
Abstract
Background:
The first-line treatment for patellar dislocations is often nonoperative and consists of physical therapy and immobilization techniques, with various adjuncts employed. However, the outcomes of nonoperative therapy are poorly described, and there is a lack of quality evidence to define the optimal intervention.
Purpose:
To perform a comprehensive review of the literature and assess the quality of studies presenting patient outcomes from nonoperative interventions for patellar dislocations.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The MEDLINE, AMED, Embase, CINAHL, Cochrane Library, PEDro, and SPORTDiscus electronic databases were searched through July 2017 by 3 independent reviewers. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed. Study quality was assessed using the CONSORT (Consolidated Standards for Reporting Trials) criteria for randomized controlled trials and the Newcastle-Ottawa Scale for cohort studies and case series.
Results:
A total of 25 studies met our inclusion criteria, including 12 randomized controlled trials, 7 cohort studies, and 6 case series, consisting of 1066 patients. Studies were grouped according to 4 broad categories of nonoperative interventions based on immobilization, weightbearing status, quadriceps exercise type, and alternative therapies. The most commonly used outcome measure was the Kujala score, and the pooled redislocation rate was 31%.
Conclusion:
This systematic review found that patient-reported outcomes consistently improved after all methods of treatment but did not return to normal. Redislocation rates were high and close to the redislocation rates reported in natural history studies. There is a lack of quality evidence to advocate the use of any particular nonoperative technique for the treatment of patellar dislocations.
A patellar dislocation is a debilitating injury typically associated with the younger population, with incidence rates of primary dislocations varying from 29 to 43 per 100,000 in adolescents. 17,33 Acute dislocations often occur as a result of noncontact twisting injuries and frequently result in a loss of activity. 6,31 Recurrent dislocations may occur in a high proportion of patients (estimated as up to 50% 52 ), and current evidence for the best treatment modality (operative vs conservative [nonoperative] management) remains controversial, with a recent Cochrane review suggesting the need for more high-quality trials. 52
Management principles for patellar dislocations are based around strengthening or reconstructing the stabilizing elements of the patellofemoral joint. In a patellar dislocation, the medial patellofemoral ligament (MPFL) is often disrupted. 16 This ligament is the primary medial static stabilizer of the patella, with in vitro lateral translation increasing by 50% when deficient. 15,19 This may explain why recurrent instability often presents after an initial traumatic dislocation. 17,31,54 A high proportion of patients also have predisposing anatomic abnormalities, such as patella alta, trochlea dysplasia, and quadriceps dysplasia, which may increase the risk of ongoing instability. 14 While a large body of literature has focused on the results of surgical outcomes, the potential benefits of nonoperative treatment are much less well understood or documented. 28
Nonoperative management has formed an integral part of treating primary and recurrent dislocations. It is often considered to be the first-line treatment for patellar instability. 12,59 One of the challenges around nonoperative management is the complexity of the interventions offered and the different approaches to rehabilitation taken in different centers. Various physical therapy techniques have been described with the aims of strengthening the quadriceps muscles; restoring range of movement; addressing deficiencies in hip, trunk, or foot biomechanics that may precipitate instability; reducing pain; and improving patient confidence. 7,10,48 Different methods of immobilization have also been used in the acute phase, and this also remains controversial. There are little data to determine which regimen is best or even what approaches are most commonly used in practice.
Few and poor-quality studies have meant that previous systematic reviews have failed to find robust evidence to suggest optimal nonoperative treatment regimens or even to determine whether current approaches to nonoperative management (such as physical therapy) have any effect on outcomes. 50,51,57 The aim of this review was to define clinical outcomes after the nonoperative management of both first-time and recurrent patellar dislocations and to explore the variability in practice within the literature.
Methods
Data Source/Search
Electronic databases that were searched included AMED, Embase, MEDLINE, CINAHL, Cochrane Library, PEDro, and SPORTDiscus (database inception to July 2017). Gray literature was also searched using Open Grey, National Technical Information Service, UK Clinical Trials Gateway, Cochrane Central Register of Controlled Trials, WHO International Clinical Trials Registry Platform, UKCRN Portfolio Database, and ClinicalTrials.gov. Conference proceedings were searched using the Web of Science database. All search strategies, MeSH terms, and keywords used for major databases can be found in Appendix 1.
