
Abstract
Background:
Several radiographic parameters have been associated with a discoid lateral meniscus. However, limited information is available regarding the radiographic findings of a discoid meniscus in the pediatric population.
Purpose:
To determine the effect of age and weightbearing (WB) on radiographic parameters associated with discoid lateral menisci in pediatric patients.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Radiographs of pediatric patients with arthroscopically confirmed lateral discoid menisci were compared with age-, side-, and sex-matched individuals with confirmed normal menisci. Radiographic parameters of lateral joint space width (LJSW) and fibular head height (FHH) were measured by 3 physicians.
Results:
Significant differences were found between the discoid and control groups when LJSW (P = .002) and FHH (P < .001) were compared. Interrater reliability was good for LJSW (intraclass correlation coefficient [ICC], 0.635) and excellent for FHH (ICC, 0.759). WB radiographs were noted to have better interrater reliability compared with non-WB radiographs for LJSW (ICC, 0.729 vs 0.514, respectively) but had reduced interrater reliability for FHH (ICC, 0.625 vs 0.868, respectively). Subgroup analysis with age stratification indicated that FHH was significantly decreased (indicative of a high fibular head) in the discoid group for all age groups (P < .001 for <10 years and 10-14 years; P = .030 for >14 years); however, LJSW was significantly different only in patients older than 14 years.
Conclusion:
Increased LJSW and FHH were associated with discoid lateral menisci and showed satisfactory interrater reliability. Radiographic evaluation for potential discoid meniscus in pediatric and adolescent patients may be improved by use of fibular height to indicate the presence of a discoid lateral meniscus across age groups, while lateral joint space may be more reliable for older patients.
A symptomatic or torn discoid lateral meniscus is a knee injury that can present at any age but often presents in pediatric or adolescent patients. A discoid meniscus is an abnormally shaped meniscus in the knee that places the patient at a greater risk of meniscal damage or knee injury. 6,15,22 Although some individuals with a discoid meniscus can go through their entire life without experiencing any problems, others will experience knee pain and/or mechanical symptoms, often beginning in childhood. 16 Discoid menisci are confirmed through magnetic resonance imaging (MRI) or direct visualization during arthroscopy; however, these methods are costly, and arthroscopy carries the inherent risks of a surgical procedure. 2,23
Several studies have been published describing the radiographic changes associated with a discoid lateral meniscus. 8,9,13,19,21 These findings include widened femorotibial joint space, a squared-off appearance of the lateral femoral condyle, cupping of the lateral tibial plateau, obliquity of the lateral articular surface, increased fibular head height (FHH), and hypoplasia of the lateral intercondylar spine. However, almost all of these studies have been performed on adults, and limited information is available regarding the radiographic findings of a discoid meniscus in the pediatric population. 4,16,20 To our knowledge, the literature provides no reports that objectively correlate radiographic changes with age or weightbearing (WB) status.
Therefore, the purpose of this study was to determine the effect of age and WB on radiographic parameters associated with discoid lateral menisci in pediatric patients. We hypothesized that an older adolescent population would show more significant radiographic findings of discoid lateral menisci compared with a younger population. We also hypothesized that WB radiographs would improve the diagnostic reliability of established radiographic parameters for discoid lateral menisci.
Methods
Institutional review board approval was obtained for this retrospective review. Patients younger than 18 years with arthroscopically proven discoid lateral meniscus, who were treated between 2006 and 2014 at 2 major pediatric medical centers, were identified. Patients were excluded if they had knee injury or deformity other than a discoid meniscus. In addition to the study group, control patients with radiographs for patellofemoral pain or other generalized knee pain and normal menisci as determined by MRI were chosen during the same open period. The control group was matched by age and sex to the study group.
All patients in this study had a true anteroposterior radiograph of the knee, completed in either a WB or a non-WB position as determined by physician preference, clinical care, or clinical protocol for each site. Radiographs were evaluated by 3 investigators (a board-certified pediatric orthopaedic sports medicine physician [M.D.M.] and 2 orthopaedic surgery residents [R.K. and J.M.]). Measurements were made through use of the digital measurement tools available on the Picture Achieving and Communication System (iSite; Philips). Each image was read twice in random order, at least 3 weeks apart, and the readers were blinded to the patients’ group assignment.
