
Abstract
Background:
Intra-articular injuries to the hip in elite athletes represent a source of significant pain and disability. Hip arthroscopic surgery has become the gold standard for the treatment of disorders involving the hip joint.
Purpose:
To examine the incidence of and abnormalities treated with hip arthroscopic surgery as well as the impact on future participation in American football athletes invited to the National Football League (NFL) Scouting Combine with a history of hip arthroscopic surgery.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Athletes invited to the NFL Combine from 2012 to 2015 were evaluated for a history of hip arthroscopic surgery. Athlete demographics, imaging findings, and physical examination results were gathered using the NFL Combine database. Information on prospective participation in the NFL with regard to draft status, games played, games started, and current status was gathered using publicly available databases and compared against all other athletes participating in the combine.
Results:
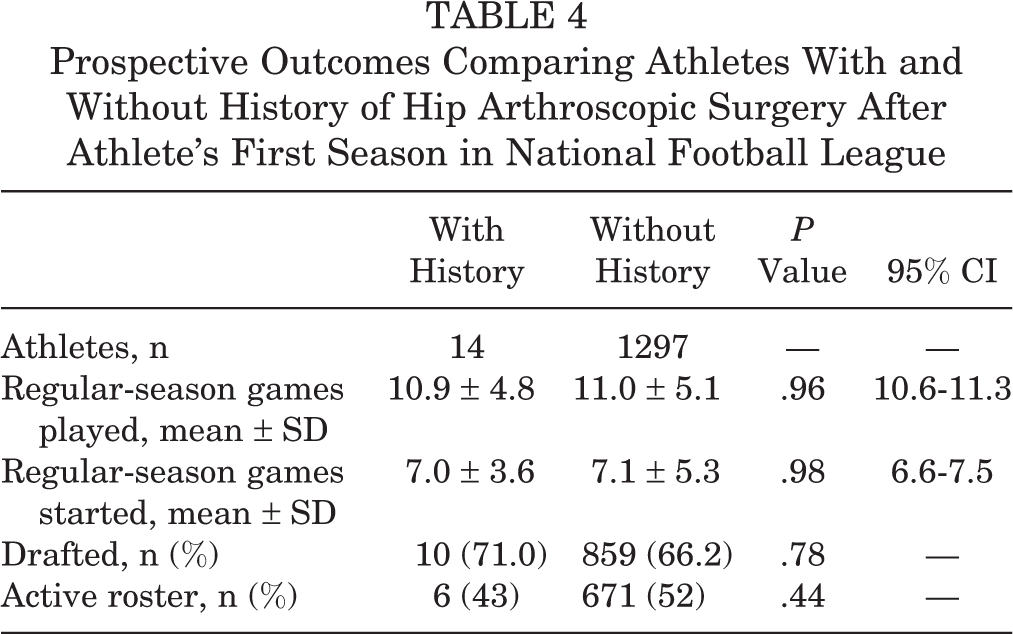
Fourteen athletes (15 hips) had a history of arthroscopic hip surgery. Acetabular labral tears were treated in 93% (14 hips), with femoroacetabular impingement decompression performed in 33% (5 hips). Compared with athletes who had no history of hip arthroscopic surgery, those undergoing arthroscopic surgery did not possess a lower likelihood of being drafted (66% vs 71%, respectively; P = .78) or of being on an active roster (52% vs 43%, respectively; P = .44) after their first season in the NFL. Moreover, there was no significant difference in the number of regular-season games played (10.9 ± 4.8 with arthroscopic surgery vs 11.0 ± 5.1 without; P = .96) or started (7.0 ± 3.6 with arthroscopic surgery vs 7.1 ± 5.3 without; P = .98).
Conclusion:
American football athletes invited to the NFL Combine with a history of hip arthroscopic surgery were not at risk for diminished participation when compared with all other athletes during their first season in the NFL.
