
Abstract
Background:
There is insufficient knowledge regarding the influence of concomitant injuries on the recovery of short-term subjective knee function after anterior cruciate ligament (ACL) reconstruction.
Purpose:
To determine whether patient characteristics, concomitant injuries, and graft choice during ACL reconstruction can predict which patients achieve acceptable knee function 1 year after reconstruction.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Data from 1 physical therapist–specific and 1 surgeon-specific register were used. Patients who had completed the Knee injury and Osteoarthritis Outcome Score (KOOS) at 1-year follow-up were included. Additional intraoperative information was extracted from a database. The primary outcome was achieving a patient-acceptable symptom state (PASS) for each subscale of the KOOS. Univariable and multivariable logistic regression models were used, with patient sex, age, and preinjury level of physical activity as covariates.
Results:
A total of 343 patients (51% females) were included. The proportion of patients achieving PASS 1 year after ACL reconstruction varied between 40% and 85% among the KOOS subscales. Younger age at reconstruction and male sex provided favorable odds of achieving acceptable knee function across the KOOS subscales. Patients without cartilage injury had increased odds of achieving PASS in the KOOS sport and recreation subscale; the increase was 1.63-fold (95% CI, 1.01-2.64; P = .045). Patients receiving patellar tendon autograft had a 0.41-fold (95% CI, 0.19-0.85; P = .017) decrease in odds of achieving PASS on the KOOS quality of life (QoL) subscale. In the multivariable analysis, increased odds of achieving PASS on the KOOS QoL subscale were associated with the absence of meniscal injury (odds ratio, 1.62; 95% CI, 1.04-2.54; P = .035), and increased odds were found for hamstring tendon autograft (OR, 2.63; 95% CI, 1.25-5.56; P = .011).
Conclusion:
More than half of the patients reported an acceptable symptom state on 4 of the 5 KOOS subscales 1 year after ACL reconstruction. A lack of consistency was noted related to the effect of concomitant knee injuries and graft choice on acceptable knee function. However, younger age and male sex were favorable, nonmodifiable characteristics that increased the odds of early acceptable function.
A large proportion of anterior cruciate ligament (ACL) injuries occur with concomitant injuries to other structures in the knee joint, such as the menisci, collateral ligaments, and articular cartilage. 4 Large-scale studies using information from the Scandinavian knee ligament registers have shown that patients with concomitant meniscal or articular cartilage injuries report inferior short-term knee function after an ACL reconstruction compared with patients with isolated ACL tears, regardless of the severity and treatment received for concomitant injuries. 2,13,25 These reports, however, have not considered potential confounding factors such as age, patient sex, preinjury level of physical activity, recovery of muscle function, and graft choice. 1,10,26 In addition, the presence of concomitant medial collateral ligament injuries has seldom been accounted for in trials assessing subjective knee function, even though these injuries have been reported to increase the time to return to sport. 3,15 Thus, a variety of factors may influence a patient’s perception of acceptable knee function after surgery, and current knowledge regarding these factors is limited.
Patient-reported outcome (PRO) should be regarded as a cornerstone in every evaluation in medical research, as the measure highlights the patient’s perception of treatment. However, the results can be difficult for the clinician to understand and interpret. A clinically meaningful change in PRO may not be associated with an acceptable state corresponding to “feeling well.” The patient-acceptable symptom state (PASS) 30,31 provides a reference value at which a majority of a population feel well, and this value can elucidate how concomitant injuries and graft choice affect the recovery of subjective knee function after ACL reconstruction.
The purpose of this study was to determine the proportion of patients who perceive an acceptable level of knee function 1 year after ACL reconstruction and to determine which patient demographics, concomitant injuries, and graft choice may influence this. The null hypothesis was that patient demographics, concomitant injuries, and graft choice would not be predictive of PASS in the Knee injury and Osteoarthritis Outcome Score (KOOS) 1 year after ACL reconstruction.
Methods
The present cohort study was based on prospectively collected data from 2 registers: 1 physical therapist–specific and 1 surgeon-specific. The physical therapist–specific register, Project ACL, is a rehabilitation register established in September 2014. 12 Project ACL uses a web-based platform for regular assessment with PROs and tests of muscle function for patients who have sustained an ACL injury. Assessments are performed at a predefined schedule after ACL injury or reconstructive surgery. Preoperative assessments are performed if the patient is registered in the project before undergoing surgery. The battery of tests of muscle function is performed according to a predefined protocol and consists of 2 parts evaluating knee strength and hop performance. 11,21 At the start of the project, isometric strength tests were performed by use of the David F200 DMS-EVE (David Health Solutions Ltd), and these values contributed to 35% of the total muscle strength data. The isometric test evaluated peak torque in knee extension at 60° of knee flexion and knee flexion at 30° of flexion. From December 2015 onward, strength tests have been performed with an isokinetic concentric test of knee extension and knee flexion at 90° per second by use of a Biodex System 4 (Biodex Medical Systems). 32 Hop tests include the single-leg hop for distance, vertical jump (Muscle Lab; Ergotest Technology), and side-hop test. All the hop tests are performed with the patients holding their hands behind their back, and the best of 3 attempts is recorded. The side-hop test is performed by the patients jumping as many times as possible over two lines 40 cm apart for 30 seconds.
