
Abstract
Background:
Meniscal and chondral lesions are commonly associated with anterior cruciate ligament (ACL) tears, and these lesions may play a role in patient outcomes after ACL reconstruction.
Purpose:
To determine the effects of the presence and location of meniscal and chondral lesions at the time of ACL reconstruction on patient-reported outcomes at a minimum 2-year follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with no prior knee surgery who underwent primary ACL reconstruction by a single surgeon between 2010 and 2014 were included in this study. Those meeting inclusion criteria were divided into the following groups based on the arthroscopic diagnosis: patients without concomitant meniscal or chondral lesions, patients with isolated meniscal lesions, patients with isolated chondral lesions, and patients with both chondral and meniscal lesions. Patient-reported outcomes (Short Form–12 [SF-12] physical component summary [PCS] and mental component summary [MCS], Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC], and Lysholm scale) were assessed at a minimum of 2 years from the index surgery.
Results:
A total of 151 patients met the inclusion criteria and were included in the study. The mean age at the time of surgery was 36.2 years (range, 14-73 years), and the mean follow-up was 3.2 years (range, 2.0-5.6 years). At the time of surgery, 33 (22%) patients had no concomitant lesions and served as the control group, 63 (42%) patients had isolated meniscal lesions, 21 (14%) patients had isolated chondral lesions, and 34 (22%) patients had both chondral and meniscal lesions. There was significant improvement in all outcome scores postoperatively for the 3 groups (P < .05 for all outcome scores). The presence of a meniscal tear and laterality of the meniscal lesion did not have a negative effect on any postoperative outcome scores. Patients with isolated chondral lesions had significantly lower postoperative WOMAC scores compared with patients without chondral lesions (P < .05). No significant differences were found for all other scores. Patients with patellofemoral chondral lesions had significantly lower postoperative SF-12 PCS and Lysholm scores than patients with tibiofemoral chondral lesions (P < .05).
Conclusion:
Patients with ACL tears achieved improved functional scores at a mean 3.2 years after ACL reconstruction. While meniscal lesions did not affect postoperative outcomes in the short term, chondral lesions were identified as a predictor for worse outcomes.
An anterior cruciate ligament (ACL) tear is one of the most common orthopaedic injuries in the United States. 12 Moreover, 30% to 60% of ACL tears are associated with meniscal or chondral injuries at the time of their index reconstruction, 3,7,8 with studies reporting that patients who present with a focal cartilage injury or prior meniscectomy had a more rapid progression of osteoarthritis from the baseline examination at the time of primary ACL reconstruction. 9,16 Although the effects of chondral and meniscal lesions at the time of ACL reconstruction have been described in multicenter studies, the effects of the specific chondral and meniscal injury locations and grades have not been characterized in a single-surgeon series. This information is crucial for surgical planning, patient expectation management, and delineation of long-term outcomes based on specific injury patterns.
Given the need to better understand the effects of specific associated lesions on ACL reconstruction, the primary aim of this study was to evaluate the effect of concurrent meniscal tears and subsequent treatment on patient outcomes at the time of ACL reconstruction. A secondary aim was to identify the location and severity of chondral defects found at the time of ACL reconstruction and to determine their impact on postoperative outcomes. We hypothesized that patients with meniscal tears at the time of primary ACL reconstruction would have worse outcomes than patients without meniscal tears. Moreover, it was hypothesized that patients with focal cartilage lesions at the time of surgery would have worse outcomes than patients without focal cartilage lesions. Finally, we hypothesized that patients who had more severe chondral lesions, defined as grade III or IV on the Outerbridge classification, 4,5 would have worse outcomes than patients with less severe lesions.
Methods
Patient Selection
This retrospective study of prospectively collected data was approved by the institutional review board of our institution (No. 2002-03). Patients of any age with closed physes who underwent primary ACL reconstruction with either chondral or meniscal lesions performed by a single surgeon between 2010 and 2014 were included. Exclusion criteria included any prior surgery on the studied knee as well as patients with any concomitant injuries at the time of surgery besides cartilage and meniscal lesions.
Patient Demographics
Collected patient demographic data included age, chondral lesion location and grade at the time of surgery, and meniscal tear type and laterality. Operative reports and all available imaging scans were reviewed for each patient included in the study to check for additional pertinent findings and to document chondral and/or meniscal lesion treatment procedures. Furthermore, patient range of motion and ligamentous stability findings were recorded both preoperatively and postoperatively.