Six knee parameters were measured as described by Kim et al 13 : FHH, lateral joint space width (LJSW), tibial spine height (TSH), obliquity of the lateral tibial plateau (OLTP), cupping of the lateral tibial plateau (CLTP), and width of distal femur (WDF) (Figure 1). FHH was defined as the distance from the lateral tibial plateau to the apex of the fibular head, LJSW as the width between the lateral femoral condyle and the lateral tibial plateau, TSH as the height of the lateral tibial spine from the tibial plateau, OLTP as the angle between the lateral tibial plateau and the tibial spine, CLTP as the height from the imaginary tibial joint line to the proximal limit of the lateral tibial plateau, and WDF as the distance between the most prominent edge of the medial femoral condyle to the most prominent edge of the lateral femoral condyle. All parameters were measured as continuous variables in millimeters, except for OLTP, which was measured in degrees.
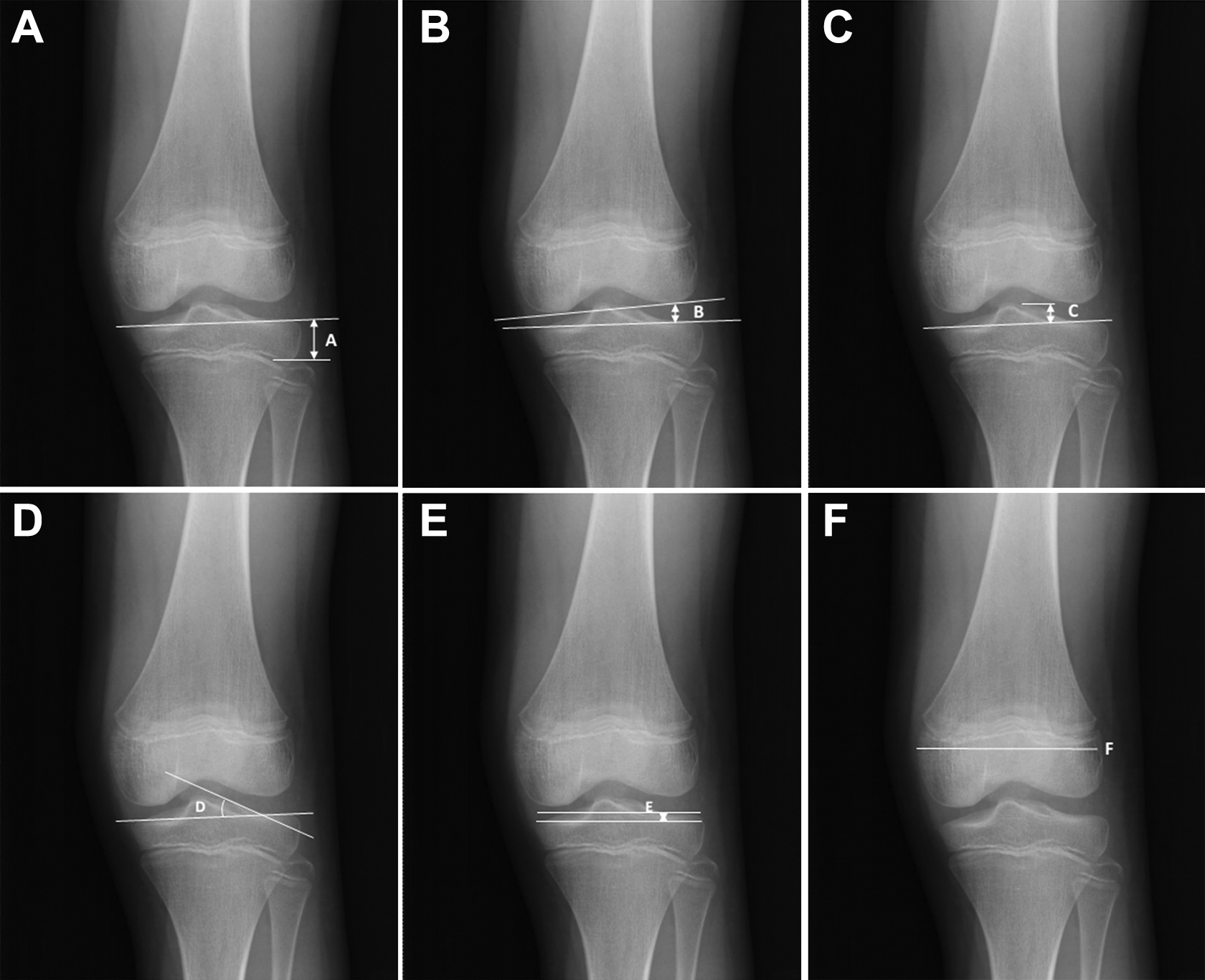
(A) Fibular head height. (B) Lateral joint space width. (C) Tibial spine height. (D) Obliquity of the lateral tibial plateau. (E) Cupping of the lateral tibial plateau. (F) Width of distal femur.
