
Abstract
Background:
Lower leg chronic exertional compartment syndrome (CECS) is usually diagnosed in young and athletic individuals. The presence of CECS in older patients has received little attention in the literature, and patient characteristics are unknown.
Purpose:
To determine the prevalence of CECS in older patients (≥50 years) and to assess whether older patients with CECS differ clinically from younger patients with CECS.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All individuals with exercise-induced lower leg pain who visited a referral center for CECS between January 2001 and December 2013 were eligible for analysis. Patients were included if history, physical examination, and dynamic intracompartmental pressure measurement indicated CECS. Characteristics of patients 50 years of age or older were compared with characteristics of patients younger than 50.
Results:
A total of 698 patients with CECS were included: 98 patients were aged 50 years or older and 600 patients were younger than 50 years. Older individuals more often reported a history of lower leg events or comorbidities (≥50 years, 45% vs <50 years, 25%; P < .01) and unilateral symptoms (≥50 years, 45% vs <50 years, 22%; P < .01). Most older patients (62%) did not participate in sport or only walked or hiked, whereas the same was true of only 7% of the younger population. Pain (≥50 years, 94%; <50 years, 96%) and tightness (≥50 years, 57%; <50 years, 62%) were the predominant symptoms of CECS in both groups. Type of CECS differed significantly (P < .01); the anterior muscle compartment was involved more frequently in older patients (≥50 years, 82% vs <50 years, 59%) and deep flexor muscle CECS was more often diagnosed in younger patients (≥50 years, 26% vs <50 years, 53%).
Conclusion:
In the present population, 1 in 7 patients diagnosed with lower leg CECS was 50 years of age or older. These individuals were less active and had more comorbidities than patients younger than 50 years. Older individuals predominantly have anterior CECS. Clinicians should consider CECS in older individuals with exercise-induced lower leg pain, particularly if it is unilateral.
Lower leg chronic exertional compartment syndrome (CECS) is an exercise-induced condition characterized by pain and tightness. 1,2 Cramps, muscle weakness, and even diminished skin sensation may also be reported. 8,26 Symptoms usually disappear after 30 minutes of rest. 28 A combination of a characteristic history and physical examination may suggest the diagnosis of CECS, and additional diagnostic tests, such as dynamic intracompartmental pressure (ICP) measurements, are used to confirm the diagnosis. 15
CECS is a condition mainly described in young and active individuals. 5 Known characteristics of patients with CECS are largely based on cohorts of athletes and military personnel. 4,25 Only 2 studies have reported on CECS in older individuals or in patients with comorbidities. 9,10 Therefore, the occurrence of CECS in older patients with exercise-induced lower leg pain is unknown. Also, characteristics of these older patients with CECS may differ from the characteristics of the young and athletic populations with CECS described in the literature.
Our facility is a referral center for individuals with exercise-induced lower leg syndromes. We increasingly see older patients who are diagnosed with lower leg CECS. The aim of the present study is twofold: first, to determine the occurrence of CECS in individuals 50 years or older with exercise-induced lower leg complaints who were evaluated for CECS; and second, to identify potential differences between older and younger individuals with CECS. Results of the study may increase awareness among health care workers regarding CECS in older patients.
Methods
Máxima Medical Center serves as a referral center for exercise-induced extremity syndromes. 20,24,27 Yearly, at a dedicated outpatient facility, our department of sports medicine evaluates approximately 225 individuals suspected of having CECS. Patients with exercise-induced symptoms of the extremities are referred by sports physicians, orthopaedic surgeons, neurologists, general practitioners, or other health workers. All procedures in the current study complied with the Declaration of Helsinki, and the hospital’s medical ethics committee approved the study protocol.
Consultation and Patient Selection
Each patient with exercise-induced lower leg complaint was evaluated by an experienced sports physician. Patients underwent a standardized physical examination including assessment of general health and posture, lower leg inspection, palpation of the muscle compartments, and palpation of distal arterial pulses. If CECS was deemed possible based on a suggestive history (predictable lower leg pain and tightness during and/or after exercise or physical activity) and other diseases were excluded during physical examination, a dynamic ICP measurement was performed. Physical examination consisted of inspection and palpation of the legs and, if indicated, assessment of the vascular and nervous system. Pressure was measured only in lower leg compartments that were suspected of having CECS based on the location of the complaints and findings during physical examination. To further minimize the number of invasive measurements and potential complications, only the most symptomatic leg was measured.