The Swedish National Knee Ligament Register (SNKLR) is a nationwide database that uses a web-based protocol for the collection of data. 2,13 The protocol consists of 2 parts: one surgeon-reported section and one patient-reported section. The operating surgeon enters information about the physical activity performed at the time of injury, time from injury to reconstruction, graft selection, and surgical fixation techniques. The data on previous surgery in the reconstructed knee, the contralateral knee, and all concomitant injuries are also registered. All surgical procedures performed on the injured knee, including meniscal surgery and treatment for chondral lesions, are reported. The patient-reported section includes scores on the KOOS and the European Quality of Life Five Dimensions (EQ-5D) preoperatively and at 1, 2, 5, and 10 years after ACL reconstruction. The coverage (proportion of participating units in relation to all eligible units) and completeness (proportion of target population in the registry) are 93% and more than 90%, respectively, with a 50% to 70% response rate on the PRO measurements. 7
Patients
Patients registered in Project ACL who had 1-year follow-up data on PROs were eligible for inclusion. For the identified patients, additional intraoperative and surgical information was extracted from the SNKLR, including data on concomitant injuries and graft choice. Only patients who underwent primary unilateral ACL reconstruction and had no previous knee surgery were included in the study. Patients were excluded if they had an early postoperative infection. Those who sustained a graft rupture or contralateral ACL injury were not considered, as they would not be eligible for the 1-year follow-up in Project ACL. All patients were given written information about the study, and informed consent was obtained. Ethical approval was obtained from the regional ethical review board in Gothenburg, Sweden.
Outcome
The primary outcome of the study was the achievement of PASS for each subscale of the KOOS, 20 with an additional analysis of KOOS4. KOOS data were extracted from the physical therapist register. The KOOS subscales are composed of pain, knee-related symptoms, activities of daily living (ADL), function in sport and recreation, and knee-related quality of life (QoL). The KOOS4 is an average score of 4 KOOS subscales, in which the subscale ADL is excluded to avoid a ceiling effect, as relatively young and active patients rarely have difficulties with function in daily living. 9 Each item on the KOOS is scored from 0 (no problem) to 4 (extreme problem) on a 5-point Likert scale. 24 Scores from each subscale are transformed to a 0-100 scale, with zero representing “extreme knee problems” and 100 representing “no knee problems.”
The achievement of PASS on the KOOS was assessed by the threshold values suggested by Muller et al. 20 These values were established by asking the following question of patients who had undergone ACL reconstruction: “Taking account of all the activity you have during your daily life, your level of pain, and also your activity limitations and participation restrictions, do you consider the current state of your knee satisfactory?” 16,31 The corresponding PASS values for the KOOS subscales are as follows: pain ≥ 88.9, symptoms ≥ 57.1, ADL = 100, sport and recreation ≥ 75.0, and QoL ≥ 62.5.
Statistics
Statistical analysis was performed with the SAS statistical analysis system (SAS/STAT, v 14.2; SAS Institute). Descriptive statistics for patient demographics and outcomes are reported as counts and proportions for categorical variables. Continuous variables are reported as means ± SDs 23 and medians with first and third quartiles. For comparisons between included and excluded patients, the Fisher exact test (lowest 1-sided P value multiplied by 2) for dichotomous variables and the Mann-Whitney U test for continuous variables were performed.
Binary logistic regression was performed to analyze the association between intraoperative variables and achieving PASS on the KOOS subscales. The PASS cutoff value for each KOOS subscale was used separately as a dependent variable. The presence of concomitant injuries was used dichotomously as an independent variable in the regression. Graft choice compared hamstring tendon (HT) and patellar tendon (PT) autografts. Patient demographics relating to patient sex, age (per 10-year increments), and preinjury level of physical activity, as measured with the Tegner activity scale, 28 were also included as independent variables. Logistic regression models were performed with fixed adjustments of previously known potential patient demographic confounders: age at index reconstruction, patient sex, and preinjury level of physical activity. The results of the logistic regression models are presented with odds ratios (ORs), 95% CIs, and P values. OR is expressed for every 1-unit increase in the predictor variable, with the exception of age (per 10 year of age). The area under the receiver operating characteristic curve (AUC) was given as a measurement of goodness of fit, using limits of 0.90-1 = excellent, 0.80-0.90 = good, 0.70-0.80 = fair, 0.60-0.70 = poor, and 0.50-0.60 = fail. 17
A continuous linear regression was performed to analyze the KOOS4. Normality in the KOOS4 was checked by use of histograms. As with the logistic regression models, the linear regression was performed after adjustment for patient demographics. The results of the linear regression are reported with beta estimates, 95% CI, and P values. The R 2 is given as a measurement of the goodness of the model. All regression models are reported as forest plots and additional detailed tables (Appendix Tables A1-A6).
