
Abstract
Background:
Ultimate Frisbee (ultimate) is a fast-growing, popular sport played nationally by over 4 million athletes. While several studies have examined injury rates in ultimate, no work has investigated the prevalence of concussions specifically or players’ knowledge and management of those injuries.
Purpose:
To estimate the lifetime prevalence of concussions in ultimate and to assess players’ knowledge of concussions as well as their concussion management behaviors.
Study Design:
Descriptive epidemiology study.
Methods:
From June to November 2015, we collected ultimate-related concussion data via an anonymous web-based survey, the Concussion in Ultimate Frisbee Survey, from a convenience sample of 787 male and female ultimate players across the United States.
Results:
There were 553 male and 234 female respondents included in the analysis; 26.58% of men and 24.79% of women reported that they had sustained at least 1 concussion while playing ultimate, with 45.58% and 43.10% of those men and women, respectively, reporting multiple concussions. A total of 67.81% of men and 78.21% of women stated that they would remove themselves from play after sustaining a given concussion, although 45.99% of men and 37.62% of women indicated that they had returned to play in the same game or practice.
Conclusion:
Our preliminary data suggest that concussions do commonly occur in competitive ultimate and that better education and management of concussions in ultimate athletes are needed. This study is an important first step in deepening our understanding of these issues.
Given the vast number of adolescents and young adults who participate in sports associated with a head injury risk, and with an estimated 1.3 to 3.8 million sports-related concussions occurring per year, 4,5 concussions are a major public health concern. Furthermore, these figures are likely conservative estimates because of difficulties with the collection of such data and the underreporting of symptoms. 8
Published incidence rates of concussions in various sports 6,18 tend to focus on those with the greatest perceived head injury risk, such as football and ice hockey. Even though competitive sports played predominantly at the club or nonelite level, such as rugby, have received some attention in this area, 3,14 athletes in these sports are often overlooked in return-to-play guidelines designed to enhance player safety. 13 Ultimate (commonly known as ultimate Frisbee) is a sport that has been overlooked and likely needs better regulation.
Ultimate is a team sport of two 7-player squads using a high-tech plastic disc, with matches held on 120- by 40-yd fields of play similar to a football field. The goal of the game is to complete a pass to a receiver over the line of the opponent’s end zone. Players are not permitted to run while they have the disc, but they may pivot and then pass to their teammates within 10 seconds of holding the disc.
Ultimate is a fast-growing sport, with over 4 million participants in the United States. 15 Over the past 2 decades, it has experienced increased levels of athleticism, competition, and professionalization. The national governing body, USA Ultimate, has over 50,000 active members, including a collegiate division (a university club sport) of nearly 18,000 athletes across 566 men’s teams and 341 women’s teams. USA Ultimate experienced growth of 94.8% in active membership between 2007 and 2015. 15 The sport is played competitively at the high school, college, club, and masters (≥33 years old for men, ≥30 years old for women) levels, across 3 sex-based divisions: men’s, women’s, and coed. Additionally, across the United States, there are many large tournaments not affiliated with USA Ultimate as well as local leagues with thousands of active members. 1,11 There are 2 professional leagues composed of 34 teams. None of these leagues, tournaments, divisions, or organizations is part of the National Collegiate Athletic Association (NCAA).
A unique feature of ultimate is the “Spirit of the Game.” In amateur levels, ultimate is player officiated, with referees utilized only in championship tournaments. In general, the infrastructure is less developed than sports that have received the most attention related to concussions. For these reasons, concussions in ultimate should be studied to help determine whether they pose a health risk to the over 4 million athletes who play competitive ultimate.
The literature on concussions in ultimate is lacking. Studies examining injuries in the sport have typically focused on only one or a very small number of tournaments and have not attempted to characterize any concussions sustained. 7,17 Furthermore, these studies did not address players’ knowledge and understanding of concussions, which is of particular importance because these athletes are often self-coached and self-refereed and do not receive university athletic training services.
We aimed to better understand the lifetime prevalence and mechanism of injury of concussions in competitive ultimate players and to assess their knowledge, attitudes, and behaviors around concussion-related management.
Methods
Data Collection
We created an anonymous web-based survey, the Concussion in Ultimate Frisbee Survey, to collect demographic information and information regarding the nature of ultimate players’ athletic competition, concussion history, and knowledge. For face validity, we beta-tested the survey on a sample of 27 current competitive ultimate players and modified accordingly. The survey was dynamic, and certain questions were displayed only when participants had responded affirmatively to a prior question. (A static version of the survey can be found in the Appendix.)