Eligibility Criteria
All studies with evidence level 1 to 4 were included if patient-reported outcome measures (PROMs) were presented for patients with primary or recurrent lateral patellar dislocations for which the treatment was nonoperative. Single-patient case reports, animal studies, cadaveric studies, studies on nonnative knees, non–English language studies, and studies in which patient-reported outcomes were not presented were excluded at the final stage of screening. Studies reporting outcomes of physical therapy, which was provided in conjunction with surgical interventions, were excluded. If the results for the nonoperative arm of studies reporting both operative and nonoperative management could not be identified and separated, then these were also excluded.
Study Screening
The Covidence platform was used to help organize first-stage and second-stage screening. 13 Three reviewers were involved in the second stage of full-text screening (M.M., N.S., A.C.). Full-text articles for all studies included in the data analysis were requested. Any disagreements on study inclusion/exclusion were resolved through a discussion between the 3 reviewers and if necessary through arbitration by the senior reviewer (A.M.). This was not necessary.
Data Extraction
Data were extracted onto a spreadsheet for intervention type, study demographics, and outcomes that had been designed by mutual agreement by the authors before the extraction process. Study demographics included study design, type of dislocation, number of patients, mean age, sex, follow-up period, and treatment given. Clinical outcomes extracted were PROM scores, redislocation rates, and operation rates.
Critical Appraisal
A critical appraisal of study quality was conducted using the Newcastle-Ottawa Scale (NOS) 60,61 for cohort studies (modified for case series by the removal of questions regarding Selection [Section 2] and Comparability) and for randomized controlled trials (RCTs) using the CONSORT (Consolidated Standards of Reporting Trials) criteria. 42
Data Analysis
Because of the significant heterogeneity in study characteristics and methodology, pooling of data for statistical analysis was not deemed possible. Analysis of data was therefore performed through a narrative analysis of the evidence. The modality of treatment given was used to categorize studies. Where possible, studies were grouped by common treatments, or themes to assess for patterns in the literature or common approaches to treatment. In RCTs in which both operative and nonoperative data were presented, only the nonoperative data were assessed.
Results
Search Strategy
Overall, 25 studies were found eligible for inclusion with 1066 patients (Figure 1 and Table 1). Of these studies, 12 were RCTs ∥ (only the abstract was available for one 45 ), 7 were cohort studies, 1,3,9,10,32,47,48 and 6 were case series. 25,29 –31,41,58

PRISMA flowchart. NTIS, National Technical Information Service.
Study Characteristics a

a GQ, general quadriceps; RCT, randomized controlled trial; VMS, vastus medialis–specific.
b Same patient population.
c Data only for nonoperative study population.
d Same patient population.
e Some study information not provided in article (author could not be contacted).
Critical Appraisal
Compliance with CONSORT criteria for RCTs exceeded 70% in 7 of 11 studies. Four studies randomized both groups to nonoperative interventions. 2,39,45,49 Significant methodological weaknesses existed in the literature; information specifying the randomization protocol was lacking (eg, failing to specify who performed the random allocation sequence and enrolled/assigned participants) in up to 9 studies, ¶ 4 studies provided insufficient information regarding the interventions to permit replication, 2,7,35,46 4 did not specify the location of the population recruited, 7,24,38,46 3 studies provided no evidence for how the sample size was estimated (ie, showed no power calculations), 24,34,35 and 1 did not outline the follow-up period. 7 Only 3 studies satisfactorily reported CIs, making an assessment of the effect size difficult. 24,34,49
Adequate control for differences in patient demographics (eg, age and sex) and population size was missing in 6 of the 7 cohort studies. 1,9,10,32,47,48 A follow-up rate of over 80% was not achieved by 3 cohort studies. 10,32,48 The modified NOS for case series revealed that 1 case series failed to meet an adequate follow-up. 31 Vengust et al 58 failed to make a statement on follow-up rates, provided no description of the population that was derived, and did not outline how the intervention results were ascertained. Total CONSORT, NOS, and modified NOS scores are outlined in Appendix 2.
Furthermore, there were missing data from many studies, especially regarding the type of intervention used and presence of anatomic variants such as trochlea dysplasia, patella alta, and tibial tubercle–trochlear groove distance.
