
Abstract
Background:
Although restricted hip range of motion (ROM) is associated with an increased risk for injuries in baseball players, the evolution of hip ROM over the season remains undefined.
Hypothesis:
Hip ROM profiles would be symmetric between hips and positions (pitchers vs position players) but would decrease from preseason to postseason. Additionally, it was hypothesized that this decrease in motion would correlate with workload.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Bilateral hip ROM was assessed in 96 professional baseball players (54 pitchers, 42 position players) preseason and postseason. ROM comparisons were made between lead and trailing hips, pitchers and position players, and preseason and postseason measures. The change from preseason to postseason was correlated with player demographics and measures of workload for pitchers and position players.
Results:
Preseason hip ROM was symmetric between hips; however, pitchers demonstrated increased preseason lead hip internal rotation (IR) (P = .018) and bilateral hip total ROM (TROM) (P < .020) compared with position players. From preseason to postseason, position players lost 7° of external rotation (ER) (P ≤ .005 ). In pitchers, the loss of IR correlated with increased pitches (P = .016) and innings (P = .037), while the loss of ER (P = .005 ) and TROM (P = .014) correlated with increasing mean fastball velocity. Workload for position players did not correlate with motion loss.
Conclusion:
Symmetric hip ROM profiles should be anticipated in baseball players; however, pitchers may have increased preseason IR and TROM and postseason ER and TROM relative to position players. Although loss of motion correlated with workload in pitchers, this was not the case for position players. Hip motion should be monitored over the course of the season. This is particularly true for pitchers who lose IR as workload increases, which may place them at a greater risk for injuries.
A multitude of studies have demonstrated rising rates of injuries in professional baseball players in recent years. 5,6,8,21 Because nearly half of these injuries occur to the shoulder and elbow, increased attention is being paid to risk factors for upper extremity injuries, such as deficits in shoulder motion, humeral torsion, elbow motion, workload, pitch velocity, and throwing mechanics, just to name a few. 1,2,9,13,20,26,28 –30 In recent years, the concept of the “kinetic chain” has gained popularity, and increasing evidence is now demonstrating that flaws in any component of this chain can adversely affect performance and potentially increase the risk for injuries in subsequent segments. 10 –12,14,15,27 This critical concept supports a more holistic approach to identifying mechanical or kinematic deficiencies in the lower extremities, hips, core, and upper body rather than focusing on the shoulder and elbow in isolation. Accordingly, a number of studies have now been published on the role of the hips in professional baseball. While several of these have simply reported on hip strength, kinematics, and rotational profiles of pitchers, 3,7,17,19,24 others have attempted to correlate these parameters with the development of subsequent injuries. 16,23,25
Currently, studies on hip range of motion (ROM) in baseball players have yielded conflicting results. Some authors have suggested that hip ROM profiles vary between the lead (contralateral to the side of throwing dominance) and trailing (ipsilateral to the side of throwing dominance) hips for a given player 17,19 or across different positions (ie, pitcher vs position player), 16 while others indicate that symmetric rotational profiles should be anticipated between hips and across positions. 7,24 Regarding injuries, Li et al 16 identified higher rates of hip, groin, and hamstring injuries in players with decreased hip internal rotation (IR). Similarly, Saito et al 23 found that decreased hip flexion and IR were risk factors for elbow pain, while Scher et al 25 correlated altered hip ROM with shoulder injuries in professional pitchers. As our understanding of this important topic grows, it is becoming clear that the hips are a key component to performance and injury risk in nearly every baseball-related movement, and the pitching motion is no exception (Figure 1).