Because there is currently no publicly available national registry of competitive ultimate players from which to draw a large random sample, we attempted to collect data by contacting professional teams, administrators of select recreational leagues, captains of college teams, and coaches of teams ranked by USA Ultimate. Contact information for these teams and individual persons was either publicly available via team and league websites or known personally to us. We asked these contacts to distribute our survey to current and former members of their leagues or teams, and to other regional teams, in a snowball sampling method via an email link. Through personal contacts of the first author (D.J.L.), over 50 such teams, leagues, and individual persons agreed to participate in the study by distributing the survey to their athletes; the individual contacts subsequently reported to us the number of individual persons to whom they distributed the survey. Distribution lists ranged from teams consisting of 14 players to leagues with over 500 active members. Based on the reported size of these distribution lists, and their potential overlap, we estimate that approximately 3500 players received the electronic invitation to complete our survey.
The survey was hosted by Qualtrics from June to November 2015. No personally identifiable information was collected. This study was approved by the governing institutional review board, and all participants provided consent to be included. Inclusion criteria were all ultimate players at least 18 years of age who had spent time playing organized ultimate in a professional, club, college, high school, or recreational league.
Definition of Injury and Exposure
Respondents were asked to self-report if they had ever received a concussion playing ultimate, with the following definition: “Concussion is a disruption in brain functioning, which is caused by a bump or blow to the head or body. It may or may not be accompanied by a temporary loss of consciousness, and symptom presentation may include changes in the realms of physiology, cognition, emotion, and/or sleep.” Additionally, we provided a list of typical concussive signs and symptoms (Table 1).
List of Concussive Signs and Symptoms Provided to Survey Respondents

Statistical Analysis
At the conclusion of data collection, we extracted all data from Qualtrics and examined univariate and bivariate distributions for outliers. We excluded responses with missing data on age or sex. We tabulated data and used the Pearson chi-square to test for independence between variables, utilizing Stata version 13 (StataCorp) with a 2-sided alpha level of .05. We stratified analysis by sex to investigate effect modification.
Results
Demographics
A total of 985 ultimate players responded to the questionnaire. Twenty responses were excluded because respondents were under 18 years of age, and an additional 175 were excluded because of incompleteness. Of the remaining 790 responses, 553 (70.00%) respondents identified as male, while 234 identified as female (29.62%), and 3 (0.38%) identified as neither category (Table 2). Because of insufficient responses in the “other” category, calculations were not performed using these responses.
Demographics of Ultimate Frisbee Players a

a Data are expressed as n (%) unless otherwise specified. GED, General Equivalency Diploma; N/A, not applicable.
b At the time of this study, the professional leagues included only male athletes.
c Athletes participating in the professional division were excluded from this analysis.
d Women are permitted to compete in the men’s division under certain circumstances, but men are not permitted to compete in the women’s division. As such, no chi-square analysis was performed on these data.
The mean time that respondents spent playing ultimate was 8.85 ± 5.71 years (range, 2-31 years) for men and 7.23 ± 4.77 years (range, 2-23 years) for women, with the majority of playing time spent at the club and college levels (Table 2). Male respondents played a mean of 8.54 hours of ultimate per week during the season, while women played a mean of 7.97 hours.
Concussion Cause and Actual Management
Of the 787 respondents (553 men and 234 women), 26.58% (n = 147) of men and 24.79% (n = 58) of women reported that they had sustained at least 1 concussion (P = .60) while playing ultimate (pooled frequency of 26.05%), with 45.58% (n = 67) and 43.10% (n = 25) of those men and women, respectively, reporting multiple concussions (Table 3), for a total of 237 concussions sustained by men and 101 concussions sustained by women.