Chondral lesions were graded intraoperatively by the surgeon (R.F.L.) based on the Outerbridge classification. 5 Additionally, all lesions were grouped by location into either tibiofemoral or patellofemoral. If 2 lesions had the same grades in one patient, the lesion with the greatest area was assigned to the patient. Meniscal tears were also identified and classified intraoperatively by location (medial, lateral, or bicompartmental) and morphology (horizontal, vertical, or other).
Patient Subjective Outcomes
Patients completed a subjective questionnaire preoperatively and at a minimum 2 years postoperatively. Survey data included the Short Form–12 (SF-12) physical component summary (PCS) and mental component summary (MCS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Lysholm scale. All patients were administered the electronic questionnaire at the time of the initial office visit and then again during follow-up visits or via email if unable to come in for a clinic visit.
Surgical Technique
Patellar tendon autografts were the graft of choice. Patellar tendon allografts were chosen for patients older than 45 years or for those who elected against an autograft. For patellar tendon allografts, the grafts were harvested first, followed by arthroscopic surgery. An accessory medial arthroscopic portal was made to localize the native ACL footprint. A bur hole was placed midway between the anteromedial and posterolateral bundle attachments and posterior to the lateral intercondylar ridge as a reference. 18 Using an over-the-top guide and a 10-mm low-profile reamer, the femoral ACL tunnel was carefully reamed, ensuring preservation of a sufficient posterior wall (1-2 mm) of the femoral cortex. A passing suture was placed into the femoral tunnel for later graft passage. Next, the location of the tibial tunnel was identified using the remnant stump of the native ACL. If the native ACL tibial stump was unidentifiable, then the margins of the anterior horn of the lateral meniscus were utilized to locate the tibial ACL attachment site. 18 Using an acorn reamer (Arthrex), the tibial tunnel was formed and then the apertures smoothed with a small rongeur and a handheld 10-mm reamer. The passing suture was pulled down the tibial tunnel, and the graft was pulled into the femoral tunnel and fixed into the femur with a titanium screw. The graft was then pulled firmly to ensure solid fixation in the femoral tunnel, and the knee was cycled 20 times while applying tension to the passing sutures in the tibial bone plug to eliminate any residual graft laxity. Next, the graft was fixed into the tibial tunnel with a titanium screw with the knee in full extension. Graft placement was verified arthroscopically, and the Lachman test confirmed that the graft had eliminated pathological anterior translation.
Rehabilitation
All patients were allowed to bear weight as tolerated upon discharge and were told to use crutches for the first 2 weeks. Physical therapy commenced 24 hours after surgery to initiate early range of motion and muscle reactivation and to control edema. Rehabilitation included straight-leg raises in an immobilizer until the patient was able to perform them without any extension sag. It was anticipated that patients would not return to full activities until a minimum of 9 months postoperatively.
Statistical Analysis
Statistical analyses were performed using SPSS version 23.0 (IBM). Statistical power was considered for this study in terms of the effect size detectable when testing the primary hypothesis given the fixed sample size. Assuming 2-tailed testing, an alpha of 0.05, and an independent-samples t test, 21 patients per group was sufficient to detect an effect size of d = 0.79 with 80% statistical power. The Kolmogorov-Smirnov test was used to show the normal distribution of all used scores. To address this study’s primary aim of characterizing the effect of meniscus and cartilage lesions on outcome scores in ACL-reconstructed patients, 2-factor analysis of variance (ANOVA) models were constructed. The interaction of these 2 covariates was tested and removed from the model when not significant. When reporting models with no interaction, the meniscus and cartilage terms were interpreted to have independent effects. A 1-factor ANOVA was used to assess differences between patient outcomes of different meniscal lesion locations. The paired 2-tailed Student t test was used to detect differences between preoperative and postoperative outcome scores for all outcome measures.