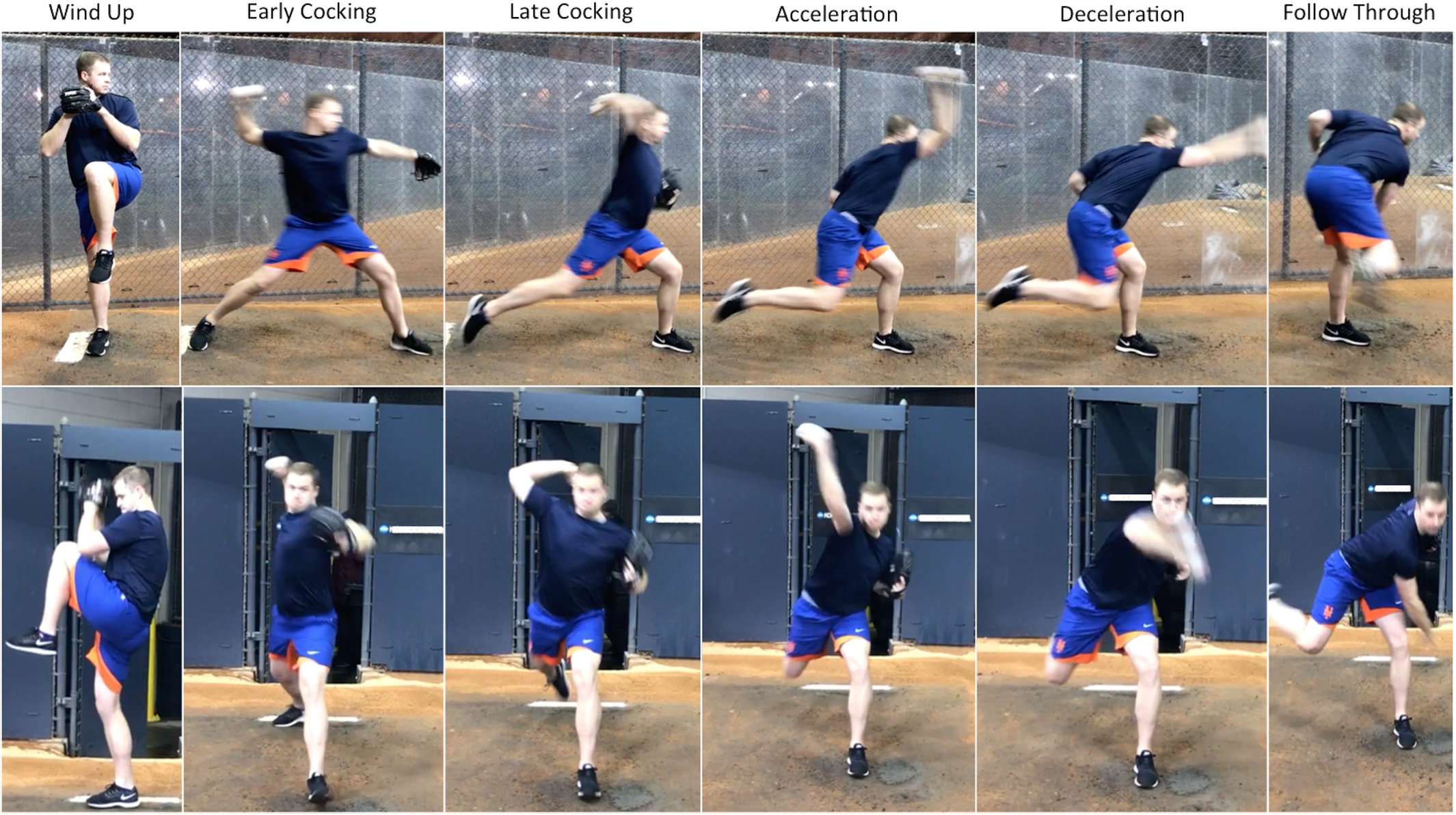
The 6 main phases of the throwing motion (windup, early cocking, late cocking, acceleration, deceleration, and follow-through) are demonstrated from the side (top) and front (bottom). To progress through these phases, the lead (contralateral to the side of throwing dominance) and trailing (ipsilateral to the side of throwing dominance) hips experience differing degrees of flexion, extension, abduction, adduction, internal rotation, and external rotation.
In another study on hip ROM and strength in 14 collegiate baseball pitchers, mean hip motion decreased from preseason to postseason. 31 Specifically, the mean external rotation (ER) decreased 8° in the lead hip and 10° in the trailing hip, while IR remained fairly steady. These changes did not correlate with the number of pitches thrown for the season. Because decreased hip motion has been associated with an increased risk for injuries, these findings are particularly concerning, as players may be at an increased risk as the season progresses and hip motion decreases. Although this work has contributed significantly to our understanding of the evolution of hip motion during a baseball season, it is not without limitations. These include a small sample size of 14 pitchers, the potential lack of sufficient power to accurately determine the relationship between workload and loss of motion, and the exclusion of position players. Similarly, because the study was performed at the collegiate level, in which the typical season lasts approximately 3 months (approximately 60 games), it may not fully translate to professional baseball, in which the season generally lasts 6 months (162 games). It is possible that with this increased workload in professional baseball, the changes in hip motion could be even more pronounced. Accordingly, the purposes of the current study were to (1) quantify the changes in hip motion in both professional pitchers and position players over the course of the Major League Baseball (MLB) season and (2) determine if specific player demographics (age, body mass index [BMI], etc) or measures of workload (innings pitched, number of pitches, and mean velocity for pitchers; games, at-bats, plate appearances, and innings for position players) were correlated with changes in hip ROM.