Concussions Sustained While Playing Ultimate Frisbee a
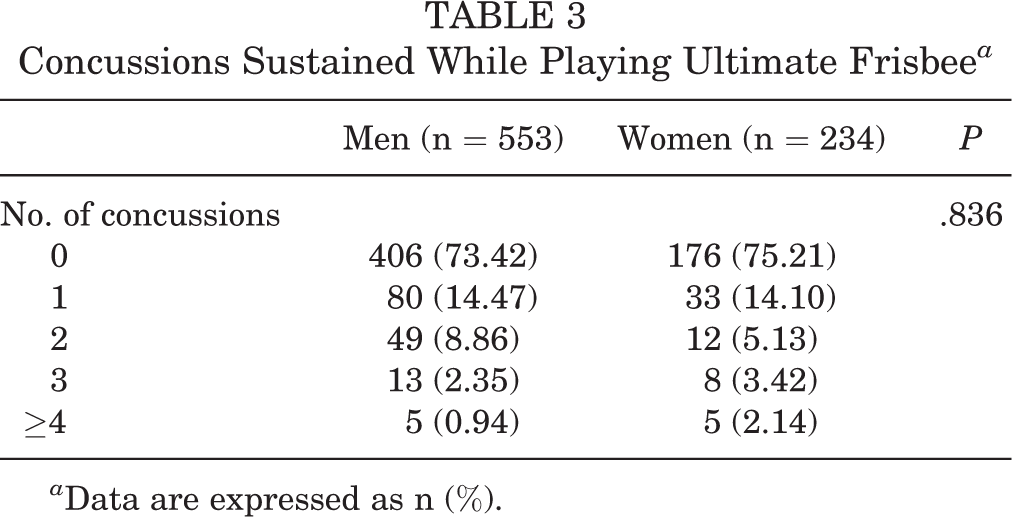
a Data are expressed as n (%).
The largest proportion of concussions occurred via head-to-ground contact and head-to-body contact, with relatively few via head-to-head contact and noncontact injuries. Regarding type of game, respondents reported that the vast majority of concussions occurred during tournament play. Complete details regarding the mechanism of the concussion as well as the level of play and type of game during which concussions occurred can be found in Table 4.
Concussion Cause and Management a

a Data are expressed as n (%).
b Concussions at the professional level were excluded from analysis because women did not participate in the professional leagues at the time of this study.
c Only a subset of respondents answered this question.
After a given concussion, 45.99% (n = 109) of men and 37.62% (n = 38) of women indicated that they returned to play in the same game or practice, while over 80% of both men and women who answered the question indicated that they either did not stop playing at all or returned in less than 1 hour. Of the respondents who answered the question (n = 132 for men and n = 41 for women), 28.03% of men and 31.71% of women reported that they were advised on whether they should return to play. Moreover, 39.24% (n = 93) of men and 46.53% (n = 47) of women stated that their symptoms had not yet disappeared before returning to play; 73.42% (n = 174) of men and 67.33% (n = 68) of women did not seek immediate medical attention for their concussion(s), and 76.79% (n = 182) of men and 59.41% (n = 60) of women did not seek follow-up attention, although women were significantly more likely to seek follow-up care than men (P = .001). The sources of medical attention sought can be found in Table 5.
Sources of Medical Attention Sought After Concussions Among Those Who Received Attention a

a Data are expressed as n (%). Multiple sources were often consulted after a given concussion. The percentages represent the percentage of total medical consultations conducted by a given type of health care professional. EMT, emergency medical technician.
b For the 63 concussions sustained by men for which immediate medical attention was sought, care came from 87 sources. For the 33 concussions sustained by women for which immediate medical attention was sought, care came from 44 sources.
c For the 55 concussions sustained by men for which follow-up medical attention was sought, care came from 79 sources. For the 41 concussions sustained by women for which follow-up medical attention was sought, care came from 49 sources.
Concussion Knowledge and Expected Management
All respondents (553 men and 234 women) reported their concussion knowledge and their anticipated concussion-related behavior and management. After seeing a list of concussion-related symptoms, 16.46% of men and 19.23% of women were surprised that those symptoms could indicate a concussion (Table 6). While approximately 80% of men and women felt that they would be able to recognize such symptoms in themselves (79.20% of men and 82.91% of women) or in teammates (82.10% of men and 82.05% of women), 32.19% of men and 21.79% of women stated that they would not necessarily remove themselves from play; men were significantly less likely to state that they would remove themselves from a game (P = .003). Furthermore, 27.57% of men and 25.00% of women stated that they would not necessarily wait until symptoms had resolved before returning to play, while 61.23% of men and 58.24% of women replied that they would not keep themselves out of play for at least 24 to 48 hours after the resolution of symptoms.