Finally, to find the best predictive model for achieving PASS for all dependent KOOS subscales, a stepwise multivariable logistic model was used, while a multivariable linear regression model was used for the KOOS4. Multivariable analyses were performed for all KOOS subscales that had a significant outcome in the univariable analyses, with patient demographics as covariates. Predictors with P < .20 were entered into the stepwise analyses. All significance tests were 2 sided and were conducted at the 5% significance level.
Results
A total of 343 patients fulfilled the final inclusion criteria and were eligible for the study. The number of ineligible patients according to exclusion criteria is presented in Figure 1. Patient demographics and a dropout analysis are presented in Table 1. No differences were found between the included and excluded patients. Results at 1-year follow-up for Tegner scores and muscle function are reported in Table 2, and KOOS and PASS outcomes are reported in Table 3. The proportion of patients achieving PASS varied among the KOOS subscales: KOOS pain, 57%; KOOS symptoms, 85%; KOOS ADL, 40%; KOOS sport and recreation, 52%; and KOOS QoL, 50%.

Patient inclusion and exclusion. ACL, anterior cruciate ligament; KOOS, Knee injury and Osteoarthritis Outcome Score; SNKLR, Swedish National Knee Ligament Register.
Baseline Data and Dropout Analysis a

a For categorical variables, n (%) is presented. For continuous variables, the mean ± SD, median (Q1; Q3), and sample size are presented. For comparisons between groups, the Fisher exact test (lowest 1-sided P value multiplied by 2) was used for dichotomous variables, and the Mann-Whitney U test was used for continuous variables. ACL, anterior cruciate ligament; BMI, body mass index.
Outcomes at 1-Year Follow-up a

a For categorical variables, n (%) is presented. For continuous variables, the mean ± SD, median (Q1; Q3), and sample size are presented. LSI, Limb Symmetry Index.
Outcomes at 1-Year Follow-up: KOOS and PASS a

a For categorical variables, n (%) is presented. For continuous variables, the mean ± SD, median (Q1; Q3), and sample size are presented. ADL, activities of daily living; KOOS4, 4 of the 5 KOOS subscales (with the ADL subscale excluded); PASS, patient-acceptable symptom state.
Patient Demographics
For each progressive 10-year increase in age, patients had significantly reduced odds of achieving PASS on all KOOS subscales, including KOOS4, with the exception of KOOS symptoms. The significantly reduced odds for older patients varied between 0.71 and 0.75 (Appendix Tables A1-A6), which also can be expressed as increased odds for younger patients to achieve PASS, equivalent to an OR of 1.33 to 1.41. Similarly, male patients had increased odds compared with females of achieving PASS across the KOOS subscales with the exception of KOOS symptoms, where no difference was observed. Patients with a higher level of preinjury physical activity had increased odds of achieving PASS on the KOOS ADL (OR = 1.11; 95% CI, 1.00-1.23; P = .043), sport and recreation (OR = 1.21; 95% CI, 1.09-1.34; P = .0003), and QoL (OR = 1.21; 95% CI, 1.09-1.34; P = .0003) but no effect was seen on the KOOS pain subscale, symptoms subscale, or the KOOS4.
PASS for KOOS Pain
None of the intra-articular concomitant injuries were associated with achieving PASS on the KOOS pain subscale. Patients without concomitant medial collateral ligament (MCL) injury had a 3.05 (95% CI, 1.04-8.98; P = .043) odds of PASS for KOOS pain. However, in the adjusted analysis, patients who underwent ACL reconstruction with HT autograft had higher odds of achieving PASS for KOOS pain compared with patients who received PT autograft (OR = 0.44; 95% CI, 0.22-0.90; P = .026) (Figure 2).