High physiological stress and torsional force placed across the hip during competition in high-level American football athletes place the hip at a high risk of injuries. 6 Extra-articular injuries ranging from muscle strains and contusions to avulsion injuries around the hip are traditionally self-limiting and treated with rest and symptomatic care. Despite constituting only 5% of all injuries to the hip, intra-articular lesions represent a significant source of pain and time lost from play. 2,7 When persistent and limiting, intra-articular hip injuries involving the labrum or chondral surface in American football players often require surgical intervention to successfully return athletes to their prior level of competition in a timely manner. 8,19
Before advancements in diagnostic capabilities, intra-articular injuries to the hip were often misdiagnosed or went unrecognized secondary to low suspicion and negligible recognition in the literature. 15,29 However, improvements in imaging using high–spatial resolution magnetic resonance imaging (MRI), coupled with advancements in surgical techniques and instrumentation in the field of hip arthroscopic surgery, have enabled a more accurate and timely diagnosis with effective surgical management. 8,19
The use of hip arthroscopic surgery in the treatment of disorders involving and surrounding the hip has become the gold standard of treatment in athletes. This minimally invasive approach not only allows for the full visualization and treatment of common hip injuries but has also been shown to result in decreased recovery times with a quicker return to previous levels of competition for the treatment of labral tears, loose bodies, femoroacetabular impingement (FAI), capsular laxity, and snapping hip syndrome. 3,14,24,27 –29,31 However, the prevalence of and impact on prospective participation in elite American football athletes undergoing hip arthroscopic surgery are largely unknown.
The purpose of this study was to evaluate the prevalence of underlying intra-articular hip abnormalities necessitating treatment with hip arthroscopic surgery as well as their impact on future participation in elite American football athletes invited to the National Football League (NFL) Scouting Combine. We hypothesized that athletes with labral tearing and FAI would constitute the majority of athletes undergoing hip arthroscopic surgery, with no significant impact on future NFL participation when compared with all other athletes.
Methods
The study protocol was preapproved by an institutional review board and the NFL Health and Safety Committee. A retrospective review of all athletes invited to the NFL Scouting Combine from 2012 to 2015 was performed using the NFL Combine database. At the combine, comprehensive medical evaluations were performed by NFL team physicians on each athlete, with particular focus on past injuries requiring surgery. Imaging studies, including plain radiography, MRI, and computed tomography (CT), were routinely performed to evaluate all previous injuries to ensure a thorough assessment.
The combine profiles and results from all 1311 athletes invited to the NFL Combine from 2012 to 2015 were reviewed. Information collected from our database search consisted of athlete name, combine year, position, age, race, surgical history, and physical examination results. Information regarding prospective participation in the NFL with regard to draft status, games played, games started, and whether the athletes were on an active NFL roster at the conclusion of their first season was gathered using the internet database at www.NFL.com. Athletes identified as having undergone hip arthroscopic surgery in high school or college were included in the study for further analysis. Athletes were excluded if they had no history of hip arthroscopic surgery.
Evaluations of athlete-reported history and physician dictation reports were used to determine the specific hip abnormality (ie, labral tearing, FAI, removal of loose bodies, chondral defect) addressed during hip arthroscopic surgery. For the evaluation of functional deficits, physician dictation reports from the combine were examined and findings considered positive with any loss in range of motion (flexion, abduction, adduction, internal rotation, external rotation) as measured using a goniometer or strength testing (flexion, abduction, adduction) on the operative hip. Subjective symptoms were defined as any athlete-reported limitation (eg, soreness, pain) involving the operative hip on range-of-motion or strength testing.
The 2 senior authors (J.E.V., M.J.S.) independently reviewed all radiographs and MRI scans performed at the combine in athletes with a history of hip arthroscopic surgery. Radiographic imaging was used to evaluate for the presence of FAI (cam, pincer lesions), osteitis pubis, hip dysplasia, slipped capital femoral epiphysis, and osteoarthritis within the femoroacetabular joint. The extent of arthritic changes in the hip were independently graded as stage I (normal), II (minimal joint space narrowing), III (moderate joint space narrowing), or IV (severe loss of joint space with osteophyte formation) by the senior authors using the classification system described by Weinstein et al. 32 MRI of the postoperative hip was performed to evaluate for FAI (cam, pincer lesions), status of the labrum (intact vs torn), hip dysplasia, and the presence of any other concomitant injuries or abnormalities about the hip such as chondral loss or athletic pubalgia (AP). A cam lesion was defined as an alpha angle measurement greater than 55° on T1-weighted MRI on oblique cuts through the axial plane. 20 The senior authors initially reviewed all imaging and recorded the presence of any abnormalities noted on radiographs or MRI as well as alpha angle measurements. If any discrepancies were present between the authors for the presence or absence of a particular abnormality, grade of arthritic changes, or difference in alpha angle measurements greater than 10°, an independent musculoskeletal radiologist was asked to review the imaging findings to settle any disagreement. No CT was performed in any athletes identified as having undergone hip arthroscopic surgery.