Methods
This study was approved by the institutional review board of the Hospital for Special Surgery. Over the course of 4 seasons, a comprehensive physical examination was performed on all players (both pitchers and position players) invited to the spring training session of a single MLB organization. Among other things, this examination consisted of an assessment of bilateral hip ROM including IR and ER. ROM was again assessed at the end of the season. Only players who were playing without restriction, free from hip injuries at the time of examination, and available for both preseason and postseason measurements were included in the study. Players were excluded if they did not have a complete assessment of hip ROM or if they were suffering from a hip injury when ROM was assessed. Player demographics recorded at the time of the examination included handedness, age, height, weight, and BMI. If a player presented to spring training for multiple seasons, ROM was measured for each season. Accordingly, data were analyzed as “player-seasons,” in which the evolution of motion was considered separately for each year.
Assessing Hip ROM
Hip ROM was assessed using a reliable and previously validated technique in which the player is positioned supine and the hip and knee are flexed to 90°. 4,18,22 This technique for measuring hip motion has demonstrated excellent interrater reliability (intraclass correlation coefficient range, 0.88-0.95 for IR and 0.91-0.95 for ER), low coefficients of variance (range, 7.7%-10.0% for IR and 5.2%-8.0% for ER), and standard errors of measurement (2.4° for IR and 2.5° for ER) that allow the accurate assessment of hip IR and ER with maximal mean discrepancies ranging from 2° to 3° between different examiners. 18,22 To further improve on this interrater reliability and accuracy, the same examiner completed all goniometric measurements in this study. This was accomplished as a second practitioner (J.M.Z.) held the extremity in position while the first practitioner (D.P.) measured IR and ER using a standardized Jamar goniometer centered over the long axis of the femur. The stationary limb of the goniometer paralleled the long axis of the patient, while the mobile arm paralleled the anterior crest of the tibia. The hip joint was taken to the maximal amount of IR or ER permissible without altering the normal arthrokinematics of the joint. Total ROM (TROM) for each hip was calculated by adding IR and ER. All measurements were video recorded and reviewed by multiple study personnel to ensure consistency and reliability in the technique. The same 2 examiners had the same roles and performed all measurements on all patients across all seasons.
Defining Lead Versus Trailing Hip
The determination of lead and trailing hips was based on throwing hand dominance for both pitchers and position players. The designation of the lead hip was assigned to the hip contralateral to the side of throwing dominance, as this hip leads the throwing motion. The hip ipsilateral to the side of throwing dominance was labeled the trailing hip. For position players, hip designation was based on throwing dominance rather than batting dominance, as a number of position players were switch hitters and did not have a consistent lead hip when batting.
Measures of Workload
For all pitchers, 3 different measures of workload were calculated. These included total pitches thrown over the course of the season, number of innings thrown, and mean fastball velocity in miles per hour (mph). Only pitches thrown in official games were used in these measurements. This did not include throwing activity that occurred during spring training, in the bullpen, during practice sessions, or as part of a normal warm-up in preparation for live game throwing. For position players, measures of workload included games played, at-bats, plate appearances, and innings played. As with the pitchers, only live game activity was recorded.
Statistical Analysis
Because of the differing demands placed on the players, separate analyses were performed for pitchers and position players. Where appropriate, results are reported using descriptive statistics such as number, mean ± SD, range, and median. Pairwise comparisons between normally distributed continuous variables (ie, mean preseason vs postseason ROM) were performed using a Student t test. These results are reported with mean differences (MDs), 95% CIs, and their corresponding P values. To assess the relationship of workload and hip motion, Pearson correlation coefficients were calculated for each relationship. These results are reported with their corresponding R and P values. For all comparisons, only P values <.05 were considered to represent statistical significance.