Population Characteristics
There was substantial heterogeneity among studies in terms of population size, patient age, and sex (Table 1). The majority of studies included patients of all age groups. However, only 3 studies focused on a pediatric population. 1,32,36 Fourteen of the 21 studies that provided demographic information had more male patients than female patients. Follow-up periods varied from 1 week to 19 years. Only 2 studies specifically analyzed patients with recurrent dislocations. 3,58
Nonoperative Treatments and Outcome Measures
Various nonoperative interventions have been reported (Appendix 3). These can be broadly categorized into 4 groups: (1) studies immobilizing or not immobilizing the knee using casts or braces; (2) full weightbearing versus partial weightbearing; (3) using generalized quadriceps (GQ) exercises versus vastus medialis–specific (VMS) exercises; and (4) studies using various other physical therapy techniques, for example, proprioceptive exercises, closed chain/open chain exercises, and electrostimulation.
A range of PROMs were reported, including the Lysholm score, 27 Tegner scale, 55 Kujala score, 26 Hughston score, 18 Knee injury and Osteoarthritis Outcome Score, 40 Norwich Patellar Instability score, 53 and the Modified Functional Index Questionnaire and Minnesota Activity Scale. 43,44 The most commonly used PROM was the Kujala score (15 studies), followed by the Lysholm score (6 studies). Some studies included more than 1 PROM.
As a measurement of treatment failure, the redislocation rate was another commonly reported outcome, despite operation rates only being provided in 7 studies (Table 2).
Study Outcomes a

a FROM, free range of movement; GQ, general quadriceps; IQR, interquartile range; KB, knee brace; KOOS, Knee injury and Osteoarthritis Outcome Score; NPI, Norwich Patellar Instability score; PROM, patient-reported outcome measure; PSO, patellar stabilizing orthosis; RROM, restricted range of movement; VMS, vastus medialis–specific.
b Same patient population.
c Same patient population.
d Some study information not provided in article (author could not be contacted).
e Data presented in the study for dislocations only for a subset of a total 16 nonoperative patients (14 patients with 1 predisposing factor).
Overall Outcomes
The pooled redislocation rate from the 21 studies that reported redislocations was 31% (16% at 2 years), with a mean follow-up period of 4 years. PROM scores are presented in Table 2. There was some variation in outcome scores, as might be expected from the heterogeneous group of studies that were included. The lowest mean Kujala score was 69, and the highest was a median of 93, with a mean of 82.7 if all patients are included. 10,45 The Lysholm scores were more consistent; the lowest score (excluding the 3-month follow-up for Armstrong et al 2 ) was a mean of 85, and the highest was 89.3, 3,58 with an overall mean of 86.3.
Immobilization Versus No Immobilization
With the exception of those studies dealing with the same patient population, 29,30,34 –36 there was no consensus between studies on the intervention protocol. All but 4 studies employed some form of immobilization. 3,41,48,58 Some studies utilized immobilization (using various braces/splints/orthoses/casts) for up to 3 weeks, 10,24,29,30,36,54 while others immobilized for 4 weeks or longer. 2,39
Knee Braces
Braces described by the studies included patellar stabilizing orthoses (PSOs), which are designed to maintain the patella in the femoral groove after a dislocation, knee extension braces, and range of movement braces. When comparing outcome data for those studies in which immobilization using a PSO (7 studies) was used compared with an alternative knee brace (10 studies), there appeared to be a trend toward higher PROM scores with a PSO (mean Kujala score for studies using a PSO was 88.3 compared with 80.5 for other braces) 11,36 (Table 2). Other braces used were a knee extension brace, 8 which applies a dynamic load in extension, and range of movement braces, 38 which allow range of motion control and can be locked at different degrees of flexion. Eight studies did not specify the type of knee brace. 2,11,24,25,30,31,41,45 The redislocation rate for the PSO group was 42.5% at 8.5 years of follow-up compared with 22.4% at 2.5 years in the alternative brace group. Given the differences in the length of follow-up, it was therefore difficult to draw conclusions based on these data.
Taping Versus Cast Immobilization
One RCT assessed taping versus cast immobilization. Rood et al 39 (N = 18) noted significantly improved Lysholm scores at 12 weeks (median difference, 36; P < .05) and 5 years (median difference, 24; P < .01) after the injury in a nonimmobilized group with tape applied compared with an immobilized group with a cast, but their sample sizes were very small. There were no cases of redislocations in either group at 5-year follow-up.