Results
Patient Demographics and Graft Type
An initial database query yielded 230 patients who underwent isolated, primary ACL reconstruction between 2010 and 2014. After applying inclusion and exclusion criteria, 171 patients remained. Of these 171 patients, 151 (88%) patients met the inclusion criteria and had a minimum 2-year follow-up (mean, 3.2 years [range, 2.0-5.6 years]). Demographic data and cohort-wide improvement in patient-reported outcome scores are shown in Tables 1 and 2, respectively. The distribution and characteristics of concomitant injuries are also reported in Table 1. Concomitant intra-articular lesions were treated as follows: 4 chondral lesions were treated with microfracture, while the remaining 51 were treated with chondroplasty. Meniscal lesion treatments are detailed in Table 1; all meniscal repair procedures were performed using the inside-out technique with vertical mattress sutures. All meniscal root tears (n = 15 patients) were treated with 2-tunnel transosseous repair. 2,11
Patient Characteristics and Concomitant Injuries a

a ACL, anterior cruciate ligament.
Overall Preoperative and Postoperative Outcome Scores a

a MCS, mental component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Significant at P < .05.
Complications and Reoperations
Four patients required revision ACL reconstruction at a mean of 19.1 months postoperatively, while 1 patient underwent deep hardware removal at 19.5 months postoperatively. One patient suffered a traumatic meniscal tear 2 years postoperatively, 1 underwent a subsequent osteochondral allograft procedure, and 1 underwent total knee arthroplasty.
Results of 2-Factor ANOVA Models
No significant interaction between chondral and meniscal lesions was identified. This indicates that meniscal and chondral lesions affected outcomes independently and did not influence each other (Table 3).
Influence of Meniscal and Chondral Lesions on Postoperative Outcomes a

a A positive effect reports a higher score in the corresponding outcome and a negative effect a lower score. MCS, mental component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Significant at P < .05.
Patient-Reported Outcomes of Meniscal Lesions
Patients with isolated meniscal tears had significantly (P = .031) higher SF-12 PCS scores than patients without meniscal lesions. Further analysis of the patients with isolated meniscal tears revealed no significant difference in sex or age when compared with patients without concomitant meniscal tears (P > .05). Patients with meniscal tears were divided into isolated medial, isolated lateral, and bicompartmental groups. A comparison of the groups showed no significant association between patient-reported outcome scores and location of the meniscal tear. Meniscal lesion data are reported in Table 4.
Association Between Patient-Reported Outcome Scores and Location of the Meniscal Tear a

a A comparison of the 3 groups showed no significant association between patient-reported outcome scores and location of the meniscal tear. MCS, mental component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Patient-Reported Outcomes of Chondral Defects
For patients with isolated chondral lesions, the postoperative WOMAC score was significantly lower (P = .024) than for patients without chondral lesions. Patients with patellofemoral chondral lesions had significantly lower SF-12 PCS (P = .011) and Lysholm (P = .049) scores compared with patients with tibiofemoral chondral lesions. There was no significant difference in SF-12 MCS and WOMAC scores between these groups (Table 5). Patients with Outerbridge III and IV lesions had significantly lower SF-12 PCS (P = .018), WOMAC (P = .039), and Lysholm (P = .036) scores compared with patients with Outerbridge I and II lesions (Table 6).
Effect of Chondral Lesion Location on Patient-Reported Outcome Scores a
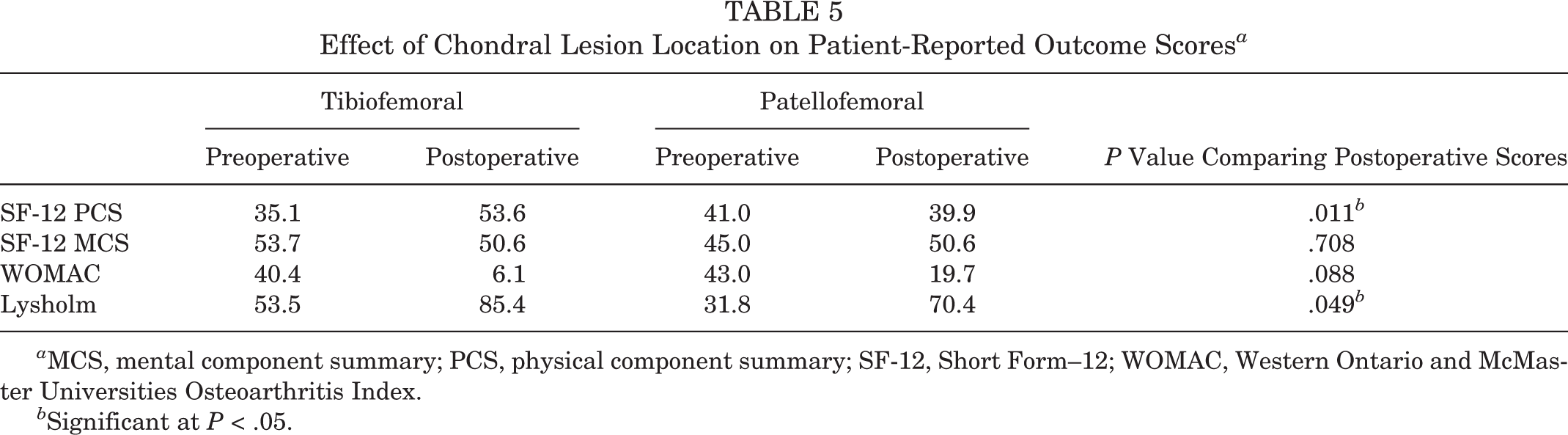
a MCS, mental component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Significant at P < .05.