Descriptive statistics were computed for all variables of interest, and the means and standard deviations are presented for ease of understanding. Inter- and intrarater reliabilities were assessed through use of intraclass correlation coefficients (ICCs) to determine the agreement of the measurements between reviewers and within reviewers. The intraclass correlation was also extended to look at the ICC for WB and non-WB radiographs. For the purposes of this study, ICC values less than 0.5 were considered poor agreement, values between 0.5 and 0.7 were considered good agreement, values between 0.7 and 0.9 were considered excellent agreement, and values greater than 0.9 were considered near-perfect agreement. To assess differences between the 2 study groups (ie, discoid and control), a single-factor analysis of variance (ANOVA) was used. A P value of less than .05 was considered a statistically significant difference. All statistical testing was performed by use of SAS software version 9.3 (SAS Institute Inc).
Given that the test for this study was a Student t test, the following method was used to calculate sample size. These calculations are based on the data presented by Kim et al, 13 in which the lateral joint space for the control group was 4.2 ± 1.2 mm and the lateral joint line space for the discoid group was 5.7° ± 1.7°. The study design allows for a 1-sided test (H0 μ1 = μ2, H1 μ1 < μ2, where μ2 is the discoid group). We propose a 1-sided t test because the most commonly stated finding is that patients with discoid menisci will have a greater lateral joint space than patients with typical menisci, and therefore we were not concerned with the lateral joint space being smaller in the discoid group compared with the control group. Furthermore, a 1-sided t test allows for a smaller sample size, which is clinically pertinent given the relatively small number of patients diagnosed with discoid meniscus. Therefore, by use of the methods published by Whitley and Ball, 28 it is possible to calculate the target difference based on the Kim et al 13 data, where the difference in means was 1.5 and the average SD was 1.5 between groups. The standard difference is calculated to be 1.0 (target difference/SD). Then, through use of the nomogram provided by Altman 1 and assuming an alpha of .05 and a power of 0.80, a total of 36 patients is required for each study group.
Results
A total of 135 patients were included in this study: 67 in the discoid group and 68 controls; patient demographics are shown in Table 1.
Patient Demographics

The discoid group consisted of 32 boys and 35 girls with a mean age of 11.66 years (range, 5-17 years). The control group consisted of 35 boys and 33 girls with a mean age of 11.90 years (range, 5-17 years). Both the discoid group and the control group had 15 WB radiographs each. No significant difference was noted between the discoid group and control group with regard to age (P = .999), sex (P = .842), and knee side examined (P = .989). Table 2 lists the mean and SD of each radiographic parameter measured for the discoid and control groups.
Radiographic Measures of the Study Groups

a Values expressed as mean ± SD, in millimeters or degrees as noted.
Significant differences were noted between the discoid and control groups in comparisons of LJSW, FHH, WDF, and CLTP. As seen in Table 3, interrater reliability was excellent for both WDF and FHH and good for LJSW, OLTP, and TSH; however, interrater reliability was poor for CLTP. No statistically significant difference was seen in radiographic measures between the discoid and control groups for TSH (P = .507) or OLTP (P = .113). All investigators completed a second radiographic evaluation to determine intrarater reliability. Intrarater reliability was excellent to near perfect for WDF and excellent for 2 of the 3 investigators with LJSW, FHH, and TSH (Table 4). Intrarater reliability was poor for 2 of the 3 investigators with CLTP and OLTP.
