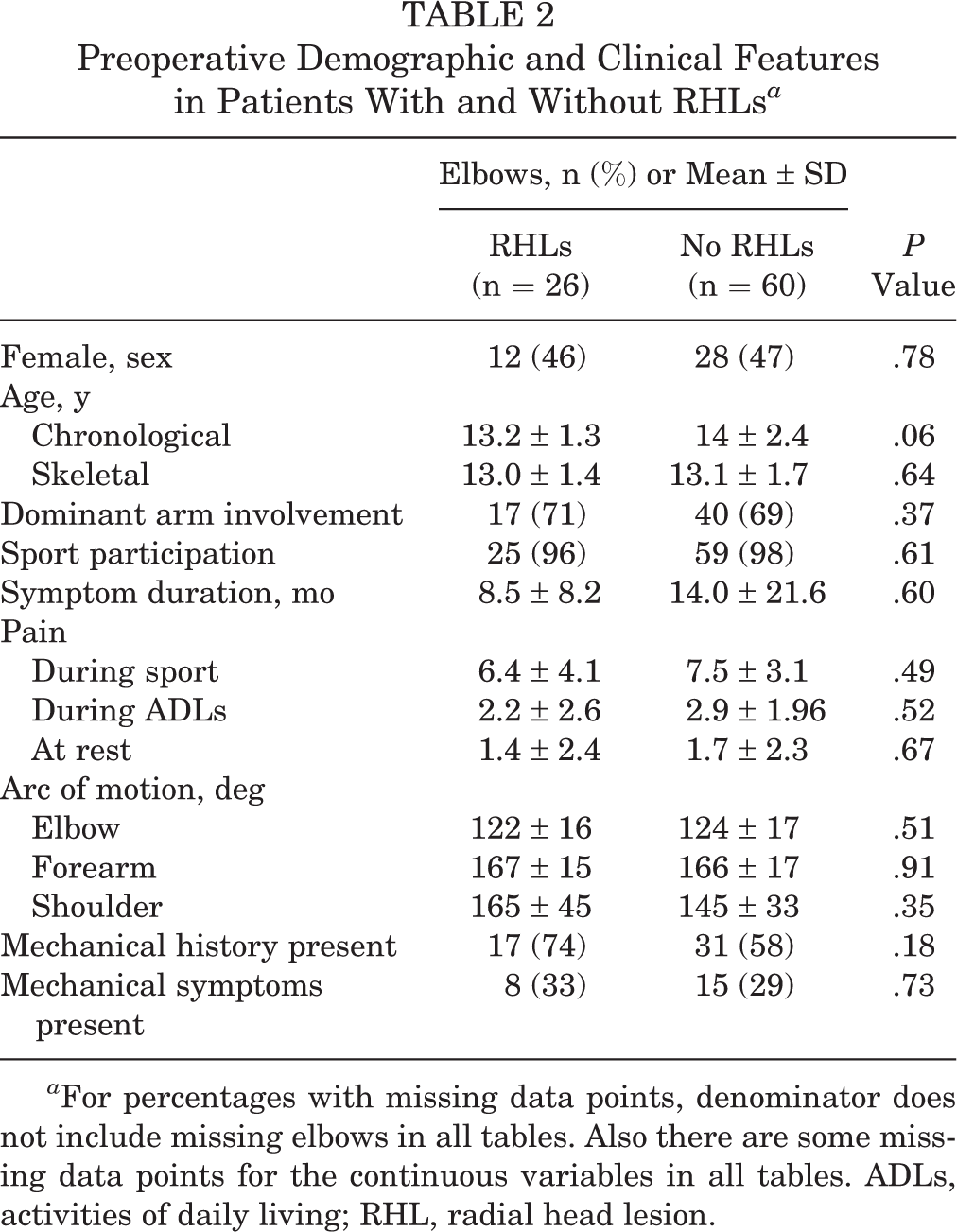
a For percentages with missing data points, denominator does not include missing elbows in all tables. Also there are some missing data points for the continuous variables in all tables. ADLs, activities of daily living; RHL, radial head lesion.
When radiographic findings were compared between the 2 groups (Table 3), there were significantly more elbows with loose bodies (Nelson grade 4) in patients with RHLs (46%; 12 of 26) than in those without RHLs (22%; 13 of 60) (P = .04). However, the mean Nelson grade did not differ between groups. The mean size of the radial head in relation to the capitellum was greater in elbows with RHLs (ratio, 2.31) versus those without RHLs (ratio, 2.26), although this was not significantly different (P = .25). The size of the capitellar OCD lesion (width, depth, and area) was not associated with the presence of RHLs.
Radiographic Findings in Patients With and Without RHLs a

a AP, anteroposterior; OCD, osteochondritis dissecans; RHL, radial head lesion.
b Nelson grading classified as 1 = thickening of intact articular cartilage and low signal changes in humeral capitellum; 2 = articular cartilage breached, low signal rim behind OCD fragment; 3 = articular cartilage breached, high signal changes behind OCD fragment; and 4 = loose body.