ICP was measured initially with the patient at rest and then directly after, 1 minute after, and 5 minutes after a standardized provocative treadmill test. If patients were unable to generate sufficient complaints, they were encouraged to hop and/or climb stairs. A more detailed description is given in previous reports. 6,26 Intracompartmental muscle pressure was considered elevated if it met or exceeded 1 or more of the following cutoff points: 15 mm Hg during rest, 30 mm Hg at 1 minute after provocation, or 20 mm Hg at 5 minutes thereafter. 15 Patients received the diagnosis of CECS if their history, physical examination, and measured ICP values were consistent with CECS.
All patients evaluated for lower leg CECS between January 2001 and December 2013 were eligible for the present study. Only patients who were diagnosed with CECS based on a suggestive history, a matching physical examination, and elevated ICP were included. Some patients were evaluated for CECS more than once during the study period. Only their first visit was included, whereas evaluations (including ICP measurement) that followed were excluded.
Data Collection and Statistics
We extracted data from 2 sources and composed 1 comprehensive data file. Between January 2001 and March 2010, we retrieved data from a custom-made Microsoft Access database that was supplemented by data from archived paper patient files. Between April 2010 and December 2013, data were retrieved from standard electronic patient hospital files. Only variables that were obtained in more than 50% of the patients were used in the present study. Peripheral artery disease, venous insufficiency, nerve conditions, major traumatic events, and other significant lower leg events and comorbidities were tabulated. The following variables were excluded from this report: influence of complaints on level of sports, activities provoking symptoms, and exercise duration before the symptoms began.
Analysis was performed by use of SPSS Statistics, Windows version 22.0.0.0. When normally distributed, data were expressed as mean ± SD; nonparametric data were expressed as median (with range). Differences in categorical baseline characteristics were assessed with a chi-square test, and a Mann-Whitney test was used to analyze continuous variables (ie, duration of complaints). A P value less than .05 was considered significant.
Results
Patient Selection
