
Abstract
Background:
Gaining a better understanding of head impact exposures may lead to better comprehension of the possible effects of repeated impact exposures not associated with clinical concussion.
Purpose:
To assess the correlation between head impacts and any differences associated with cognitive testing measurements pre- and postseason.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 34 National Collegiate Athletic Association Division I men’s lacrosse players wore lacrosse helmets instrumented with an accelerometer during the 2014 competitive season and were tested pre- and postseason with the Sport Concussion Assessment Tool (SCAT 3) and Concussion Vital Signs (CVS) computer-based neurocognitive tests. The number of head impacts >20g and results from the 2 cognitive tests were analyzed for differences and correlation.
Results:
There was no significant difference between pre- and postseason SCAT 3 scores, although a significant correlation between pre- and postseason cognitive scores on the SCAT 3 and total number of impacts sustained was noted (r = –0.362, P = .035). Statistically significant improvements on half of the CVS testing components included visual reaction time (P = .037, d = 0.37), reaction time (P = .001, d = 0.65), and simple reaction time (P = .043, d = 0.37), but no correlation with head impacts was noted.
Conclusion:
This study did not find declines in SCAT 3 or CVS scores over the course of a season among athletes who sustained multiple head impacts but no clinical concussion. Thus, it could not be determined whether there was no cognitive decline among these athletes or whether there may have been subtle declines that could not be measured by the SCAT 3 or CVS.
Despite numerous cognitive concussion testing tools, as of now no single test can diagnose a concussion. 20 All concussions present and are treated differently. 4 The most commonly reported concussion symptoms are headache, dizziness, and balance disturbances. 12,20 Sensitive and objective measurements are needed 16,19 to accurately diagnose and treat for a concussion. The incorporation of multiple cognitive testing tools are critical given the varying and sometimes lack of outward display 19 or the underreporting of symptoms. 22 At times, athletes may report feeling fine, whereas cognitive testing shows neurologic deficits. 2
The National Athletic Trainers’ Association’s position statement on sport-related concussion 4 recommends baseline concussion examinations before a competitive season. At times, athletes may be symptom free, whereas cognitive testing shows neurologic deficits. 19 Baseline testing is recommended annually for adolescent athletes and for those who have recently sustained a concussion. 4 These baseline tests should include a clinical history, physical and neurologic evaluation, and measures of motor control and neurocognitive function. The incorporation of a multifaceted approach, including the use of a graded symptom checklist, Standardized Assessment of Concussion, neuropsychological assessment, and balance assessment, is considered one of the best ways to manage a concussion. 10 To capture these different components, commonly used tools include the Sport Concussion Assessment Tool (SCAT 3), a computerized cognitive evaluation tool, and the Balance Error Scoring System test.
Concussion management has been studied significantly, and it is well known that early intervention leads to a favorable prognosis. 10 While early intervention is crucial, little research is available regarding subconcussive blows and the use of cognitive testing in assisting with subconcussive reporting. A proposed definition of subconcussive impact is a “cranial impact that does not result in known or diagnosed concussion on clinical grounds.” 1 Research has shown that subconcussive impacts may result in cumulative neurologic deficits. 1 Repeated mild head trauma can lead to neuropsychological deficits and changes in cognition, mood, and behavior. 24
However, Miller et al 21 found no meaningful changes from pre-, mid-, and postseason reports regarding cognitive testing, indicating that cognitive testing may not be sensitive enough to detect the effect of subconcussive impacts throughout a season. Interestingly, others 14,18 found poorer scores on postseason cognitive testing among those with no documented concussion.
With the increase in concussion rates in recent years, 15 all those involved in sport need to be aware of the best practices to manage a concussion and which tests are the most sensitive. Equipment-intensive sports have a high incidence of concussion, 17 and health care professionals need to be aware of the high incidence in underreporting of symptoms, 22 which may put athletes at risk. The aim of our study was to analyze the head impact exposures (possible subconcussive blows) and the correlation between these exposures and any changes on 2 cognitive tests: the SCAT 3 and the Concussion Vital Signs (CVS) computer-based neurocognitive test. Our hypothesis was that the more frequent the head impacts, the lower the cognitive test scores would be after postseason play.
Methods
Participants
Thirty-six National Collegiate Athletic Association (NCAA) Division I men’s lacrosse players from a single university participated in this study. All athletes were fully cleared for participation, with no reported concussion within the previous 6 months. Two athletes were removed: 1 because of a concussion during the season and 1 for an ongoing lower extremity injury. A total of 34 players over the course of a single competitive season were included in the analysis (mean ± SD: height, 71.65 ± 2.5 in; weight, 178.03 ± 21.44 lb; age, 19.56 ± 1.44 years). The study was approved by the university’s internal review board, and all participants signed an informed consent.
Instrumentation
All players wore Warrior Sports Regulator II helmets instrumented with a GForceTracker (GFT) sensor. The GFT was affixed internally to the crown of the helmet and calibrated prior to use per the manufacturer’s guidelines. The GFT contains a triaxial accelerometer and triaxial gyroscope to measure linear acceleration and rotational velocity, and it has been shown to be a valid and reliable instrument to measure these data. 5 This sensor has a sampling frequency of 3 kHz 5 and recorded data when an impact exceeded the study’s preset threshold of 20g; in sum, 40 milliseconds of data per impact were recorded (8-millisecond pretrigger and 32-millisecond posttrigger).