Additionally, evidence of radial head subluxation, determined per plane radiograph and clinical examination, was present in 4 (15%) of 26 elbows with RHLs versus only 1 (2%) of 60 elbows without RHLs (P = .06). In the single patient with radiocapitellar subluxation without RHL, there was considerable edema in the proximal radial metaphysis and diaphysis; however, this patient was not deemed to have an RHL owing to our strict radiographic criteria. If a broader definition of proximal radial changes were utilized, all patients with radial head subluxation would have radial head changes.
For patients who went on to surgery, we compared the postoperative results between the 9 elbows with RHLs that underwent OATS and the 8 elbows with RHLs that underwent drilling. Of the 8 patients with RHLs who underwent drilling, 2 had persistent mechanical symptoms at final clinical follow-up, as opposed to none of the patients with RHLs who underwent OATS (P = .06). There was also greater improvement in range of forearm arc of motion (improvement of 2°) for patients with OATS versus those who had drilling performed (loss of 10°; P = .06), although this improvement may not be of clinical significance. There was no significant difference in mean change of shoulder or elbow motion (pre- to postoperative), pain scores, or rate of return to sport between the OATS RHL group and drilling RHL group. When the results of patients without RHLs who underwent OATS versus drilling were compared, there were no significant differences in pain scores, range of motion, mechanical symptoms, or return to sport (Table 4).
Postoperative Results Comparing OATS and Drilling Between Patients With and Without RHLs a

a Data are shown as mean ± SD or n (%). ADLs, activities of daily living; OATS, osteochondral autograft transplantation surgery; RHL, radial head lesion.
b Dash indicates data was not measured.
Discussion
The exact etiology of capitellar OCD is unclear, although existing literature suggests that repetitive and/or high valgus forces applied to the radiocapitellar joint are a primary etiologic factor. 2,11,15,17 Repetitive microtrauma exposes the radiocapitellar articulation to increased compression and shear forces, which can equal up to 2.4 times a patient’s body weight during certain sporting activities. 12,15 OCD has frequently been reported in male baseball players and female gymnasts, as demonstrated in the current study. Given the stresses placed on the elbow in patients with capitellar OCD, we sought to investigate the concomitant changes in the radial head. These changes included edema (n = 22), cysts (n = 4), and blunting (n = 10). Specifically, this study aimed to describe radial head changes seen in conjunction with capitellar OCD and how they compared clinically and radiographically with elbows that had capitellar OCD without concomitant RHLs. We also investigated postoperative clinical outcomes between those with and without RHLs.
Prior studies reporting RHLs described them as isolated, in the posteromedial aspect of the radial head, and occurring in the context of anterior radial head subluxation. 5,22 Given that our findings describe RHLs located primarily in the anterior radial head associated with capitellar OCD, we propose that the changes described in this study are a previously uncharacterized entity.
Regarding the etiology and pathogenesis of these lesions, we propose that (1) increased forces on the radial head, (2) intrinsic biomechanical properties, and (3) articular incongruity all play a role in RHL development. In a cadaveric study from 2013, Mihata and colleagues 15 demonstrated that presence of capitellar osteochondral defects result in increased elbow valgus laxity and contact pressure in the radiocapitellar joint as compared with elbows without capitellar OCD. As all of the patients in the current investigation had capitellar OCD, the radial heads presented here may have been subjected to increased contact pressures relative to those of the general population. The intrinsic material and biomechanical properties in a skeletally immature cohort may also predispose these patients to radial head changes; the mean skeletal age of patients with RHLs in this study was 13 years. Skeletally immature individuals have increased ligamentous laxity and greater cartilaginous composition of the radial head, perhaps contributing to shear and compressive forces across the radiocapitellar joint, leading to the described subsequent RHLs.
This study raises questions about how articular incongruity may play a role in the pathogenesis of RHLs. The observation that radial head changes—including radiocapitellar subluxation—were more commonly seen in patients with more advanced OCD lesions (Nelson grade 4) suggests that the radial head may engage the capitellar incongruity in positions of loading, as depicted in Figure 4. The finding that RHLs were not as common in grade 3 OCD lesions may be attributed to the fact that grade 3 lesions, although unstable, do not lead to the same level of radial head engagement of the OCD defect as that seen in grade 4 lesions (presence of loose body). With the majority of changes located in the anterior third of the radial head, it is likely that this portion is engaging the capitellum in midflexion, as evidenced by the cysts, blunting, and edema.

(A) Schematic diagram depicting the anterior portion of the radial head engaging a capitellar lesion in a position of midflexion. Grid lines represent radial head lesion, and black represents the capitellar incongruity in a Nelson grade 4 osteochondritis dissecans lesion. (B) Sagittal magnetic resonance imaging demonstrates the anterior radial head engaging a Nelson grade 4 capitellar osteochondritis dissecans lesion in elbow flexion. Images courtesy of Children’s Orthopaedic Surgery Foundation, 2017.