During the 13-year study period, 1765 patients with exercise-induced lower leg pain were referred to our hospital for evaluation. In 153 patients, history and physical examination suggested a condition other than CECS. After exclusion of 201 patients who were previously evaluated in our hospital for CECS, 1411 unique patients remained. Based on a combination of history, physical examination, and elevated ICP, CECS was diagnosed in 698 patients (49%) (Figure 1). The prevalence of CECS in evaluated patients who were 50 years or older was 38% (98/255), and in patients younger than 50 years it was 52% (600/1156). The current report is focused on the 698 patients diagnosed with CECS.

Study flow chart of patients evaluated for chronic exertional compartment syndrome (CECS) in a referral center. ICPM, intracompartmental pressure measurement.
Patient Characteristics
There were no differences in sex or duration of complaints between patients with CECS who were 50 years or older (n = 98) and patients younger than 50 (n = 600) (Table 1). Older patients with CECS more often had relevant comorbidities (peripheral artery disease, venous disease, major nerve conditions, significant bony or soft tissue disorders) (Table 1). Older patients also had received less physical therapy (57% vs 80%; P < .01) and fewer orthotic devices (47% vs 62%; P = .05) than younger patients. Bilateral complaints were seen less often in the older population (55% vs 78%; P < .01).
Characteristics of Patients Aged ≥50 and <50 Years Diagnosed With Lower Leg Chronic Exertional Compartment Syndrome (CECS) a
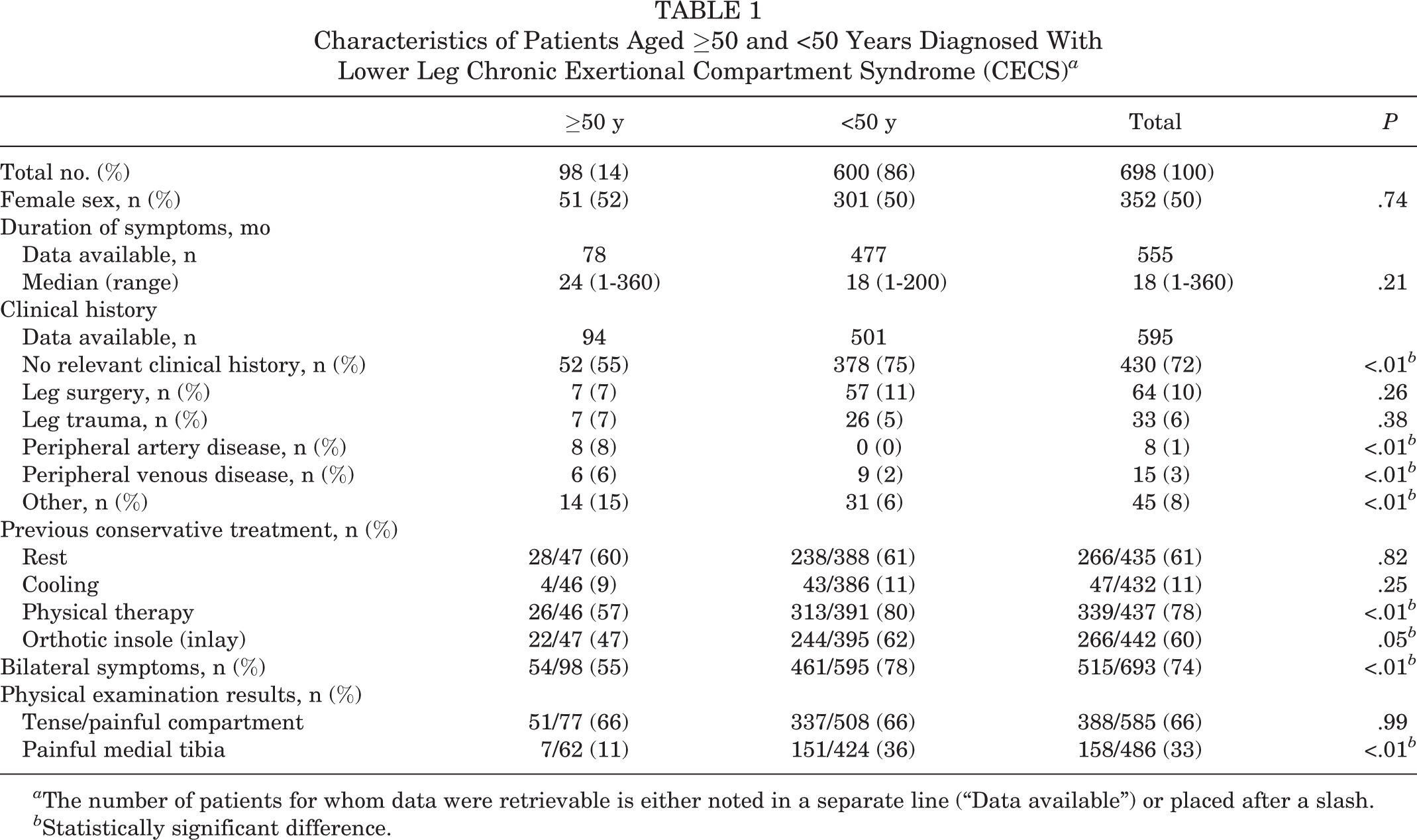
a The number of patients for whom data were retrievable is either noted in a separate line (“Data available”) or placed after a slash.
b Statistically significant difference.
Sport Activities
The type and level of sports differed significantly between the older and younger patients with CECS (Table 2). Interestingly, 62% (51/82) of the patients 50 years or older did not participate in sports or engaged in only hiking or walking. In contrast, the same was true of only 7% (38/552) of patients younger than 50. Furthermore, patients 50 years or older were significantly less engaged in competitive sports, as only 5% (3/66) practiced sports on a competitive level. Conversely, 69% (270/392) of the younger patients practiced sports on a competitive or professional level.