Concussion Knowledge and Expected Concussion Management a
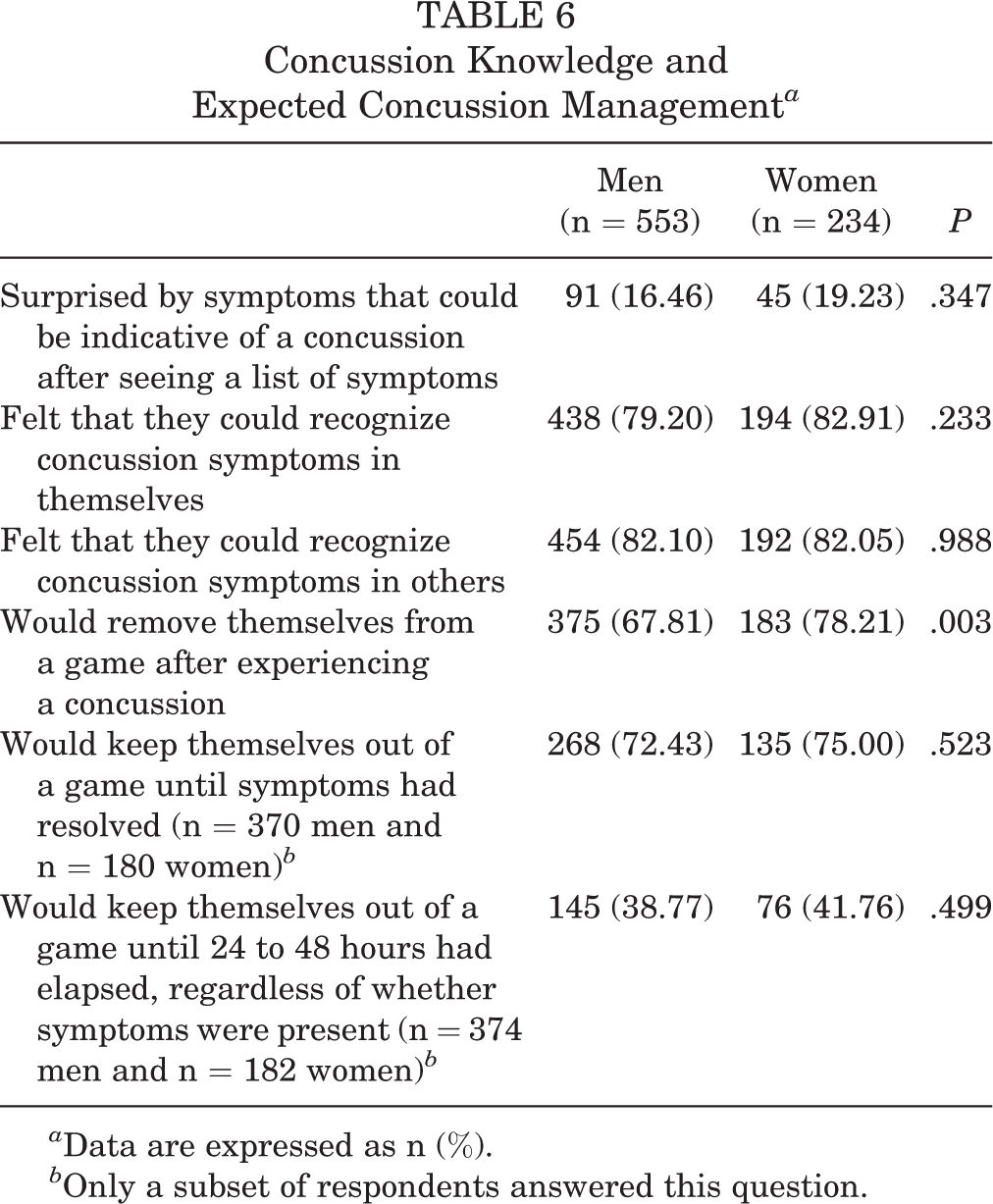
a Data are expressed as n (%).
b Only a subset of respondents answered this question.
Discussion
The current study took an initial step toward understanding the prevalence of concussions in ultimate Frisbee, as well as concussion knowledge and management among ultimate players. To our knowledge, this is the first study to investigate the prevalence of concussions in ultimate across varying levels of play while also ascertaining knowledge and postinjury behaviors. We found that 26% of competitive ultimate players reported having sustained a concussion, suggesting that a mild traumatic brain injury is a potential consequence of playing this sport. Furthermore, 43% of those who experienced a concussion returned to play in the same game, placing these athletes at an increased risk for second-impact syndrome and catastrophic injuries. 10 As approximately 17% of respondents were unaware of typical concussion signs and symptoms, this is not entirely surprising. Additionally, ultimate competitions are often not covered by health care providers, as they are typically played in recreational or club formats. Safety precautions around concussions in competitive ultimate conflict with international consensus statement guidelines 9 or NCAA regulations.