Results
Overall Demographics
A total of 54 pitchers and 42 position players met all inclusion criteria and underwent comprehensive assessments of hip ROM before and at the end of the MLB season. One position player was excluded because of a hip injury at the time of the end of the season examination. For pitchers, mean demographic data were as follows: age, 27.9 ± 4.7 years; height, 188.4 ± 5.0 cm; weight, 97.4 ± 11.1 kg; and BMI, 27.5 ± 3.5 kg/m2. For position players, mean values were the following: age, 27.3 ± 3.6 years; height, 186.3 ± 4.6 cm; weight, 96.3 ± 7.7 kg; and BMI, 27.7 ± 1.9 kg/m2. Additional demographic data are provided in Table 1. Pitchers threw a mean of 1244 ± 910 pitches and 102.7 ± 52.3 innings over the course of the season. The mean fastball velocity was 92.4 ± 2.6 mph (range, 87.5-97.9 mph). Position players had a mean of 115.5 games played, 373.0 at-bats, 418.9 plate appearances, and 805.0 innings played (Table 1).
Basic Demographics and Measures of Workload for All Pitchers and Position Players a
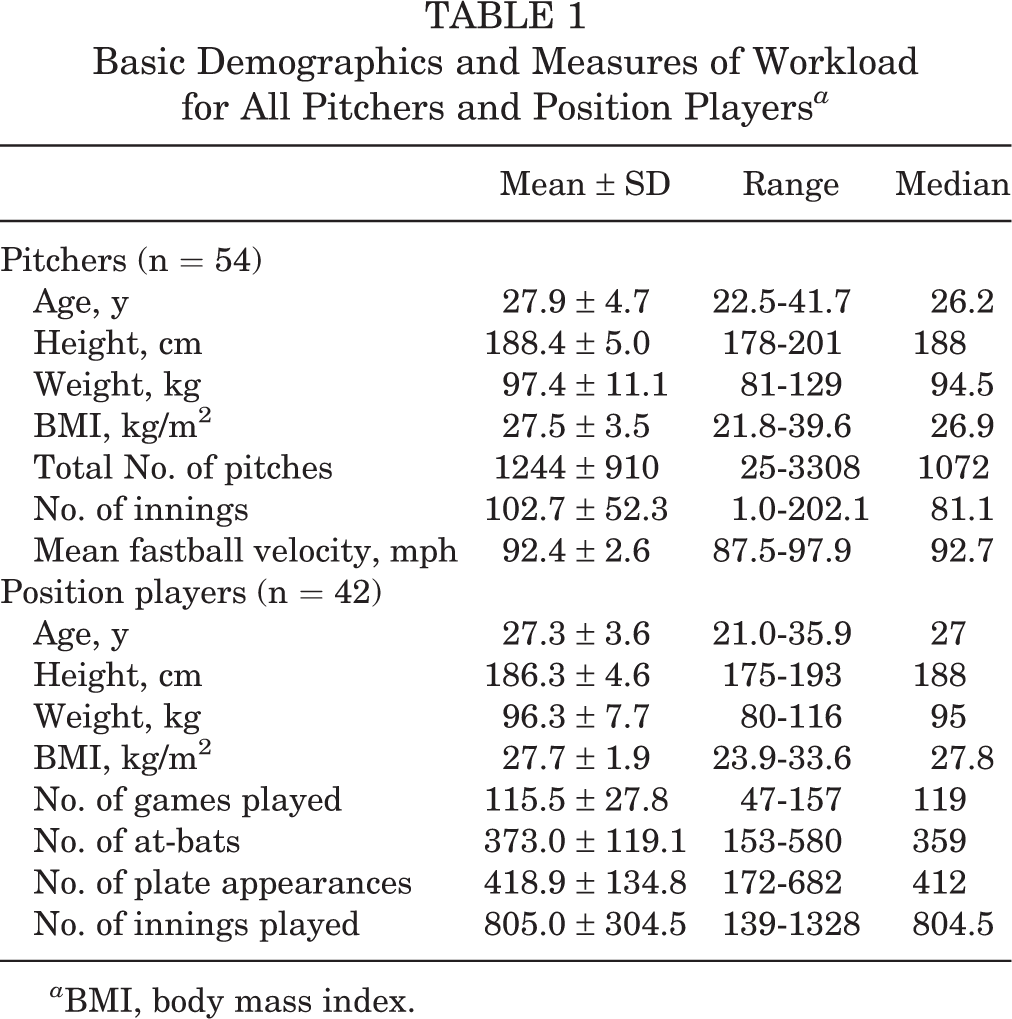
a BMI, body mass index.