No Immobilization Versus Cast Immobilization
One study assessed no immobilization versus cast immobilization. Armstrong et al 2 conducted a feasibility RCT randomizing patients to 4 weeks of cylinder cast immobilization or no immobilization. Eight patients were randomized, and no statistics were performed by the authors because of the small sample size; however, a suggestion was made for a trend toward improved short-term functional results (Lysholm scores) in patients not immobilized. 2 Redislocation rates were not reported.
Weightbearing Versus No Weightbearing
Seven studies outlined weightbearing status. Two studies specified partial weightbearing. 24,38 The mean Kujala scores in studies reporting full weightbearing and partial weightbearing were 86.7 and 80.7, respectively. The redislocation rate for partial weightbearing (37.5%) 37 was within the range of redislocation rates for full weightbearing (7.1%-71%) and was similar to the overall pooled redislocation rate of 31%.
GQ Exercises Versus VMS Exercises
Fourteen studies implemented GQ exercises, 2 described a combination of GQ and VMS exercises, while 2 focused on VMS exercises (Table 2). Of note, an RCT by Smith et al 49 of 50 patients with a first-time patellar dislocation observed statistically significant differences in Lysholm scores between a GQ exercise group and a VMS exercise group (GQ better than VMS) (95% CI, –14 to 0.0; P = .05) at 12 months, without reaching a clinically significant difference.
Outcomes in Studies Using Proprioceptive Exercises, Closed/Open Chain Exercises, and Electrostimulation
Because of the limited number of studies implementing proprioceptive exercises, closed/open chain exercises, and electrostimulation, 1,2,7,48,58 these studies were assessed alone. Studies using proprioceptive exercises reported Lysholm scores of between 70 and 89.3 at follow-up. 2,7,58 Bitar et al 7 evolved closed chain to open chain exercises, while Sillanpaa et al 48 used both concurrently; redislocation rates were 35% and 54.8%, respectively, 7,48 compared with the pooled redislocation rate of 31% from all studies. The 2 studies implementing electrostimulation used different PROMs: Bitar et al 7 used the Kujala score, and Armstrong et al 2 used the Lysholm score. Furthermore, redislocation rates could only be gathered from Bitar et al, 7 making qualitative comparisons difficult.
Discussion
Nonoperative treatment is a common management option for lateral patellar dislocations 12,59 and is widely used in the case of a first-time patellar dislocation. It is also commonly used for patients with more than 1 dislocation, and many authors do not advocate surgical treatment until a course of nonoperative treatment has been deemed to have failed. 12,59 One of the main findings of this systematic review was that mean PROM scores after nonoperative treatment were high on the whole but did not represent normal function in any of the studies, 38 with the Kujala score and the Knee injury and Osteoarthritis Outcome Score in the larger series mostly approximating 80% of the maximum score.
None of the studies reviewed had a “no intervention” control group, and so it was not possible to comment on the overall effectiveness of the treatments that were presented as compared with the true natural history of the condition. PROM scores improve in many acute musculoskeletal conditions over time, and research is needed to determine whether physical therapy is effective compared with no active treatment and the passage of time. 4,5,56 One included study found no difference in PROM scores between the group that had no further dislocations and the group that had recurrent dislocations after their course of rehabilitation. 31 These authors also found that although PROM scores improved, only 26% of patients who had no further dislocations were able to return to sports without limitation.
Only 2 studies investigated patients with recurrent dislocations. 3,59 This population presents with a more challenging problem and may have different pathoanatomic processes as well as potential differences in behavior and responses to outcome surveys through different health beliefs and experiences compared with patients with a first-time dislocation. 53 These studies should be considered in this context. Nonetheless, it is important to note that there remains a paucity of evidence on how to manage the recurrent dislocation population, particularly on when nonoperative management has been exhausted and when surgical interventions may be deemed appropriate. This remains a key research priority.
Redislocation rates were high for most of the included studies, which is similar to the reported natural history of patellar dislocations. 17,20 Without direct comparative studies, it is not clear whether the interventions used (including physical therapy) are able to reduce the rate of redislocations. However, large reductions in redislocations after physical therapy were not shown. Both treating health care professionals and patients should be aware of the rates of redislocations after nonoperative treatment.