Statistical analysis was performed to analyze the impact of hip arthroscopic surgery on future NFL participation based on draft status, total number of games played, games started, and current status in the NFL after the athlete’s first season compared with all other athletes invited to the combine with no history of hip arthroscopic surgery. Continuous variables were compared using the Student t test and categorical variables compared using the chi-square test. The Fisher exact test was performed in cases in which a variable had an expected frequency of ≤5. A P value of <.05 was used to determine statistical significance. All analyses were performed using Stata software version 13.0 (StataCorp).
Results
Analysis of the NFL Combine database identified 14 athletes (n = 15 hips) invited to the NFL Combine from 2012 to 2015 with a history of hip arthroscopic surgery, accounting for 1.1% of the 1311 athletes participating in the combine (Table 1). Offensive linemen (n = 3) and defensive backs (n = 3) had the greatest number of hip arthroscopic procedures, while placekickers had the highest incidence among all position groups (2/45, 4.4%). One athlete underwent bilateral hip arthroscopic surgery at different times during his collegiate career, while no athlete required revision surgery. Acetabular labral tearing was treated with repair alone (11/15, 73%), debridement alone (1/15, 7%), or repair and debridement (2/15, 13%) in 93% (14/15) of hips undergoing arthroscopic surgery, with concomitant FAI addressed with decompression in 33% (5/15) of hips (Table 2). One athlete (1 hip) underwent hip arthroscopic surgery with microfracture because of persistent pain from chondral damage in the hip. Functional limitations were present in 27% (4/15) of hips: specifically, decreased internal rotation (n = 3; mean, 6.6° ± 2.9°) and hip flexion (n = 1; mean, 30.0°) when compared with the nonoperative hip. No athlete demonstrated any decreased strength on examination.
Overview of National Football League Combine Participants (2012-2015) Based on Position

Overview of Athletes With History of Hip Arthroscopic Surgery for Intra-articular Hip Injury a
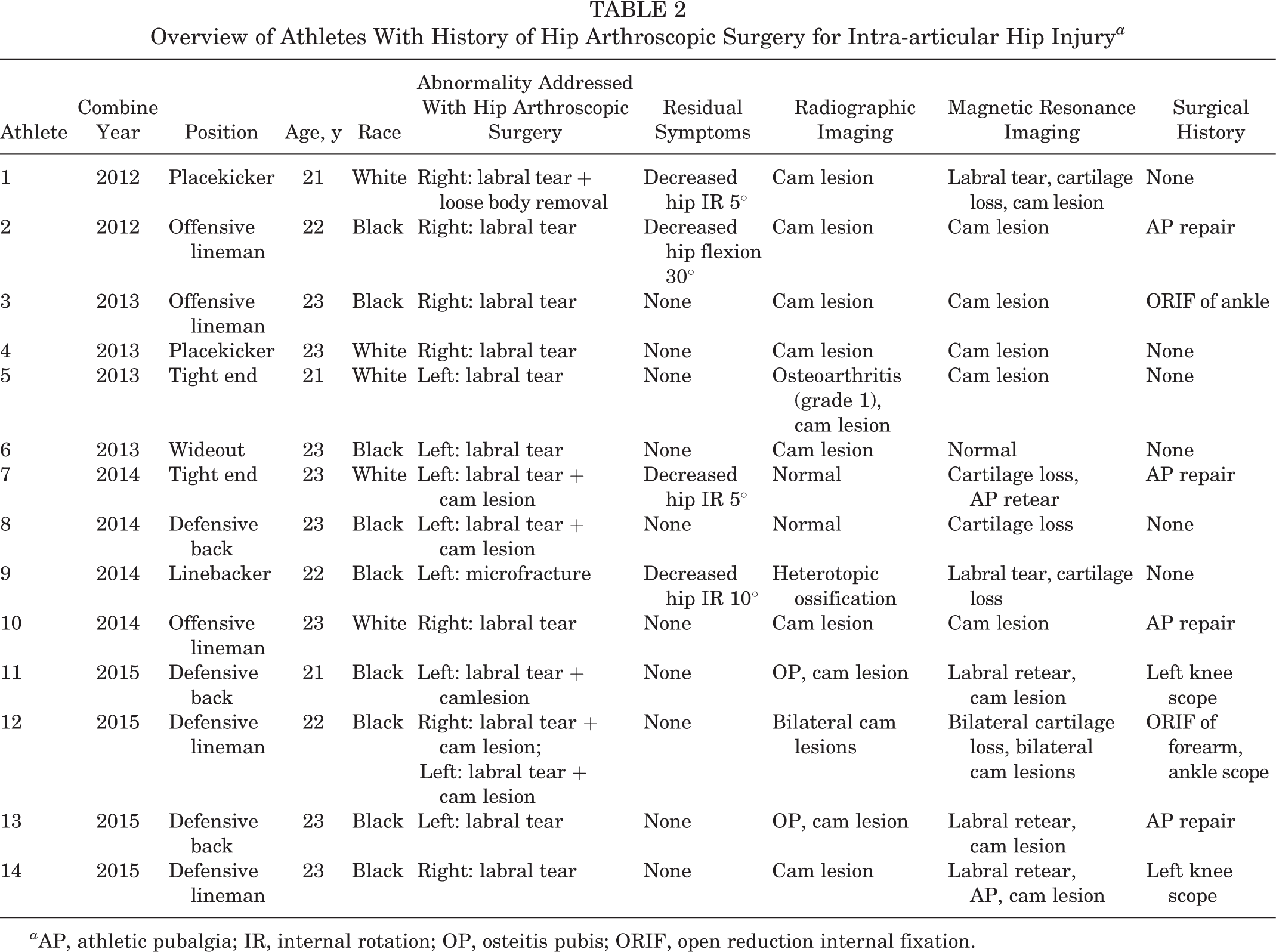
a AP, athletic pubalgia; IR, internal rotation; OP, osteitis pubis; ORIF, open reduction internal fixation.