Effect of Chondral Lesion Severity on Patient-Reported Outcome Scores a
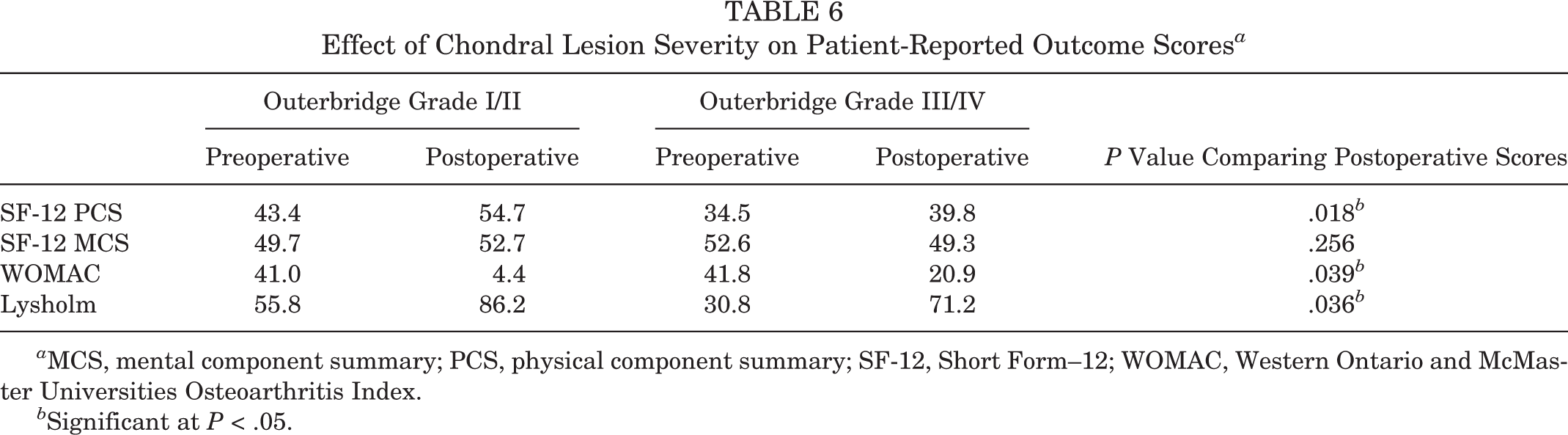
a MCS, mental component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Significant at P < .05.
Discussion
The most important finding of this study was that the presence of chondral lesions at the time of primary ACL reconstruction had a significant negative effect on WOMAC scores at a mean of 3.2 years’ follow-up. Furthermore, the location of the chondral lesions was significantly associated with outcomes, with patellofemoral chondral defects having worse postoperative SF-12 PCS and Lysholm scores compared with tibiofemoral chondral lesions. Patients with Outerbridge III and IV chondral lesions also had significantly worse SF-12 PCS, WOMAC, and Lysholm scores compared with patients with Outerbridge grade I and II lesions. The vast majority of chondral lesions were treated with chondroplasty, perhaps suggesting that more involved articular cartilage resurfacing procedures may be indicated for these patients. Contrary to our hypothesis, meniscal injuries did not lead to lower postoperative scores. The findings support our second hypothesis that focal, high-grade cartilage lesions are associated with decreased patient-reported outcome scores.