The SCAT 3 was used per recommendations from the Fourth International Conference on Concussion. 20 The SCAT 3 includes short neuropsychological tests to assess memory and function as well as the Maddocks questions and Standardized Assessment of Concussion questions for the assessment of symptoms. 20
The CVS is a free computerized neurocognitive tool 11 used by the hosting institution. It includes 7 tests: verbal and visual memory, psychomotor speed (combined score of finger tapping and symbol digit coding), executive function (performance on shifting attention test), cognitive flexibility (shifiting attention and the Stroop test), and the CPT correct responses (the number of correct responses on the continuous performance test). 11
Procedures and Data Collection
The GFT was internally affixed to each player’s helmet via 3-mm double-sided adhesive at the crown of the helmet and was calibrated per the manufacturer’s guidelines. GFTs were automatically turned on and off before and after each practice and game via a hub connected to the laptop containing the GFT software. GFTs were charged every other day while remaining attached to the helmet. After the sensor was fully charged, the data were downloaded via USB connection and exported to a secure central server. All sensors were charged after each game to ensure proper battery life for the following practice. A total of 9702 impacts were documented amid a total of 15 games (3241 impacts recorded) and 45 practices (6361 impacts recorded) during the lacrosse season.
Cognitive testing data were collected via the SCAT 3 and CVS tests. One of the researchers (T.L.M.) and the team’s head athletic trainer conducted pre- and postseason SCAT 3 data collections and supervised CVS testing while the athletes completed it on the computer.
Statistical Analysis
A paired-sample t test was conducted to compare pre- and postseason scores on the SCAT 3 and CVS neurocognitive testing tools for each variable (Table 1). To determine if there was a relationship between head impact exposures and cognitive testing, a Pearson correlation was used. Score differentials were computed from pre- to postseason and used to calculate correlations with head impact exposure data, which included mean linear acceleration per impact, mean Head Injury Criterion per impact, average Gadd Severity Index per impact, and total hits. All data were analyzed with SPSS (v 23; IBM Corp). Statistical significance was established a priori as α ≤ .05.
Mean Differences in Pre- and Postseason Scores on the SCAT 3 and CVS a

a CPT, Continuous Performance Test; CVS, Concussion Vital Signs; SCAT 3, Sport Concussion Assessment Tool.
b Statistically significant difference between pre- and postseason scores (P < .05; paired-sample t test).
Results
Table 1 shows the mean differences for the SCAT 3 and CVS test and the improvements or deficits between pre- and postseason testing. Paired-sample t tests determined no statistical significance in SCAT 3 measurements from pre- to postseason. Statistically significant differences were found in half of the CVS testing components. Decreases in scores from pre- to postseason were noted in visual reaction time (P = .037, d = 0.37), reaction time (P = .001, d = 0.65), and simple reaction time (P = .043, d = 0.37). Increases in scores would have indicated decreased performance from pre- to postseason.
Interestingly, statistically significant improvements were also found in the following tests from pre- to postseason: executive function (P = .007, d = 0.50), with a 3.79-point improvement in mean score from pre- to postseason, and cognitive flexibility (P = .006, d = 0.51), with a mean improvement in score of 3.78 points.
To investigate if there was a statistically significant association between head impact exposure data and cognitive testing, a Pearson correlation was computed according to pre- to postseason score differentials with head impact exposure data. The only significant correlation found was between SCAT 3 cognitive scores from pre- to postseason and total number of head impacts sustained (r = –0.362, P = .035). Correlations are detailed in Tables 2 and 3.
Pearson Correlations Between SCAT 3 Differential Scores and Head Impact Exposure Data a
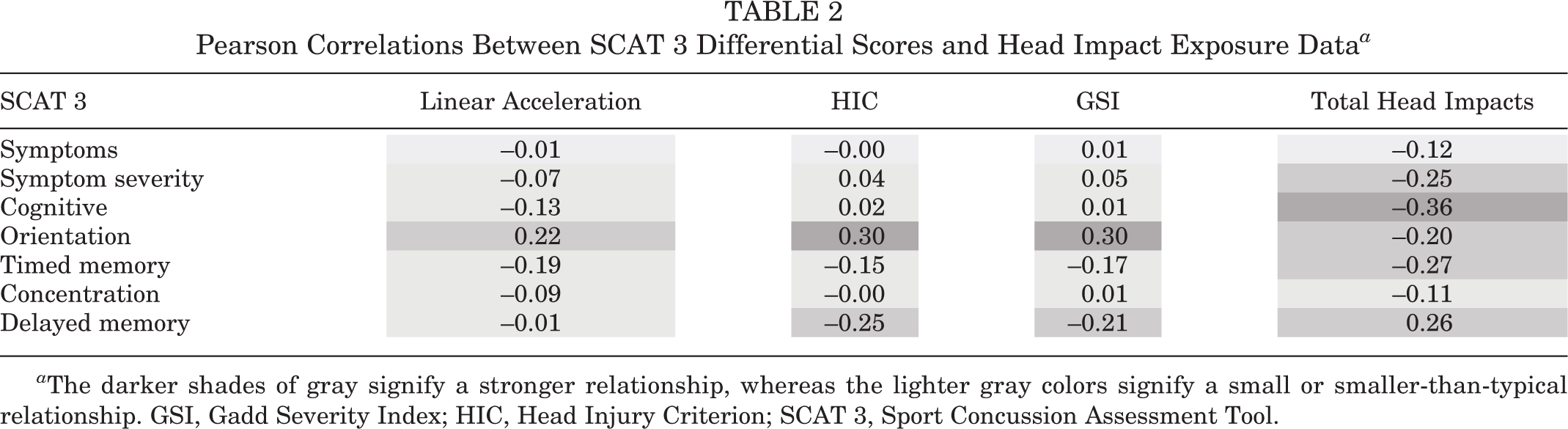
a The darker shades of gray signify a stronger relationship, whereas the lighter gray colors signify a small or smaller-than-typical relationship. GSI, Gadd Severity Index; HIC, Head Injury Criterion; SCAT 3, Sport Concussion Assessment Tool.