A review of radiological imaging at the combine found consensual agreement between the senior authors for the presence of osteitis pubis in 13% (2 hips in 2 athletes) of hips, while osteoarthritis was identified in 6.7% (1 hip in 1 athlete) of hips, graded as stage I by both authors (Table 2). The athlete undergoing microfracture (athlete No. 9) was noted to have a significant amount of heterotopic ossification lateral to the acetabulum and femoral head. No athlete was noted to have evidence of hip dysplasia or slipped capital femoral epiphysis.
Cam lesions were identified on MRI in 73% (11/15; mean alpha angle, 64.6° ± 3.9°) of hips, including a persistent cam deformity in 60% (3/5; mean alpha angle, 68.2° ± 2.6°) of hips that underwent previous FAI decompression (Table 2). No athlete was found to have evidence of a pincer lesion. Alpha angle measurements performed by the senior authors were within 10° in all hips, precluding the need for consultation with an independent musculoskeletal radiologist, with no measurement discrepancies outside the diagnostic range for cam lesions. All athletes with cam lesions on MRI were similarly diagnosed on radiography, while 1 athlete (athlete No. 6) with a suspected cam lesion on radiography was found not to possess the necessary alpha angle on MRI by either senior author. Recurrent labral tearing was identified on MRI in 29% (4/14) of hips that had undergone prior labral repair or debridement. Recurrent labral tearing was present in 36% (4/11) of hips with untreated FAI lesions, defined by a residual alpha angle measuring greater than 55°. Evidence of cartilage loss on MRI was found in 40% (6 hips in 7 athletes) of operative hips. MRI evidence of AP was identified in 14% (2/14) of athletes, including 1 athlete (athlete No. 7) with evidence of recurrent tearing of the adductor/gracilis aponeurosis despite prior AP repair, while another (athlete No. 14) had newly discovered evidence of AP without physical examination findings. No athlete reported any concomitant surgery performed at the time of hip arthroscopic surgery. The most commonly reported additional surgical procedure performed at a separate time in athletes with a history of hip arthroscopic surgery was AP repair, present in 29% (4/14) of athletes.