Interrater Reliability a

a ICC, intraclass correlation coefficient.
b Values expressed as mean ± SD, in millimeters or degrees as noted.
Intrarater Reliability

Table 5 shows the effect of WB on the radiographic parameters measured. WB radiographs had better interrater reliability compared with non-WB radiographs for LJSW, WDF, TSH, and OLTP but reduced interrater reliability for FHH.
Reader Reliability Based on Weightbearing Status a
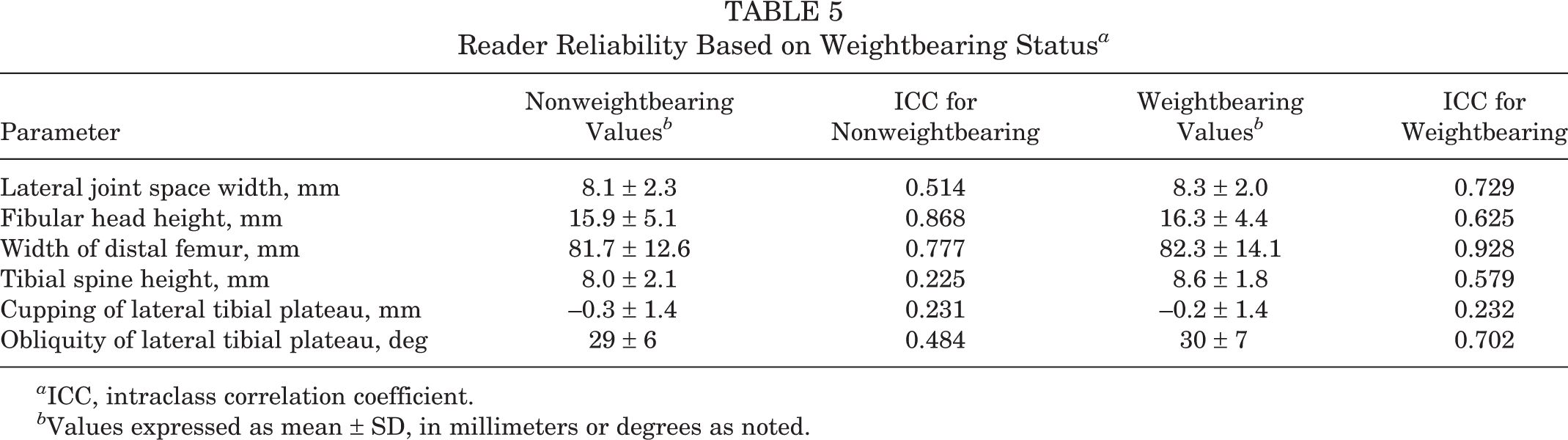
a ICC, intraclass correlation coefficient.
b Values expressed as mean ± SD, in millimeters or degrees as noted.
Subgroup analysis based on age was also completed, comparing patients under 10 years old (n = 50), patients between 10 and 14 years old (n = 44), and patients over 14 years old (n = 41). The FHH measurement was significantly decreased (indicative of a high fibular head) in the discoid group in all age groups (P < .001 for <10 years and 10-14 years; P = .030 for >14 years) (Table 6). However, even though LJSW was greater in the discoid group at all ages, it was significantly different only in patients older than 14 years (P = .016) (Table 7).
Fibular Head Height Measurements by Age

a Values expressed in millimeters as mean ± SD.
Lateral Joint Space Width Measurements by Age

a Values expressed in millimeters as mean ± SD.