In terms of the management of concussive injuries in ultimate, while 83% of the sample indicated that they were aware of concussive signs and symptoms, over 25% of respondents reported that they would not remove themselves from the game; this admission was significantly more common in men. Importantly, the most recent international consensus statement from the Concussion in Sport Group (“Berlin guidelines”) recommends that after sustaining a sports-related concussion, athletes should not be permitted to return to play on the day of injury. 9 Further, athletes should not return to contact risk until an appropriate return-to-play protocol has been completed, which involves a 24- to 48-hour period of physical and cognitive rest, followed by a graduated, stepwise rehabilitation program over the course of approximately 1 week before returning to full activity. 9 This discrepancy between player behavior and expert guidelines suggests the need for more robust concussion education for ultimate players. It is possible that this need for education extends to other club sports played “under the radar” at the university level.
Patterns of concussions suggest high-risk settings for concussions in ultimate. Most concussions (68%) occurred during tournament play, when athletes generally compete in 4 to 8 games over 2 consecutive days of play; 17% of concussions occurred during nontournament games and only 15% during practices. These statistics are not surprising, as one would expect the lifetime prevalence of concussions to increase with additional athletic exposures (ie, tournament play compared with a single game) and increased athleticism and intensity (ie, college and club play compared with recreational leagues or high school).
This study also provides initial insight into what ultimate players know about concussions and how that knowledge may be dictating their behavior. Despite reporting familiarity with concussion signs and symptoms, many in our sample (17%) were surprised that certain signs and symptoms could be associated with a concussion. This suggests that ultimate players, like all competitive athletes, require further education about concussions. However, what might be more surprising was that over one-fourth of respondents indicated that they would not remove themselves from play if they were experiencing postconcussive symptoms. While this sentiment might be expected in a sport such as football, ultimate is a sport that is rarely supported by athletic training or medical providers. If the culture of toughness exists in a sport such as ultimate, colleges and universities responsible for their students’ physical welfare may need to better examine their risk management practices around club sports. We offer this advice with the understanding that athletes at all levels of competition are prone to doing all they can to remain in the game. Now, in this survey, we see that this is true in ultimate.
College ultimate is a club sport, and at most levels of play, it is self-officiated. As a club sport, it often receives minimal medical attention or access to athletic training services. In our study, 71% of respondents who believed that they were concussed did not receive any advice regarding return to play. Thus, the majority of concussed ultimate players make their own decisions regarding their readiness to return to competition after a concussion. As repeat concussions are a likely source of serious injuries 2 or longer recovery times, 12 this finding is of particular concern. Also, 72% of concussed ultimate athletes did not seek follow-up care for their injury; women were more likely to seek this care than men.
While 71% of respondents stated that they would remove themselves from play if they suspected a concussion, only 57% reported actually doing so after sustaining a concussion. This disconnect between reported intentions and actual behaviors is concerning and furthers the need for not only education but also much better surveillance and intervention in ultimate. In light of these findings, we recommend the institution of several changes in the landscape of competitive ultimate in an attempt to promote concussion management practices that are consistent with current guidelines and risk prevention best practices.
At the collegiate level, teams should have access to certified athletic trainers for both the identification and acute-to-postacute management of concussions. This should extend to tournament play as well. While ultimate is governed by the “Spirit of the Game” principle, at higher level tournaments and during professional play, referees (or limited referees, referred to as “observers” in ultimate) are part of the game. Extending the presence of referees or observers to lower stakes matches will aid in the identification of concussions while also helping to reduce “dirty play.” Most importantly, ultimate players need better education regarding concussion management. If our aforementioned suggestions will not be taken, and ultimate remains self-officiated and self-coached, then it is incumbent upon the players to know what to do to keep themselves and their teammates safe in the event of a suspected concussion.
We believe that USA Ultimate is well positioned to provide concussion management education across all levels of ultimate competition except the professional level, although professional players typically rise through the competition levels overseen by USA Ultimate and would be accessible for concussion-related education at those levels of play. At the college level, such a curriculum could be delivered in partnership with the school’s wider concussion management policies and procedures for all athletes. Such education should cover the biological and behavioral aspects of concussion, along with programmatic considerations, such as the steps toward recovery, what athletes should generally expect, and which medical providers they should seek out for treatment. Finally, in an effort to further the field’s understanding of concussions in ultimate, we recommend that USA Ultimate sponsor concussion surveillance projects at all major tournaments. This would allow for the systematic collection of reliable injury data in ultimate.