Sport Activities of Patients Aged ≥50 and <50 Years Diagnosed With Lower Leg Chronic Exertional Compartment Syndrome (CECS) a
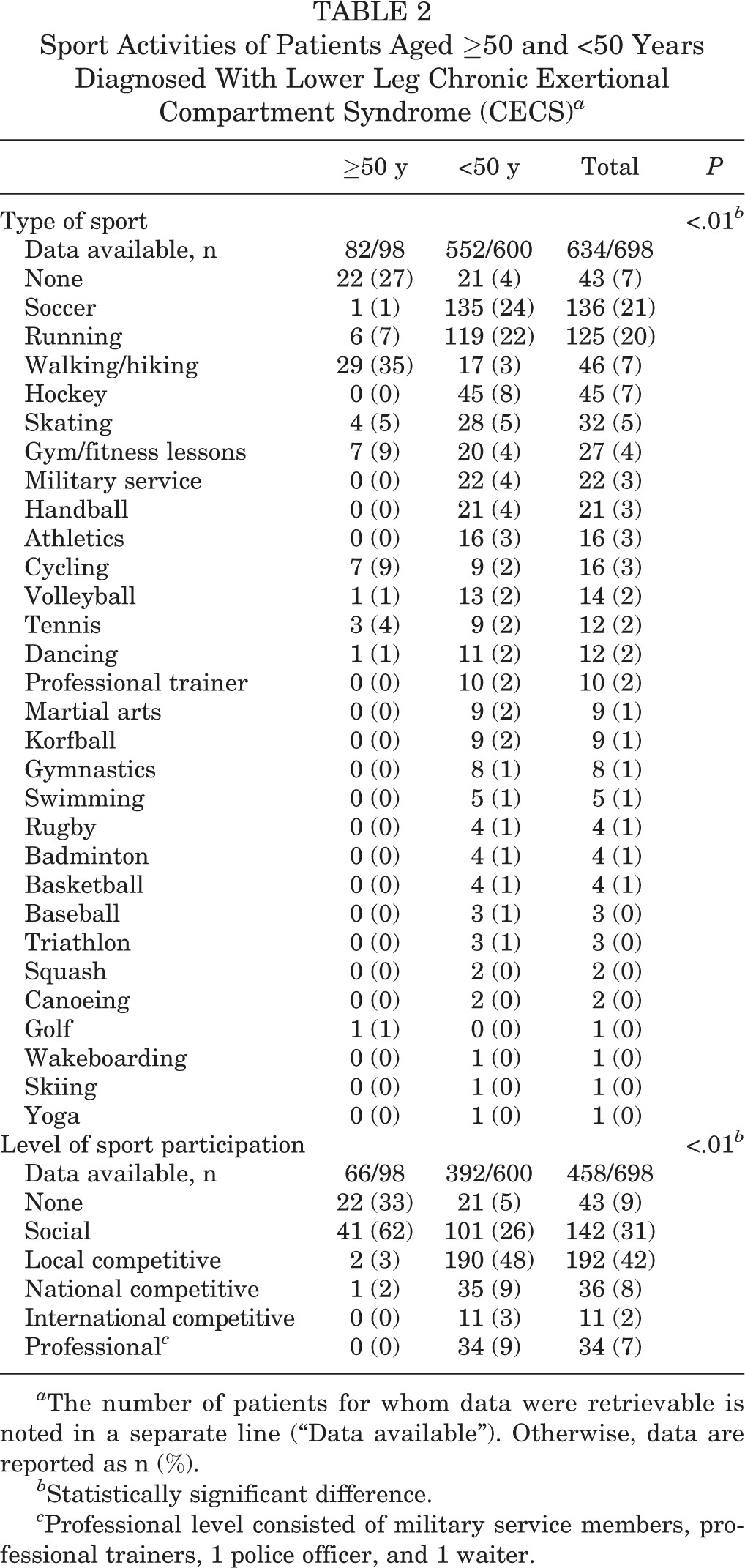
a The number of patients for whom data were retrievable is noted in a separate line (“Data available”). Otherwise, data are reported as n (%).
b Statistically significant difference.
c Professional level consisted of military service members, professional trainers, 1 police officer, and 1 waiter.
Symptoms
CECS symptoms were comparable in both groups (Table 3). Almost all patients reported pain as their main symptom (≥50 years, 94%; <50 years, 96%; P = .61). Tightness was also present in a majority of patients (≥50 years, 57%; <50 years, 62%; P = .38). Only a minority reported cramps, muscle weakness, and altered skin sensation (Table 3). Physical examination revealed the same proportion of the 2 groups had a tense or painful compartment (both 66%, P = .99). A painful medial tibial rim during palpation was found more often in younger patients (≥50 years, 11%; <50 years, 36%; P < .01).
Symptoms and Physical Examination Results in Patients Aged ≥50 and <50 Years Diagnosed With Lower Leg Chronic Exertional Compartment Syndrome (CECS) a

a All results are presented as n (%). The number of patients for whom data were retrievable is placed after a slash.
b Statistically significant difference.
Affected Compartments
A statistically significant difference was found between older and younger patients with respect to the affected lower leg muscle compartments (Table 3). Most older patients (82%) were diagnosed with anterior CECS (either isolated or in combination with other compartments), and 26% of the older patients were diagnosed with deep flexor CECS. In contrast, 59% of the younger patients were diagnosed with anterior CECS and 53% were diagnosed with deep flexor CECS. In both age groups, a similar proportion was diagnosed with lateral CECS (≥50 years, 12%; <50 years, 11%). ICP data regarding the anterior, deep flexor, and lateral compartments were comparable between the 2 groups of patients (Figure 2).

Lower leg muscle intracompartmental pressures (ICPs) before and after a standard provocative treadmill test in patients with chronic exertional compartment syndrome (CECS) who were 50 years or older and those younger than 50 years. For each separate compartment, we included only patients diagnosed with CECS in that specific compartment.