Symmetry of Hip Motion
Comparisons of lead and trailing hip motion between the preseason and postseason measurements are listed in Table 2. Overall, preseason hip motion was symmetric for pitchers between their lead and trailing hips for IR (39.1° vs 37.1°, respectively; P = .269), ER (46.9° vs 48.7°, respectively; P = .345), and TROM (85.9° vs 85.8°, respectively; P = .958). Similar results were observed for the preseason lead and trailing hips of position players for IR (34.1° vs 34.0°, respectively; P = .967), ER (45.9° vs 46.9°, respectively; P = .676), and TROM (80.0° vs 80.7°, respectively; P = .746).
Changes in Hip Range of Motion Over the Course of the Season for Professional Baseball Players a

a All values are expressed in degrees except for P values. P values <.05 are presented in bold. ER, external rotation; IR, internal rotation; MD, mean difference; TROM, total range of motion.
b Negative values indicate a loss of motion.
Comparison of Pitchers and Position Players
Overall, pitchers tended to have more IR and TROM compared with position players (Table 2). More specifically, during the preseason examination, pitchers demonstrated more IR in the lead hip (39.1° vs 34.1°, respectively; MD, 5.0°; 95% CI, 0.89°-9.11°; P = .018), TROM in the lead hip (85.9° vs 80.0°, respectively; MD, 5.9°; 95% CI, 1.94°-9.86°; P = .004), and TROM in the trailing hip (85.8° vs 80.7°, respectively; MD, 5.1°; 95% CI, 1.07°-9.13°; P = .014). None of the other preseason hip ROM measures were significantly different (P > .05 for all). For the postseason examination, greater differences were noted for ER and TROM between pitchers and position players. Pitchers demonstrated higher postseason lead hip ER (43.1° vs 38.5°, respectively; MD, 4.6°; 95% CI, –0.26° to 9.46°; P = .063), trailing hip ER (46.0° vs 40.3°, respectively; MD, 5.7°; 95% CI, 1.12° to 10.39°; P = .018), lead hip TROM (79.9° vs 74.0°, respectively; MD, 5.9°; 95% CI, 0.51° to 11.23°; P = .034), and trailing hip TROM (82.8° vs 75.3°, respectively; MD, 7.5°; 95% CI, 2.25° to 12.75°; P = .006).
Change in Motion Over the Course of the Season
Looking at the change of ROM over the course of the season in pitchers, lead hip TROM decreased 6.0° from 85.9° to 79.9° (95% CI, –10.6° to –1.5°; P = .010), and there was a trend toward decreased lead hip ER from 46.9° to 43.1° (MD, –3.8°; 95% CI, –8.0° to 0.4°; P = .078) (Table 2). In position players, decreases from preseason to postseason were noted for lead hip ER (MD, –7.4°; 95% CI, –12.2° to –2.6°; P = .003), trailing hip ER (MD, –6.6°; 95% CI, –11.1° to –2.1°; P = .005), lead hip TROM (MD, –6.0°; 95% CI, –10.8° to –1.2°; P = .016), and trailing hip TROM (MD, –5.4°; 95% CI, –9.7° to –1.1°; P = .015) (Table 2).
Relationship of Hip Motion to Workload
For pitchers, there were no significant correlations between any of the demographic parameters studied (age, height, weight, and BMI) and the change in hip ROM. However, trailing hip IR decreased as total pitches (R = –0.330; P = .016) and number of innings (R = –0.288; P = .037) increased. As the mean fastball velocity increased, decreases were noted for trailing hip ER (R = –0.382; P = .005) and trailing hip TROM (R = –0.336; P = .014) (Table 3). None of the demographics or measures of workload significantly correlated with the change in hip ROM for position players.
Significant Correlations Between Loss of Hip Motion and Workload in Pitchers a

aP values <.05 are presented in bold. ER, external rotation; IR, internal rotation; TROM, total range of motion.
Discussion
The hip plays a critical role in nearly every baseball-related activity, and a number of recent studies have demonstrated an increased risk of hip, groin, hamstring, shoulder, or elbow injuries in pitchers with restricted hip ROM. 16,23,25 Although this relationship between hip ROM and injuries is gaining interest, our understanding of the evolution of hip ROM over the course of the baseball season remains limited. Accordingly, the purposes of this work were to characterize the change in hip ROM from preseason to postseason and to determine if these changes correlated with various measures of workload experienced during the season. Ultimately, there were no significant differences between preseason lead and trailing hip ROM measures in pitchers or position players; however, pitchers tended to have increased preseason IR and increased postseason ER compared with position players. Pitchers lost a mean of 6.0° of lead hip TROM over the course of the season, while position players demonstrated decreases in lead hip ER (7.4°), trailing hip ER (6.6°), lead hip TROM (6.0°), and trailing hip TROM (5.4°) over the season. For position players, none of the player demographics or measures of workload correlated with loss of motion.