Redislocation rates were highly variable between studies, probably reflecting the multiple differences in the studies analyzed, with different populations and lengths of follow-up in particular. The importance of this time to follow-up was well demonstrated by the long-term follow-up data of Palmu et al 36 (where at 14 years, the redislocation rate was 71%, although in a small cohort), and differences in the population are important to consider, as the influence of age at first dislocation is known to have a major influence on the risk of further dislocations. 23 Trochlea dysplasia and patella alta are also known to influence the risk of further dislocations but were not assessed by the studies in this review. There was no clear advantage of any nonoperative treatment in reducing redislocation rates in the studies analyzed.
Nonoperative management is theorized to optimize the neuromusculoskeletal system by achieving dynamic stability through the recruitment of muscle groups including the glutei, quadriceps, hamstring, and calf complex. 50,52 Nonoperative management is also hypothesized to promote successful healing of the MPFL, which could translate to reduced recurrent dislocation events and improved clinical outcomes. 50,52 The relative importance of MPFL healing and improved neuromusculoskeletal control in preventing further dislocations is not known.
Unfortunately, the current evidence poorly reports the interventions prescribed as part of a nonoperative intervention. It remains unclear whether the nonsuperiority of one immobilization or rehabilitation program over another is attributable to an insufficient type and dosage of physical therapy (in relation to intervention provided, frequency, and loading of exercises or duration of immobilization) or a lack of efficacy from the interventions or research methodology, which is not able to differentiate between them (eg, a large randomized trial). Future randomized trials are therefore required to clearly report nonoperative interventions with reporting checklists such as the template for intervention description and replication checklist to overcome this problem. 22
There was a wide variation in intervention programs. With the paucity of literature evaluating each specific program, it remains unclear whether there is superiority between them. A review in 2010 was unable to reach a consensus on the best intervention program. 50 Similarly, we have also been unable to identify either a preferred strategy or even a common pattern of treatment in the literature. Four RCTs have been conducted since the time of the 2010 review. 2,39,45,49 Significant weaknesses in these RCTs preclude definitive conclusions. Smith et al 49 noted a statistically significant difference in Lysholm scores between GQ exercises compared with VMS exercises (GQ better than VMS) without reaching clinical significance. This may be a promising avenue for further inquiry if a suitably powered study can be conducted. 49 The use of a PSO also showed promising results, although redislocation rates were similar, and may be an area for further study. 36 Pilot and feasibility studies have suggested that there may be a trend toward better results when patients are not immobilized after a dislocation, but these studies are very small, and a much larger trial is needed to determine whether this is the case.
Based on the current evidence, there is a justification for early active rehabilitation, particularly with approximately 60% of patients demonstrating improvements in functional outcomes. However, a research priority should be to determine the best practice rehabilitation pathways to optimize the recovery of these patients. A better understanding of the subgroups of the patellar dislocation population is required to determine what types of rehabilitation pathways should be adopted and which patients should be considered as surgical candidates.
There are 4 key limitations to this review. Foreign language articles were excluded because of the costs associated with translation, which may therefore have introduced publication bias. Second, the included studies poorly reported PROMs. A future research priority should be to develop a core set of outcomes, which may include repeated dislocations and adverse events, functional outcomes (as measured with the Kujala score 26 ), patellar instability (as measured with the Norwich Patellar Instability score 53 or Banff score 21 ), and quality of life as possible domains. Third, the absence of normative data on the Kujala score or Lysholm score in this population makes interpretations of the clinical significance of the findings challenging. Finally, the current evidence base remains focused on male patients, particularly male military recruits and those with more physically demanding occupations or pursuits. Future research should aim to assess this abnormality in more typical community-based cohorts rather than military cohorts, which may not represent the typical patient.
To conclude, this systematic review showed that PROM scores consistently improve after the nonoperative management of patellar dislocations, but they do not return to their preinjury function, and the pooled redislocation rate was 31%. The treatment of patellar instability in the literature is highly variable, and there is no definitive evidence to inform the optimal intervention regimen. Health care professionals and patients should be aware of the risk of recurrent or ongoing instability with the nonoperative management of patellar dislocations.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: T.O.S. is supported by funding from the National Institute for Health Research (NIHR) Oxford Health Biomedical Research Centre.