Discussion
Current knowledge of CECS is based almost exclusively on cohorts of young and athletic individuals. 4,25 However, the condition has occasionally been reported in slightly older patients or in patients with comorbidities. 9,10 The prevalence of CECS in persons over 50 years of age is unknown. The present study demonstrates that CECS is not limited to young and active individuals, as 14% (98/698) of all patients diagnosed with CECS at our facility were 50 years or older. Although these older patients with CECS mostly refrained from competitive sports, we suspect that increased physical activity due to increased leisure time may induce complaints. Moreover, patients 50 years or older more often had unilateral complaints, and the deep flexor compartment was seldom involved.
CECS is often overlooked as the cause for exercise-induced lower leg pain. For instance, diagnostic delay in one study was up to 7 years. 18 The duration of exertional pain was 4 years in a study of diabetic patients with CECS whose age ranged from 18 to 72 years 9 ; during this period, these patients with undiagnosed CECS may have undergone a host of diagnostic tests and treatments. In the absence of a diagnosis explaining their exertional leg pain, patients may curtail their physical activity. Diminished participation in sports and exercise may result in a decreased health status and quality of life. 14 The present study also found an extended delay in some older patients (up to 360 months) prior to arriving at the diagnosis, although this diagnostic delay was not statistically significant compared with younger patients (median, 24 vs 18 months). Therefore, awareness among health care providers regarding the potential presence of CECS in any age group must be improved.
The majority of CECS studies report on cohorts of highly active individuals, most of whom participate in competitive sport activities. 4 The present report demonstrates that CECS may also occur in older patients who are not necessarily engaged in competitive sports. Most patients had complaints during everyday activities or during hiking or walking. Although these patients do not participate in competitive sports, they are relatively active. We hypothesize that these older individuals increased their physical activities as leisure time became more available to them. Most studies have found that patients with CECS do not have any relevant comorbidities or history of lower leg abnormality. 8,22 In contrast, the only 2 studies describing older patients with CECS found that a significant proportion of these patients reported relevant comorbidities such as diabetes, cardiovascular disease, or previous trauma. 9,10 As might be expected, the present study also found that rates of earlier lower leg surgery, trauma, or relevant comorbidities were higher in the population 50 years or older than in the population younger than 50. Hence, we emphasize that comorbidities or previous lower leg events such as surgery do not exclude the presence of CECS in older patients.
At present, uniformity is lacking in regard to describing the frequency and intensity of symptoms associated with CECS. However, exertional pain is universally accepted as the dominant symptom. 13,17,21 Two studies in older patients with CECS found that all patients experienced pain, whereas only a minority experienced tightness, cramps, muscle weakness, or altered skin sensation. 9,10 The present study confirms these findings. Interestingly, these 5 symptoms were seen at similar rates in the older and younger populations. In the present study population, pain (95%) and tightness (62%) characterized CECS in both older and younger patients.
Individuals with lower leg CECS have been reported to have predominantly bilateral anterior compartment involvement. 5,23 The two studies in older patients with CECS also reported predominant involvement of the anterior compartment. 9,10 However, deep flexor CECS is common, as recognized in recent reports. 28 In the present population, 82% of all older patients had involvement of the anterior compartment, whereas this percentage was limited to little over half of the younger patients. Conversely, only 1 in 4 older patients had involvement of the deep flexor compartment, compared with over half of younger patients. We found a higher prevalence of unilateral complaints in older patients with CECS (45%) than in younger patients (22%). The rate of unilateral complaints in our older population is remarkably higher than in other studies. 3,7,12 We suspect that this higher rate of unilateral CECS may be related to a higher rate of mainly unilateral comorbidities in our older patients with CECS. Unfortunately, the current dataset is too limited to explore this potential relation.
Our study has some limitations. Its retrospective design limited the number of variables we were able to include in the analysis, and missing data may have introduced information bias. Furthermore, the retrospective design prevented us from thoroughly exploring relations between several variables. Operative results and outcome data were not available, as most patients were treated in other hospitals. In the absence of operative results, ICP measurements were used to confirm the diagnosis of CECS. The absolute role of elevated ICP values is currently under debate. 11,16,19 However, we believe that a combination of a suggestive history, physical examination, and elevated ICP values is sufficient to diagnose patients with CECS. Last, because we are a referral center, our population is highly selective, and the incidence of CECS in other populations of patients with exercise-induced lower leg pain may be lower.
In conclusion, CECS may occur in individuals 50 years or older with exercise-induced lower leg pain. These patients are less active and more often have sustained previous lower leg events or comorbidities than younger patients with CECS. In older individuals, CECS is more often localized in the anterior compartment rather than the deep flexor compartment. Clinicians should be aware that lower leg exertional pain in older patients may be caused by CECS. These patients may present differently than younger patients with CECS.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by the medical ethical research committee at Máxima Medical Center.