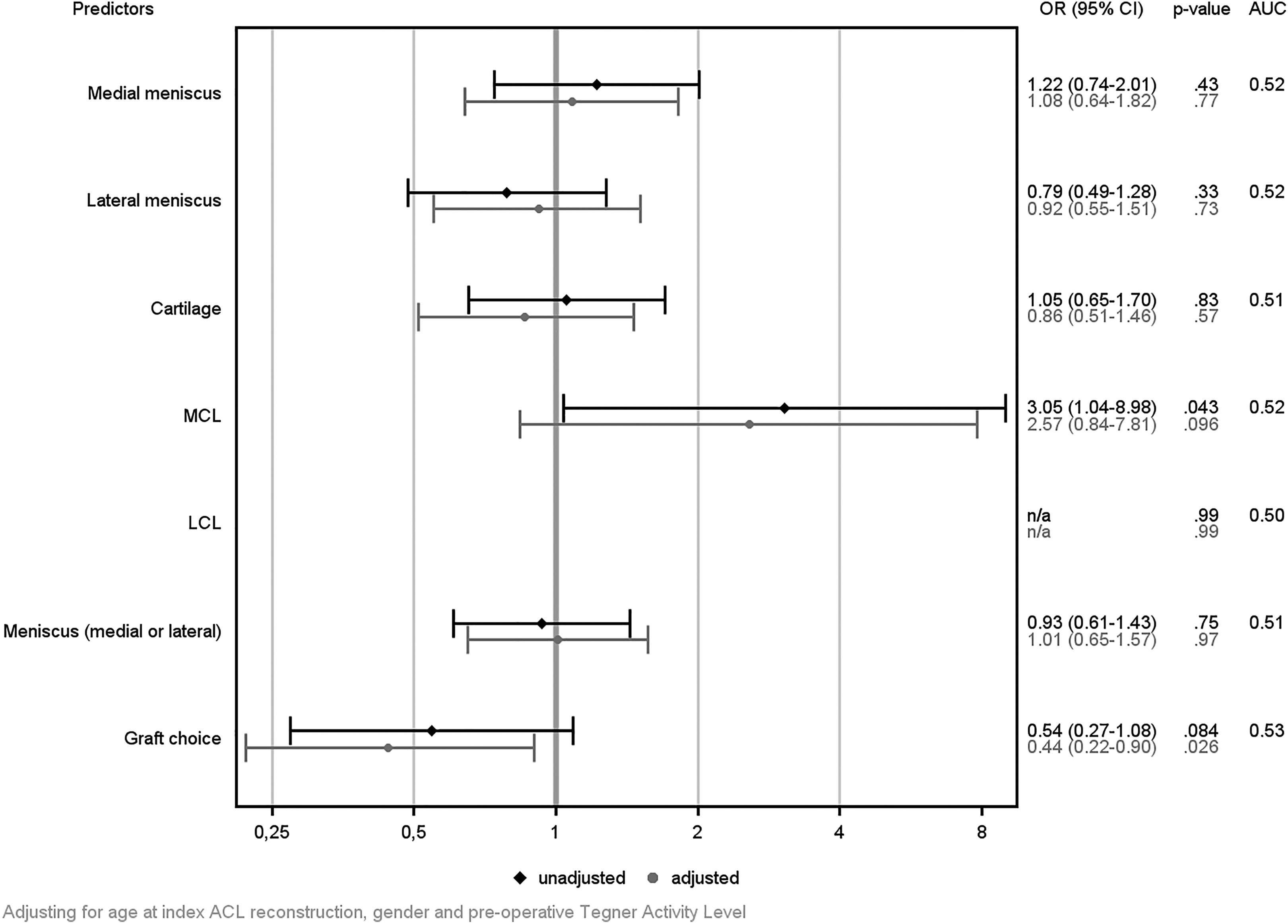
Unadjusted (black) and adjusted (gray) odds ratios (ORs), 95% CIs, and area under the receiver operating characteristic curve (AUC) for a patient-acceptable symptom state on the Knee injury and Osteoarthritis Outcome Score pain subscale. An OR >1 indicates a result favoring the absence of concomitant injury. For graft choice, an OR <1 indicates a result favoring a hamstring tendon autograft and an OR >1 favors a patellar tendon autograft. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; n/a, not applicable.
PASS for KOOS Symptoms
No intraoperative predictor was found to be statistically significant when attempting to predict the achievement of PASS on the KOOS symptoms subscale (Figure 3).

Unadjusted (black) and adjusted (gray) odds ratios (ORs), 95% CIs, and area under the receiver operating characteristic curve (AUC) for a patient-acceptable symptom state on the Knee injury and Osteoarthritis Outcome Score symptoms subscale. An OR >1 indicates a result favoring the absence of concomitant injury. For graft choice, an OR <1 indicates a result favoring a hamstring tendon autograft and an OR >1 favors a patellar tendon autograft. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; n/a, not applicable.
PASS for KOOS ADL
No intraoperative predictor was found to be statistically significant when attempting to predict the achievement of PASS on the KOOS ADL subscale (Figure 4).