Regarding presentation, those with RHLs had more mechanical symptoms, although this difference was not statistically significant and may have been confounded by the fact that patients with RHLs were more likely to have grade 4 lesions with intra-articular loose bodies. It is difficult to clinically distinguish between locking from incarcerated loose bodies and engagement of the radial head into the capitellar defect. We did not appreciate a difference in pain or range of motion at presentation. Potential explanations for this finding include the relatively small sample size, lack of clinical symptoms associated with early-stage OCD and RHLs, or difficulties in distinguishing symptoms associated with the RHL versus the capitellar OCD. Therefore, careful radiographic inspection—particularly in fluid-sensitive MRI sequences—is needed to identify concomitant radial head changes.
The results following surgery further support the hypothesis that RHLs result from radiocapitellar incongruity and abnormal mechanics. Patients with RHLs who had OATS trended toward better motion and resolution of mechanical symptoms than did those who underwent drilling. In patients without RHLs, where articular incongruity may be less of an issue, clinical results did not differ. These findings suggest that in the presence of RHLs, it may be advantageous to perform reconstructive procedures that restore the normal convexity and articular congruity of the capitellum through osteochondral grafting rather than marrow stimulation techniques, which allow for fibrocartilage formation but do not restore the articular congruity of the capitellum as effectively. Note, however, that regardless of the surgery performed on patients with RHLs, all had minimal pain and had returned to sport by their most recent clinical visit.
We report on a relatively small cohort of patients, and larger studies should be performed to further assess the clinical and functional implications of this study’s findings. Further longitudinal investigation is needed to ascertain if radial head changes predispose to long-term stiffness, pain, and arthrosis. Bauer and colleagues 1 described radial head enlargement for 18 of 27 patients in a long-term follow-up of those with capitellar OCD, although there was no report on whether this subset of patients had a higher rate of degenerative joint disease. Additionally, long-term studies with follow-up MRI can allow us to assess resolution of RHLs on advanced imaging (Figure 5).

Sagittal fluid-sensitive magnetic resonance imaging. (A) Preoperative edema in the radial head (white arrow). (B) Same patient following osteochondral autograft transplantation surgery (OATS) with resolution of edema (white arrow) in the radial head after restoration of radiocapitellar articular congruity. Images courtesy of Children’s Orthopaedic Surgery Foundation, 2017.
Recognition of the concomitant radial head changes merits further investigation—including structural changes in the articular surface, radial head enlargement, engagement of the radial head within the capitellar defect, and radiocapitellar instability. If radial head changes portend a worse prognosis, greater efforts to restore a congruent capitellar surface should be made. As supported by the preliminary findings in this investigation, this would theoretically be better achieved with OATS rather than simple debridement and/or microfracture.
This study had a number of limitations. First, there was selection bias, as all patients were seen at a single tertiary-care referral center, which also likely explains the higher percentage of female patients in our study as compared with prior series. Additionally, there was no randomization of patients in determining the type of procedure that patients underwent (ie, OATS vs drilling), with a significant number of patients undergoing procedures other than OATS or drilling. We focused on OATS and drilling results, as these procedures best represented patients who underwent complete articular restoration and those who did not. This study also had a small sample size, with the possibility of a beta error, particularly in terms of short-term surgical results for patients who had RHLs and went on to OATS or drilling. There was also short-term follow-up for our patients who underwent procedures. However, our ongoing prospective longitudinal cohort study will allow us to further investigate the clinical impact of RHLs and their treatment in larger numbers of patients. Additionally, we had varied quality imaging; specifically, 1.5- versus 3.0-T MRI may have affected our ability to detect RHLs. Furthermore, not all patients had DESS sequences, which may have affected our ability to effectively measure capitellar OCD lesion size. This may explain why we did not see an association between greater capitellar OCD lesion size and the presence of RHLs. Last, there were challenges identifying and measuring sclerosis and other qualitative changes on MRI. More consistent imaging with higher-resolution MRI—even bioimaging techniques, such as dGEMRIC—may help elucidate the natural history of RHLs in capitellar OCD.
Conclusion
Edema, cysts, and/or blunting of the radial head is seen in nearly one-third of elbows with capitellar OCD. Lesions predominantly occurred in the anterior radial head of patients with more advanced capitellar lesions. Short-term clinical follow-up suggests better postoperative results with regard to range of motion and resolution of mechanical symptoms among patients with RHLs who were treated with OATS than with drilling. Further longitudinal investigation of larger numbers of patients is warranted to better understand the impact of these changes on elbow pain, motion, and function in the longer term. Efforts are underway to expand our prospective registry to multiple centers in hopes of answering these remaining questions.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.S.B. receives publishing royalties from Lippincott, Williams, & Wilkins; receives research support from the Pediatric Orthopaedic Society of North America; and is on the Clinical Education Medical Advisory Board of Orthopediatrics.
Ethical approval for this study was obtained from Boston Children’s Hospital (protocol No. IRB-P00011928).