Prospectively, 71% (n = 10) of athletes were successfully drafted into the NFL, including all athletes treated for combined labral tearing and FAI (Table 3). A total of 57% (8/14) of athletes played in a regular-season game, while 21% (3/14) started a regular-season game. After the conclusion of each athlete’s first season in the NFL, 43% (6/14) were on an active NFL roster, while 21% (3/14) of athletes were on injured reserve for injuries not involving the operative hip. Statistical analysis found that when compared with all other athletes invited to the combine, athletes with a history of hip arthroscopic surgery were not at a significantly different risk of being undrafted (P = .78), of playing (P = .96) or starting (P = .98) in fewer NFL games during their first season in the NFL, or of being on an active NFL roster (P = .44) (Table 4).
Prospective Participation of Athletes With History of Hip Arthroscopic Surgery

a After the conclusion of the athlete’s first season in the National Football League.
Prospective Outcomes Comparing Athletes With and Without History of Hip Arthroscopic Surgery After Athlete’s First Season in National Football League
Discussion
Intra-articular lesions to the hip represent a small proportion of injuries sustained in elite American football athletes in comparison with injuries to the shoulders, knees, and extremities. 1,8 Our study corroborates the findings from Byrd and Jones, 5 who reported labral tearing present in 61% of athletes in their study, as the most common hip abnormality appreciated during hip arthroscopic surgery; the current study found labral lesions in 93% (14/15) of hips undergoing arthroscopic surgery. However, it has only been over the past 2 decades that labral tearing has become widely recognized as a potential source of hip pain in elite athletes. 4,8,14 Using the NFL Injury Surveillance System, Feeley et al 8 examined the incidence and cause of hip injuries from 1997 to 2006, identifying only 5 cases of labral tearing of 738 (0.7%) recorded injuries to the hip, with none reported before 2004. The same authors then contrasted these findings with their more recent institutional experience, in which the senior authors reported treating a total of 13 professional football athletes with labral tears over a 7-year period from 2001 to 2008. 8 Feeley et al noted that within their practice, athletes typically demonstrated decreased internal rotation and pain with internal rotation and flexion of the hip, prompting advanced imaging for a diagnosis secondary to suspicion for potential labral abnormalities. While the recognition of labral injuries has improved, a careful physical examination with pain or limitations about the hip in contact athletes should raise the suspicion for underlying labral abnormalities, prompting additional imaging for diagnostic confirmation.
Multiple studies have demonstrated a strong association between labral abnormalities and the presence of impingement secondary to FAI within the hip. 11,16,21,24,33 In this study, FAI lesions were identified in 73% of hips with a history of hip arthroscopic surgery. Similarly, in their cohort of 13 professional football players treated with hip arthroscopic surgery, Feeley et al 8 reported that 100% of athletes with labral tears also possessed alpha angles (mean, 63.2°) suggestive of impingement. All athletes undergoing hip arthroscopic surgery in their study (n = 5) were subsequently treated with labral debridement and decompression of FAI lesions. In addition, Philippon et al 25 reported that in the treatment of 5 professional football players with hip arthroscopic surgery, all were found to have labral tearing with impingement.
Moreover, this study found that 73% of hips evaluated at the combine with a history of hip arthroscopic surgery had continued evidence of impingement radiographically based on alpha angle measurements greater than 55° after surgery, including 60% of hips initially treated with decompression for FAI. Multiple studies have found that the failure to address impingement lesions results in inferior outcomes after arthroscopic surgery. 10,26,27 Heyworth et al 10 found that in 24 hips requiring revision surgery, 79% (n = 19) possessed untreated, underlying impingement. In addition, the authors found that of the 8 hips with recurrent labral tearing despite prior repair, untreated FAI lesions were identified in 75% (6/8 hips) and concluded that unaddressed FAI is effectively a contraindication to labral repair or reattachment when performed as an isolated procedure. The results from the current investigation support the high rate of recurrent labral tearing in athletes with persistent FAI, as recurrent tearing was present in 36% (4/11) of hips previously treated with isolated labral repair or debridement versus 0% (0/2) of hips with a history of FAI decompression with an alpha angle measurement of less than 55°. However, the clinical and physical implications for labral tearing or persistent FAI appreciated on imaging appear to be nonsignificant, as the incidence of functional limitations or subjective symptoms in the athletes evaluated in this study was small. Moreover, prior investigations have found that despite a high prevalence of radiographic hip abnormalities, many elite athletes remain asymptomatic. In their assessment of 95 asymptomatic elite male soccer athletes, Gerhardt et al 9 reported the presence of cam lesions in 54% (51/95) of athletes, while Silvis et al 30 found a 56% (22/39) prevalence of labral tearing in asymptomatic collegiate and professional hockey athletes and evidence of cam lesions in 31% (12/39).