Unadjusted (black) and adjusted (gray) odds ratios (ORs), 95% CIs, and area under the receiver operating characteristic curve (AUC) for a patient-acceptable symptom state on the Knee injury and Osteoarthritis Outcome Score activities of daily living subscale. An OR >1 indicates a result favoring the absence of concomitant injury. For graft choice, an OR <1 indicates a result favoring a hamstring tendon autograft and an OR >1 favors a patellar tendon autograft. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; n/a, not applicable.
PASS for KOOS Sport and Recreation
A 1.63-fold (95% CI, 1.01-2.64; P = .045) increase was found in the odds of achieving PASS for the KOOS sport and recreation subscale in patients who did not have a concomitant cartilage injury. No effect was found for the presence of collateral ligament injury. No intraoperative predictor was found to be statistically significant when attempting to predict the achievement of PASS for KOOS sport and recreation in the adjusted analysis (Figure 5).

Unadjusted (black) and adjusted (gray) odds ratios (ORs), 95% CIs, and area under the receiver operating characteristic curve (AUC) for a patient-acceptable symptom state on the Knee injury and Osteoarthritis Outcome Score sport and recreation subscale. An OR >1 indicates a result favoring the absence of concomitant injury. For graft choice, an OR <1 indicates a result favoring a hamstring tendon autograft and an OR >1 favors a patellar tendon autograft. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; n/a, not applicable.
PASS for KOOS QoL
Higher odds of achieving PASS on the KOOS QoL subscale were found in patients receiving HT autografts compared with PT autografts in both the univariable analysis (OR = 0.43; 95% CI, 0.21-0.89; P = .023) and the adjusted analysis (OR = 0.41; 95% CI, 0.19-0.85; P = .017) (Figure 6). No effect of the presence of any concomitant injury was found for this subscale.

Unadjusted (black) and adjusted (gray) odds ratios (ORs), 95% CIs, and area under the receiver operating characteristic curve (AUC) for a patient-acceptable symptom state on the Knee injury and Osteoarthritis Outcome Score quality of life subscale. An OR >1 indicates a result favoring the absence of concomitant injury. For graft choice, an OR <1 indicates a result favoring a hamstring tendon autograft and an OR >1 favors a patellar tendon autograft. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; n/a, not applicable.
KOOS4
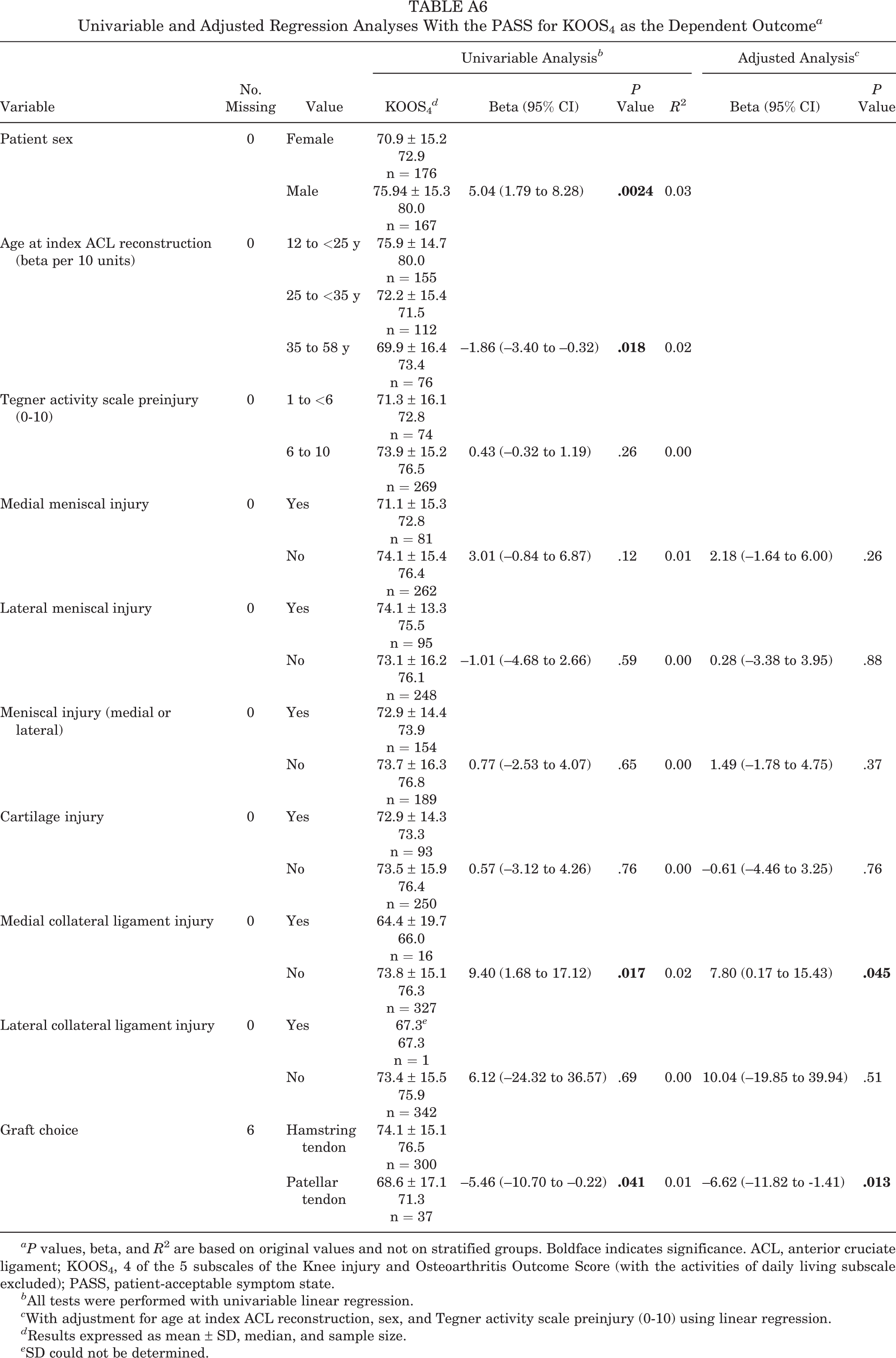
Increased odds of a higher KOOS4 were found in patients without a concomitant MCL injury (β = 9.40; 95% CI, 1.68-17.12; P = .017) and in patients undergoing primary ACL reconstruction with HT autografts (β = –5.46; 95% CI, –10.70 to –0.22; P = .041) compared with PT autografts. These results were consistent in the multivariable adjusted analyses, for patients without a concomitant MCL injury (β = 7.80; 95% CI, 0.17-15.43; P = .045) and for patients with an HT autograft (β = –6.62; 95% CI, –11.82 to –1.41; P = .013), respectively (Figure 7).