Limitations to Internal Validity
To estimate the true prevalence and determinants of concussions in ultimate players, the ideal design would be a prospective cohort, following a nationally representative random sample of competitive players at various levels. Our study was a cross-sectional design, with retrospective self-reporting, and thus suffers some limitations.
Our data on ultimate players come from a convenience sample obtained from snowball sampling. We were thus unable to calculate an exact response rate, given the unknown denominator, but we estimate that it was around 25%. It is possible that some athletes who initiated the survey upon receiving the email invitation were motivated to respond because they had experienced concussions in the past; such a response bias would overestimate the true prevalence of concussions. However, even in the hypothetical case in which all survey recipients who sustained an ultimate-related concussion responded to the survey, and all nonrespondents were concussion free, we would still find a clinically significant 6% prevalence of concussions (assuming 3500 unique recipients of the survey as discussed previously). Conversely, it is possible that our sample reflects survivorship bias in that athletes who experienced severe concussions no longer play ultimate and thus would not have received the survey; this would result in an underestimate of the true prevalence. Given the multiple potential sources of sampling bias, it is not possible to determine how our estimate of the lifetime prevalence of concussions in ultimate might have been affected.
The self-reported nature of our survey also raises the possibility of information bias. In an ideal, prospective surveillance study, injuries would be closely observed and diagnosed via consistent, predetermined criteria. In contrast, simply asking respondents about their concussion history could result in an overestimate or underestimate. We attempted to mitigate this issue by providing a clear definition of a concussion, with signs and symptoms. One could argue that asking about self-diagnosed (instead of physician-diagnosed) concussions could result in misclassification; on the other hand, given that many concussions sustained during sports are likely to go undiagnosed, 5 asking about self-diagnosed concussions does not discount these findings.
Limitations to External Validity and Future Research
Our estimate that 26% of players have experienced a concussion while playing ultimate is derived from a convenience sample of athletes, representing a variety of competitive levels and geographic areas. USA Ultimate reports that 70% of their members are male, with an age distribution similar to our sample, which assuages some concern that our sample is biased with respect to those 2 important variables. 16 It is unknown whether similar estimates of concussions would be seen internationally, at the high school level, or within select subgroups of the sport (eg, “pickup” games, beach ultimate, etc). Similarly, given our sampling methodology, it is not clear that our snapshot prevalence estimate can be generalized to the current population of competitive ultimate players in the United States, let alone to the changing landscape of this sport, as it increases in popularity and players become faster, stronger, and more specialized.
As discussed previously, other studies 7,17 have followed well-defined cohorts prospectively but have had substantially smaller sample sizes spread across far fewer levels and forums of play; those studies also did not examine the lifetime prevalence of injuries. We chose our convenience sampling method to capture as large a number of current athletes as possible. While we have been able to estimate a lifetime prevalence of concussions in ultimate and have begun to characterize the concussions experienced as well as to assess players’ knowledge and expected concussion management behaviors, there is a great deal of uncertainty in our estimates. To estimate the incidence of concussions in ultimate to better determine the health risk posed to athletes, future studies should examine injuries in a prospective manner, with well-defined study populations and objective measures of both recording and reporting concussions.
Conclusion
Concussion research is regularly plagued by the issue of subjective reporting, with the study of ultimate being no exception, given that ultimate is a sport that has never been included in large-scale surveillance studies. As such, the precise number of identified concussions is challenging to ascertain, although our data showing that 26% of competitive ultimate athletes have sustained a concussion while playing ultimate, that 43% of those have sustained multiple concussions, and that 43% returned to play in the same game or tournament after sustaining the injury do indicate a potentially serious injury risk from this sport. Therefore, at this time and for a pilot study such as ours, collecting self-reported information, with its many inherent limitations, is an important first step in deepening our understanding of this issue.
Sports concussions are a major public health concern. With the knowledge that concussions do occur in ultimate Frisbee, it is time for national and regional organizations to take a second look and stronger stance at how we approach club sport concussion management.
Footnotes
Acknowledgment
The authors thank Mary Lazar, PsyD, and Sean McCormick, PhD, for their assistance with the development of this project many years ago.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by the Dartmouth College Committee for the Protection of Human Subjects (study No. 00028872).