Our results demonstrated favorable SF-12 PCS scores in patients who had a concomitant meniscal tear necessitating repair but no significant difference in the other outcome scores. It should be noted, however, that more than half of the meniscal lesions in our cohort underwent repair, which may have mitigated the negative effects of meniscal injuries. LaPrade et al 10 found similar results at 2-year follow-up in a study using the Norwegian Knee Ligament Registry. Compared with patients undergoing isolated ACL reconstruction, those who underwent concomitant lateral meniscal repair, partial lateral meniscectomy, or partial medial meniscectomy did not have significantly different Knee injury and Osteoarthritis Outcome Score (KOOS) values. Meanwhile, patients who underwent concomitant medial meniscal repair demonstrated significantly worse outcomes on 2 KOOS subscales. The authors reported that the follow-up period was too short to determine a negative difference with the meniscectomy procedures. In another Scandinavian registry study, Rotterud et al 13 reported no significant differences in KOOS values at 2-year follow-up between patients with and those without associated meniscal lesions. In general, meniscus integrity has been demonstrated to affect knee stability in biomechanical studies 14,17 and outcomes in clinical studies 14,17 ; hence, meniscus preservation should always be attempted. It is possible that in the short term, the negative effects of meniscal lesions are not detected in these studies, and long-term studies are needed.
In the present study, patients with chondral lesions had significantly poorer WOMAC scores compared with patients without chondral lesions. In addition, patients with high-grade chondral lesions had significantly poorer outcomes compared with those with partial-thickness defects. Ahn et al 1 assessed the outcomes of 40 patients based on concomitant injury patterns at a minimum 3 years after revision ACL reconstruction. The authors noted that patients with Outerbridge grade 0 or I lesions had significantly better patient-reported outcomes than those with Outerbridge grade II to IV lesions.
The negative effect of high-grade chondral defects that we found in our study on patient-reported outcomes is similar to the results of large database studies. In a registry study including 8476 patients, Rotterud et al 13 reported that patients with full-thickness cartilage lesions at the time of ACL reconstruction demonstrated significantly worse KOOS values across all subscales. However, a long-term follow-up of a cohort in the Norwegian registry 5 to 9 years after ACL reconstruction showed no significant differences in KOOS values between patients with concomitant full-thickness cartilage lesions and patients without concomitant cartilage lesions. 15
Limitations
While this study does demonstrate significant findings, it is not without limitations. This is a retrospective study, and it exhibits the inherent limitations of this type of research. Further, the current study only reports patients’ subjective outcomes, and limited objective outcomes are reported; we recognize that this limits the reliability of the findings. The follow-up length was short and may underestimate the true negative effect of meniscal lesions, similar to what has been reported in registry studies. 10 This is a diverse cohort, and differences between age, graft choice, and management of concomitant injuries could confound our results. The time interval from injury to surgery is also an important factor that should be evaluated in future studies. In a recent systematic review and meta-regression by Cinque et al, 6 the authors reported an increased risk of the development of posttraumatic osteoarthritis with an increasing time interval from injury to surgery. However, it is not clear if the effect of the time from injury to surgery can be detected with short-term follow-up studies. Specific articular cartilage defect locations could be analyzed rather than chondromalacia in general for most large series. Furthermore, meniscal injuries were evaluated in larger cohorts, limiting the specific reporting of outcomes based on the tear pattern or location. Finally, in spite of our relatively large cohort, some differences could still be missed, leading to type II errors. Despite multicenter studies having reported on the outcomes of associated cartilage and meniscus injuries at the time of ACL reconstruction, 4,9,11 the specific characteristics of these lesions have not been analyzed in detail. The strength of the present study is that a single surgeon’s results minimize the variability of using multiple surgical centers, which might have different operative techniques and rehabilitation protocols.
Conclusion
Patients with ACL tears achieved improved functional scores at a mean 3.2 years after ACL reconstruction. While meniscal lesions did not affect postoperative outcomes in the short term, chondral lesions were identified as a predictor for worse outcomes.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. receives royalties from Arthrex, Ossur, and Smith & Nephew; is a paid consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Linvatec, Ossur, and Smith & Nephew.
Ethical approval for this study was approved by the Vail Valley Medical Center Institutional Review Board (protocol No. 2002-03).