Unadjusted (black) and adjusted (gray) beta estimates (β), with percentage CIs and R 2 for a patient-acceptable symptom state on 4 of the 5 subscales of the Knee injury and Osteoarthritis Outcome Score (KOOS4) (activities of daily living subscale excluded). An OR >1 indicates a result favoring the absence of concomitant injury. For graft choice, an OR <1 indicates a result favoring a hamstring tendon autograft and an OR >1 favors a patellar tendon autograft. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament.
Multivariable Analysis (Finding the Best Predictive Model)
The stepwise multivariable analysis to predict PASS on the KOOS pain subscale showed that HT autografts were associated with achieving PASS (OR = 0.44; 95% CI, 0.22-0.91; P = .023). No other variable was entered into the model. The absence of concomitant meniscal injury (OR = 1.62; 95% CI, 1.04-2.54; P = .035) and receiving an HT autograft (OR = 0.38; 95% CI, 0.18-0.80; P = .011) were independent predictors of PASS on the KOOS QoL at 1 year after ACL reconstruction. However, this model had poor accuracy in terms of predicting PASS on the KOOS QoL (AUC = 0.62). For the KOOS4, an HT autograft remained significantly associated with improved outcome (β = –6.62; 95% CI, –1.37 to –19.08; P = .013) when age at index ACL reconstruction, patient sex, and the preinjury level of physical activity were included as covariates in the multivariable analysis. No associations were found in the multivariable analysis for the KOOS symptoms, ADL, or sport and recreation subscales.
Discussion
The main finding in this study was that approximately half of the patients reported an acceptable symptom state (ie, “feeing well”) in 4 of 5 KOOS subscales at 1 year after ACL reconstruction. Younger age and male sex were patient-related factors that increased the odds of achieving acceptable levels of knee function at 1-year follow-up. In terms of injury- and surgery-related factors, the presence of an injury to the MCL or meniscus as well as the selection of a PT autograft decreased the odds of reporting an acceptable knee function on different KOOS subscales. Overall, concomitant knee injuries appeared to have a negative influence on achieving acceptable knee function across the KOOS subscales. However, almost no consistency was found across the models regarding associations with different concomitant injuries. The lack of consistency of these findings is also highlighted by the poor capacity of any models to explain the variance in the outcome; none of the AUC results showed predictive capacity better than chance, and none of the R 2 values were above 2%. Larger studies of more homogeneous groups of patients with ACL injury, without the limitations present in the present study, may clarify the circumstances under which concomitant knee injuries play a role in predicting PROs after ACL reconstruction. In the attempt made in the present study to find the best multivariable model to predict acceptable patient-reported knee function, only the KOOS QoL subscale showed a significant association, including 2 intraoperative variables in patients 1 year after ACL reconstruction. The model showed favorable odds for HT autografts and the absence of meniscal injury, but the fit of the model was also considered to be poor.