Discussion
Discoid meniscus is a well-described abnormal, congenital anatomic variant of the meniscus, first described by Young et al 29 in 1887. Since then, numerous studies have been published on discoid meniscus, describing its histologic features, anatomic classifications, and various treatment options. 5,14,17,24,27 Historically, the diagnosis of discoid meniscus was based on physical examination and patient history, although the clinical presentation can be highly variable. 14,15 Today, MRI and arthroscopy are used to more definitively diagnose discoid menisci, but MRI can be costly and arthroscopy is invasive and not without risk. 23
Plain radiography has been considered an ancillary tool for the diagnosis of discoid meniscus, as many past studies have reported normal radiographic findings in patients with a discoid meniscus. 10,18,20 Nathan and Cole 18 reported finding only early arthritis in adults and concluded that plain radiographs had little value in the detection of discoid lateral meniscus. Ogut et al 20 studied 11 cases of discoid meniscus in children and reported that radiography was not helpful, as none of their radiographs showed widening of the lateral joint space.
In contrast, many studies have been published describing characteristic radiographic findings associated with a discoid lateral meniscus. 8,13,19,21 In 1950, Jeannopoulos 10 reported 21 cases of discoid lateral meniscus. Of these 21 cases, 4 exhibited a widened lateral joint space and 2 demonstrated lateral femoral condyle hypoplasia on radiographs. In 1981, Engber and Mickelson 8 reported on a 22-year-old patient with a discoid lateral meniscus in whom cupping of the lateral tibial plateau was found on radiograph. The following year, Dickhaut and DeLee 7 described the “discoid lateral-meniscus syndrome” and reported a widened lateral joint space and cupping of the lateral tibial plateau.
More recently, Nawata et al 19 assessed radiographic characteristics of discoid lateral meniscus in adults and observed cupping of the lateral tibial plateau, while Bellier et al 3 reported that children with discoid lateral menisci showed widened lateral joint space, blunted lateral tibial eminence, and obliquity of the lateral tibial plateau on radiographs. In 2001, Rao et al 21 published a retrospective study of 87 patients to establish common clinical and radiologic features associated with a discoid lateral meniscus. The investigators concluded that of the 63 patients who had radiographs available for review, 53.9% showed bony changes known to be associated with a discoid meniscus. The most common finding was widening of the lateral joint space. Studying a group of 130 adults, Song et al 25 reported that a high fibular head and a widened lateral joint space were reliable screening parameters for complete but not for incomplete discoid meniscus. Jiang et al 11 also described the clinical utility of radiographs as a screening tool for lateral discoid meniscus in an adult population.
Our present study objectively confirms the finding of increased lateral joint space and shows that a high fibular head is associated with a discoid lateral meniscus. A high fibular head might be a more useful clinical screening tool, as the standard deviations for our LJSW were greater than the differences in the mean values between these groups. Given the shape of the discoid meniscus, it makes sense that the LJSW would be increased because the meniscus completely, or nearly completely, covers the lateral tibial plateau and thus widens the lateral joint space. With regard to the smaller measurements for FHH observed in our discoid cohort, this finding may have several causes. Perhaps the lateral tibial plateau is depressed from the discoid, which would lead to apparent joint space widening and a relatively higher fibular head. However, the difference between the measurement of the LJSW and FHH does not compute to the total distance between the proximal aspect of the fibular head and distal femur. Therefore, the LJSW and FHH measurements are independent of each other, suggestive of other reasons responsible for the height difference. Further studies are needed to correlate the relationship between lateral joint space widening and a relatively high-appearing fibula.
Our findings of increased LJSW and a high fibular head associated with discoid lateral menisci confirm the results of Kim et al. 13 They performed one of the few studies in the literature that used objective knee dimensions rather than subjective findings to compare a normal control group and a discoid meniscus group. Among the dimensions that Kim et al 3 measured, only widening of the lateral femorotibial joint space and height of the fibular head were statistically significant between groups. However, one of the limitations to their study was the exclusion of pediatric patients.
Limited information is available in the literature regarding the radiographic findings of a discoid meniscus in the pediatric population. 4,16,20,26 Our study looked exclusively at pediatric patients with discoid menisci and objectively compared them with normal age- and sex-matched control patients. To our knowledge, only 1 other study, that by Choi et al, 4 has objectively compared the radiographic features of discoid meniscus and normal controls in children. Although our study as well as that by Choi et al 4 showed a significant difference in LJSW and FHH between the discoid and control groups, unlike Choi et al, we did not find a significant difference with regard to tibial spine height and obliquity of the lateral tibial plateau. Additionally, Choi et al 4 analyzed only non-WB radiographs and did not qualify their results based on patient age. To our knowledge, our study is the first in the literature to objectively correlate discoid meniscus radiographic changes with age or WB status.