Note
Appendix 1 Search Strategies and Terms
Appendix 2

Appendix 3
Nonoperative Interventions a

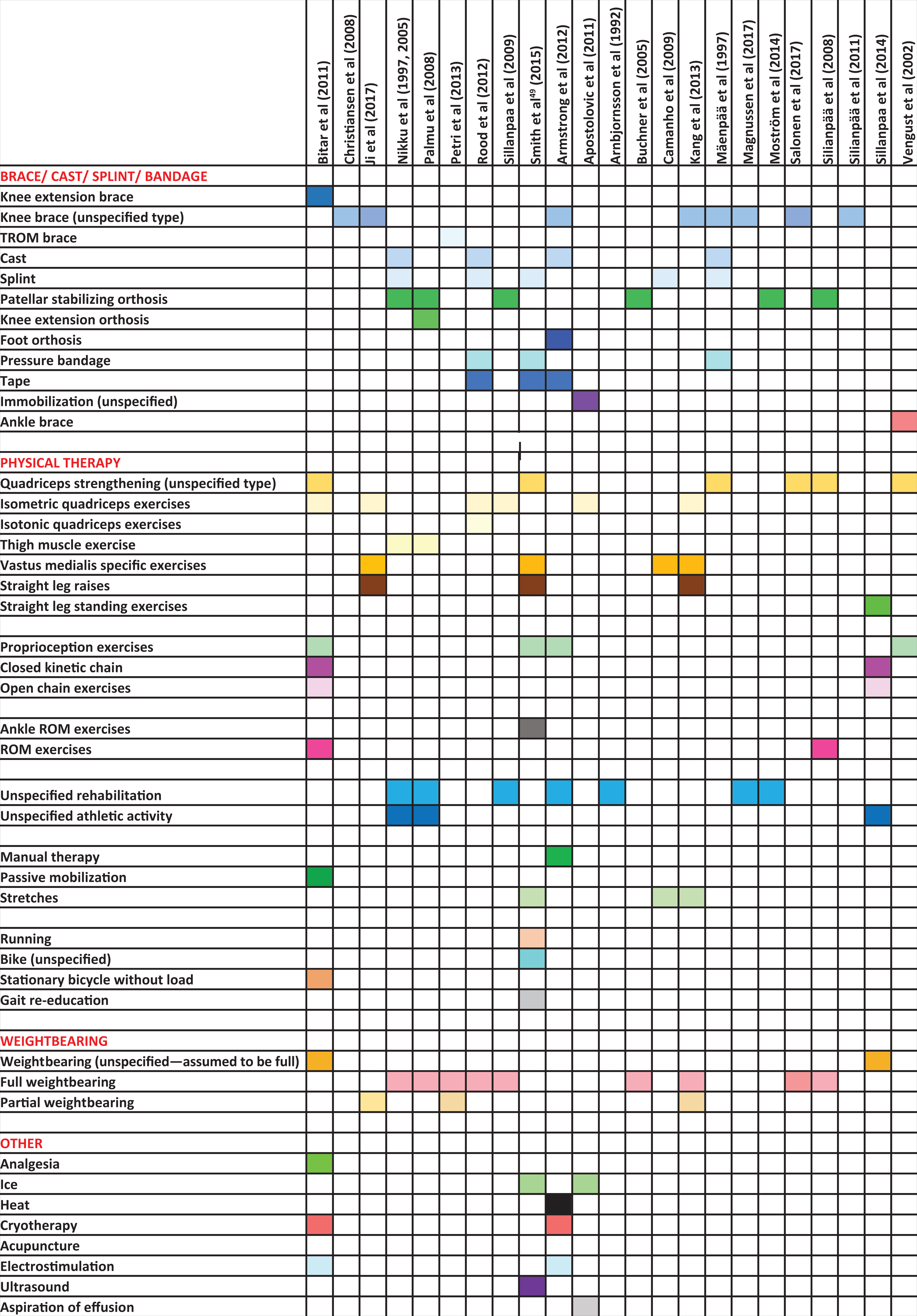
|
a TROM, total range of motion; ROM, range of motion.