An HT autograft was associated with increased odds of achieving PASS on the KOOS pain, the KOOS QoL, and the continuous analysis of KOOS4. The use of a PT autograft is associated with more early harvest-site morbidity than the HT autograft, 5,33 which may imply that these results disappear over time. However, the distribution of PT and HT autografts selected for primary reconstruction in this study was skewed in the cohort, which may have influenced the favorable outcome for HT grafts: 41 and 334 patients for PT and HT, respectively. The difference found in this study is an artifact likely related to the finding that more than 95% of patients in the SNKLR undergo primary ACL reconstruction with an HT autograft, thereby creating a selection bias. 13 In contrast, a Cochrane review found no difference between graft choices on knee function in a balanced cohort at short- or long-term follow-up. 19
The largest effects on predicting PASS for the different KOOS subscales were found for patient demographics favoring patients with younger age and males, which is consistent with previous literature. 1,6,8 However, the effect of preinjury level was inconsistent across the KOOS subscales. Nevertheless, several of the significant associations found in this study between concomitant injuries, intraoperative findings, and the PASS 1 year after ACL reconstruction disappeared in the adjusted analysis. This may suggest that concomitant injuries have only a minor effect on acceptable levels of symptoms in the short term. It is possible that the KOOS may be suboptimal in discriminating subjective differences in patients who have undergone ACL reconstruction with additional concomitant injuries or who have undergone different treatment regimens. The KOOS has been used frequently to evaluate patients with ACL injury, and it is the primary PRO in the Scandinavian knee ligament registers. Despite this, differences between subgroups of patients are usually below the threshold for minimal important change and sometimes even below the threshold of minimal detectable change. 14,18,27 This makes any interpretation of the KOOS difficult. In the present study, we used the PASS thresholds related to the subscales of the KOOS; these thresholds have been suggested to facilitate an understanding of PROs related to a level at which the patients “feel well.” 20 Nonetheless, the KOOS results were not bimodally distributed, which can question the relevance of the cutoff values used and the loss of power in the analysis created by the dichotomization with PASS. 22
Limitations
This study investigated the short-term influence of concomitant injuries in patients who had undergone ACL reconstruction. The univariable analyses on the presence of a concomitant injury in this study are limited by the fact that the reference group (ie, patients without the concomitant injury of interest) may include patients with other concomitant injuries, thereby reducing the effect of the model. A large number of regression models were conducted, which increases the risk of multiple significance and type 1 error. In addition, differences in treatment regimens during surgery and rehabilitation could have minimized the influence of the concomitant injuries. 34 Only a small proportion of patients had a concomitant injury to the medial (n = 18) or the lateral (n = 1) collateral ligaments, and this small number of patients may limit the ability to draw conclusions with regard to these injuries and their association with acceptable knee function. In terms of concomitant meniscal and cartilage injuries, no information relating to size, severity, or treatment was included, which may act as a limitation.
Moreover, this study may be limited by the fact that the recovery of muscle function was not controlled for in the regression analyses; that is, insufficient muscle function may be related to a nonacceptable level of symptoms in the cohort. Nevertheless, the analysis was adjusted for differences in the level of physical activity, and the average Limb Symmetry Index for the test of muscle function in the included patients can be regarded as acceptable, with mean values between 89% and 98%.
Interestingly, the majority of patients reported achieving acceptable subjective knee function, even though the cohort on average reported a decrease in their present level of physical activity compared with the preinjury level. This highlights that including a measurement of physical activity provides additional information to the KOOS when it comes to understanding knee function during sports participation. However, little is known about the association between sports participation and acceptable levels of knee function evaluated with PROs. 29 No significant differences were found related to patients lost to follow-up compared with the patients included in the study.
The strength of this study is the relatively large cohort of patients, especially in terms of studies including a clinical evaluation of rehabilitation. To our knowledge, this is the first study to use 2 patient registers comprising 2 medical professions. The SNKLR has a high level of completeness of the nationwide registrations of patients undergoing ACL reconstruction. 7 However, the rehabilitation registration is voluntary and may be subject to selection bias, where more motivated patients are potentially interested in the regular assessments.
Conclusion
More than half of the patients reported an acceptable symptom state on 4 of the 5 KOOS subscales 1 year after ACL reconstruction. Younger age and male sex increased the likelihood of achieving acceptable levels of knee function 1 year after ACL reconstruction. A lack of consistency was found related to the effect of concomitant knee injuries and graft choice on acceptable knee function.