The high axial and torsional loads placed on the hip joint in American football players often lead to the development of injuries outside of the hip joint. 8,10 AP repair was the most commonly reported additional surgical procedure performed in athletes with a history of hip arthroscopic surgery, with 29% of athletes reporting AP repair before or after hip arthroscopic surgery. The association between intra-articular hip abnormalities and AP has been well documented, leading to the moniker “sports triad” to represent the combination of labral tearing with adductor and rectus strains present in athletes. 13,18,19 Many authors have theorized that hip injuries create muscle imbalances across the hip, alterations that lead to additional abnormalities and injury progression. 17 However, no definitive timeline of an injury has been established as to whether labral injuries are caused by or are the effects of rectus and adductor strains, both of which share a common sheath. 8 Based on its strong association with intra-articular hip abnormalities, elite-level contact athletes require an evaluation for all potential sources of hip pain, including extra-articular lesions implicated in AP.
This study is not without limitations. The collection of data was retrospective in nature and dependent on the athlete’s recollection at a single point in time during the NFL Scouting Combine, inviting the potential for recall bias. As such, specific details regarding injury mechanisms, dates of injury, surgical indications, failed nonoperative measures, and timing from injury to surgery were infrequently reported and thus not included in the analysis. We did not have access to operative reports to determine the full extent of injuries addressed during hip arthroscopic surgery, relying purely on athlete reports and postoperative imaging. Because of the small number of athletes meeting appropriate inclusion/exclusion criteria, we were unable to perform any meaningful statistical analysis to determine the impact of recurrent acetabular labral tearing, untreated FAI lesions, or the presence and grade of femoroacetabular osteoarthritis on future participation in the NFL. Selection bias was present in this study, as only athletes who received an invitation to the NFL Combine were analyzed, and therefore, this study does not account for athletes participating in the NFL with a history of hip arthroscopic surgery who were not invited to the combine. As it is possible that athletes may have failed to receive an invitation to the combine secondary to persistent symptoms after hip arthroscopic surgery, we are unable to determine if hip arthroscopic surgery represents a true hindrance to short-term participation in all athletes in the NFL. In addition, the status of an athlete in the NFL (active, free agent, injured reserve, practice squad) is multifactorial and may be related to factors beyond a specific injury history. Last, no athlete underwent magnetic resonance arthrography, which has been shown to provide increased detection for the diagnosis of labral and chondral abnormalities within the hip joint. 12,22,23
Conclusion
In elite American football athletes participating in the NFL Scouting Combine from 2012 to 2015, 1.1% of athletes had a history of hip arthroscopic surgery for the treatment of intra-articular hip abnormalities, primarily labral tearing with or without concomitant FAI. The majority of athletes were found to have evidence of untreated FAI lesions. American football athletes invited to the NFL Combine with a history of hip arthroscopic surgery were not at risk for diminished participation when compared with all other athletes during their first season in the NFL.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. is a paid consultant for Ossur and Stryker and receives research support from AlloSource, Arthrex, Athletico, DJ Orthopaedics, Linvatec, MioMed, Smith & Nephew, and Stryker. J.E.V. is a paid consultant for Arthrex. M.J.S. is a paid consultant for Smith & Nephew.
Ethical approval for this study was obtained from the Institutional Review Board for Human Investigation of the University Hospitals Cleveland Medical Center (No. 04-15-50) and the National Football League Health and Safety Committee.