Since most of the literature describing radiographic changes associated with discoid menisci has been in adults, it is not known whether these radiographic changes are present in youth or develop over time. In a study of 23 adult patients with discoid menisci, Nawata et al 19 hypothesized that characteristic radiographic changes may be induced by the abnormal morphologic features of the lateral discoid meniscus causing a mechanical imbalance between the medial and lateral compartments of the knee with aging. While our overall results showed that both LJSW and FHH were significantly different between pediatric discoid and control patients, our subgroup analysis based on age showed that FHH was significantly decreased (indicative of a high fibular head) in the discoid group across all ages, while increased LJSW was significantly different only in patients older than 14 years. This may be because as the knee approaches skeletal maturity, increased ossification near the joint space likely makes LJSW a more reliable measure in this age group.
In addition to analysis by age, the use of WB radiographs and the associated effect on radiographic measurements in pediatric patients with discoid menisci have not been previously reported. Our results demonstrated that WB radiographs provide increased reliability among readers for most measured parameters, including LJSW. WB allows a more realistic view of the joint space; however, WB radiographs are more common in adult orthopaedic knee evaluation because of the prevalence of degenerative osteoarthritis and associated joint space narrowing seen in this older patient population. FHH was the only measure that had reduced reliability with WB, although its interrater reliability was still good. A possible explanation for this improved reliability may be the fact that WB radiographs could be more regimented, and thus the amount of knee flexion or lower limb rotation may vary among non-WB radiographs whereas WB radiographs may be able to control these positions. It is unclear why reliability would be reduced for FHH given that it is a more standardized examination. However, an explanation could be that a small amount of knee flexion makes the fibular head easier to see and measure. Further research is certainly needed to assess these explanations and improve reliability.
The strengths of this study include the relatively large number of patients with a discoid lateral meniscus confirmed by arthroscopy. 12 Another strength is that our study was blinded in order to prevent bias and included radiographs from our control group of age-, side-, and sex-matched individuals with confirmed normal menisci on MRI. Additionally, this is the first study to include a subgroup analysis by age and the first study to look at WB radiographs for this condition.
Nonetheless, our study has limitations. Our relatively small number of WB radiographs likely represents current pediatric practice patterns that de-emphasize WB radiography in the child with a painful knee who is unlikely to have degenerative arthritic changes. Further analysis with a larger group of WB radiographs would provide additional support to our findings. Radiographic techniques and quality varied, and this could have affected the reliability of the results. Another potential limitation was having 2 residents as reviewers. However, their results were similar to those of a double fellowship–trained orthopaedic attending surgeon (M.D.M.), which points to these measurements’ being reproducible at various levels of experience. In addition, we did not distinguish between complete and incomplete-type discoid meniscus or calculate normalized knee dimensions (absolute values of each knee dimension divided by each knee’s interepicondylar distance). We used age- and sex-matched groups, which should minimize any differences in relative size of the patients’ knees. Another limitation of this study is the lack of height and weight measurements for both control and discoid patients. How these variables influence radiographic measurements warrants further investigation.
Conclusion
Increased lateral joint space and a high fibular head are radiographic findings associated with a discoid lateral meniscus and have good interrater reliability. WB radiographs improve interrater reliability for LJSW but slightly decrease reliability for FHH. Higher fibular height was consistently seen across age groups, but increased LJSW was significantly different only in the group older than 14 years. Fibular height might be a better radiographic screening parameter for discoid lateral meniscus evaluation across age groups, while lateral joint space may be better in older adolescent patients.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.D.M. is a committee chair of the Pediatric Research in Sports Medicine (PRISM) group, is a board member of the Research in Osteochondritis Dissecans of the Knee (ROCK) group, has received publishing support from Elsevier, and receives research support from Allosource Vericel. J.L.P. is a paid consultant for Arthrex, Ceterix, Grand Rounds, and Smith & Nephew.
Ethical approval for this study was obtained from Connecticut Children’s Medical Center (CCMC IRB No. 14-028).