Pearson Correlations Between CVS Differential Scores and Head Impact Exposure Data a

a The darker shades of gray signify a stronger relationship, whereas the lighter gray colors signify a small or smaller-than-typical relationship. CPT, Continuous Performance Test; CVS, Concussion Vital Signs; GSI, Gadd Severity Index; HIC, Head Injury Criterion.
Discussion
Based on the study sample of 34 NCAA Division I men's lacrosse players, statistically significant improvements in cognitive testing scores were found in CVS cognitive testing from pre- to postseason in the domains of visual reaction time, reaction time, and simple reaction time. Significant improvements in test scores were also seen from pre- to postseason in 2 areas of the CVS test: executive function and cognitive flexibility. No statistical significance was found in SCAT 3 scores, including symptoms scores. McAllister et al 18 reported poorer scores on some postseason cognitive testing and found a correlation with greater head impact exposures on those athletes with no documented concussions.
Our findings show no statistically significant declines in measurements in either the SCAT 3 or CVS tests. Similar to our results, those of Gysland et al 13 revealed no meaningful changes from pre- to mid- to postseason on neurologic function. Conversely, others 8,14 found lower cognitive scores for those with no reported concussion and greater head impact exposures. Further, our findings associated with repeat injury showed impairments in complex spatial learning and other cognitive impairments. Interestingly, we found significant improvement in performance with some CVS testing variables. Given the variables in which we saw improvement (Table 1), we hypothesize that these improvements may be due to the nature of the sport of lacrosse and the overall improvement in reaction time seen with practice.
No association could be drawn from acceleration forces and total hits regarding any changes in cognitive testing for any variable in the SCAT 3 and CVS tests. A Pearson correlation based on pre- to postseason score differentials showed that the relationship was linear with regard to pre- and postmeasurements of each test when compared with Head Injury Criterion mean, Gadd Severity Index mean, and total hits (Tables 2 and 3). Only cognitive score changes on the SCAT 3 showed a significant correlation with total number of impacts (P = .035). Breedlove et al 3 found progressive neurophysiologic changes with accumulated impacts to the head of high school football players; however, the distribution of head impacts was not significantly different, and the magnitude of the impacts did not correlate to a concussion injury. Findings in our study may differ from these findings owing to the age of the participants, the type of sport, and the study design.
Although this study does not show significant change in all areas pre- to postseason with the SCAT 3 and CVS testing, it does show some areas of significance, as discussed. Eckner et al 9 found that impacts to players who sustain a concussion are not often different from those to asymptomatic players. We need to be aware that athletes may not report symptoms 22 and that athletes with observable symptoms have neurophysiologic changes. 25
As more individuals participate in sport and the intensity of sports increases, the velocity of impacts increase and may contribute to the higher incidence rates of concussion. 7 Repeat mild head trauma may lead to complex neuropsychological sequelae involving changes in cognition, mood, and behavior. 24 The number of concussions continues to increase in football, men’s lacrosse, and women’s soccer, 15 and concussion is the most common form of traumatic brain injury worldwide. 23 Limitations of our study include assessing data over 1 season versus a 4-year span and not incorporating physical signs and symptoms in the analysis.
Based on our findings, further research is needed on neurocognitive tools and assessment of cognitive function for those without reported concussion. Our study failed to find any decline in SCAT 3 or CVS scores over the course of a season among athletes who sustained multiple head impacts but no clinical concussion. Thus, we cannot determine whether there was no cognitive decline for these athletes or whether there may have been subtle declines that could not be measured by the SCAT 3 or CVS. Although the SCAT 3 in this study showed no significant change between pre- and postseason play, it is possible that there are cognitive changes that the SCAT 3 cannot detect. 6 Furthermore, the CVS may not be sensitive enough for changes attributed to subconcussive impacts over a single season. Further assessment of these data is needed over a 4-year college career.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Sacred Heart University, Fairfield, Connecticut, USA.