Footnotes
Acknowledgment
The authors thank biostatisticians Bengt Bengtsson and Nils-Gunnar Pehrsson from Statistiska Konsultgruppen for help with statistical analyses and advice on interpretation of data, the Swedish National Knee Ligament Register for providing data, and Christoffer Thomeé for technical support in collecting and extracting data.
The authors declared that they have no conflicts of interest in the authorship and publication of the contribution.
Ethical approval for this study was obtained from the regional ethical review board in Gothenburg, Sweden (registration number 265-13, T023-17).
Appendix
Univariable and Adjusted Regression Analyses With the PASS for KOOS4 as the Dependent Outcome a
| Variable | No. Missing | Value | Univariable Analysis b | Adjusted Analysis c | ||||
|---|---|---|---|---|---|---|---|---|
| KOOS4 d | Beta (95% CI) | P Value | R 2 | Beta (95% CI) | P Value | |||
| Patient sex | 0 | Female | 70.9 ± 15.2 72.9 n = 176 | |||||
| Male | 75.94 ± 15.3 80.0 n = 167 | 5.04 (1.79 to 8.28) |
|
0.03 | ||||
| Age at index ACL reconstruction (beta per 10 units) | 0 | 12 to <25 y | 75.9 ± 14.7 80.0 n = 155 | |||||
| 25 to <35 y | 72.2 ± 15.4 71.5 n = 112 | |||||||
| 35 to 58 y | 69.9 ± 16.4 73.4 n = 76 | –1.86 (–3.40 to –0.32) |
|
0.02 | ||||
| Tegner activity scale preinjury (0-10) | 0 | 1 to <6 | 71.3 ± 16.1 72.8 n = 74 | |||||
| 6 to 10 | 73.9 ± 15.2 76.5 n = 269 | 0.43 (–0.32 to 1.19) | .26 | 0.00 | ||||
| Medial meniscal injury | 0 | Yes | 71.1 ± 15.3 72.8 n = 81 | |||||
| No | 74.1 ± 15.4 76.4 n = 262 | 3.01 (–0.84 to 6.87) | .12 | 0.01 | 2.18 (–1.64 to 6.00) | .26 | ||
| Lateral meniscal injury | 0 | Yes | 74.1 ± 13.3 75.5 n = 95 | |||||
| No | 73.1 ± 16.2 76.1 n = 248 | –1.01 (–4.68 to 2.66) | .59 | 0.00 | 0.28 (–3.38 to 3.95) | .88 | ||
| Meniscal injury (medial or lateral) | 0 | Yes | 72.9 ± 14.4 73.9 n = 154 | |||||
| No | 73.7 ± 16.3 76.8 n = 189 | 0.77 (–2.53 to 4.07) | .65 | 0.00 | 1.49 (–1.78 to 4.75) | .37 | ||
| Cartilage injury | 0 | Yes | 72.9 ± 14.3 73.3 n = 93 | |||||
| No | 73.5 ± 15.9 76.4 n = 250 | 0.57 (–3.12 to 4.26) | .76 | 0.00 | –0.61 (–4.46 to 3.25) | .76 | ||
| Medial collateral ligament injury | 0 | Yes | 64.4 ± 19.7 66.0 n = 16 | |||||
| No | 73.8 ± 15.1 76.3 n = 327 | 9.40 (1.68 to 17.12) |
|
0.02 | 7.80 (0.17 to 15.43) |
|
||
| Lateral collateral ligament injury | 0 | Yes | 67.3 e 67.3 n = 1 | |||||
| No | 73.4 ± 15.5 75.9 n = 342 | 6.12 (–24.32 to 36.57) | .69 | 0.00 | 10.04 (–19.85 to 39.94) | .51 | ||
| Graft choice | 6 | Hamstring tendon | 74.1 ± 15.1 76.5 n = 300 | |||||
| Patellar tendon | 68.6 ± 17.1 71.3 n = 37 | –5.46 (–10.70 to –0.22) |
|
0.01 | –6.62 (–11.82 to -1.41) |
|
||
aP values, beta, and R 2 are based on original values and not on stratified groups. Boldface indicates significance. ACL, anterior cruciate ligament; KOOS4, 4 of the 5 subscales of the Knee injury and Osteoarthritis Outcome Score (with the activities of daily living subscale excluded); PASS, patient-acceptable symptom state.
b All tests were performed with univariable linear regression.
c With adjustment for age at index ACL reconstruction, sex, and Tegner activity scale preinjury (0-10) using linear regression.
d Results expressed as mean ± SD, median, and sample size.
e SD could not be determined.