Similar to previous work performed in collegiate 7 and professional 24 baseball players, the current study demonstrates relatively symmetric ROM profiles between the lead and trailing hips of these athletes. This is in contradiction to the works of McCulloch et al, 17 which found greater ER in the lead hip and Picha et al, 19 which found greater IR in the lead hip of pitchers compared with their trailing side. Although these last 2 studies conflict with one another and the current investigation, the majority of published works suggest that symmetrical hip ROM should be anticipated in professional baseball players.
When comparing pitchers with position players, Sauers et al 24 did not find any significant differences across positions; however, Li et al 16 reported decreased IR in pitchers and catchers compared with other position players. In the current study, pitchers had significantly increased IR and TROM compared with position players at the beginning of the season, but ER was similar between the groups. This relationship changed over the course of the season as position players tended to lose a significant amount of ER while maintaining (or slightly gaining) IR. Accordingly, on the postseason assessment, IR was similar between pitchers and position players; however, pitchers had greater amounts of ER and TROM compared with position players.
When specifically evaluating pitchers, they tended toward decreased ROM over the course of the season, with a 6.0° decrease in lead hip TROM representing the most significant change (P = .010). It is also worth noting that decreases in IR, ER, and TROM tended to be more pronounced in the lead hip (2.3°, 3.8°, and 6.0°, respectively) compared with the losses observed in the trailing hip (0.4°, 2.7°, and 3.0°, respectively). Although the differences were not statistically significant, there was a tendency toward greater losses in ER compared with IR for both hips in pitchers. This is in agreement with a recent report on hip ROM in collegiate baseball players in which ER and TROM decreased significantly (P < .01) over the course of a collegiate baseball season but IR was maintained. 31 In that study, changes in hip ROM were not correlated with measures of workload such as innings pitched, number of pitches thrown, and maximum velocity. 31 In the current study, trailing hip ROM was significantly correlated with total pitches (decreased IR), innings pitched (decreased IR), and mean fastball velocity (decreased ER and TROM). Although these correlations were statistically significant (P < .04 for all), the relationship was weak (R < −0.4 for all ).
For position players, the most significant observation was the loss of ER in both the lead (7.4°) and the trailing (6.6°) hips. This decline also resulted in a significant decrease in bilateral TROM over the season. Although several prior studies have linked decreased hip IR and/or flexion to injuries in baseball players, 16,23,25 it is unknown if decreased ER and TROM increase the risk of injuries in professional baseball players. Unlike pitchers, the changes in position players tended to be symmetric, and workload did not correlate with decreased ROM. The fact that ROM decreased significantly but did not correlate with any measure of workload in position players may be related to the fact that these measures are not adequate for quantifying the true amount of work experienced by the hips during the season. Ultimately, workload may prove to be more difficult to quantify in position players, as they use their hips for a wider array of baseball-specific activities (fielding, throwing, batting, running, etc) compared with pitchers, who predominantly throw.
There are a few limitations to this research that merit discussion. This study of 96 professional baseball players may not have been sufficiently powered to detect stronger relationships between workload and loss of hip motion. Also, as mentioned previously, the true workload of professional baseball players is a very difficult entity to measure. Although each of the measures used in this work may approximate the relative workload, none fully encompasses the work experienced by these athletes. Currently, there are no reliable methods with which to assess the actual workload (on and off the field) of baseball players, and it varies significantly across different players. Accordingly, additional research into this critical topic is warranted. This work is also limited by not correlating these changes with player-reported outcomes. The players were not asked if they noticed decreased motion or if they felt like it affected their performance in any way. It is also worth noting that interrater reliability was not assessed for the methods used to quantify hip ROM, and ROM was only assessed in the supine position (rather than in the prone and supine positions). Repeated measures were not performed because it was not logistically practical in the setting of preseason and postseason player examinations. A number of steps were taken to maximize the accuracy and reliability of the measures, including the utilization of previously validated measurement techniques, 4,22 2 examiners (one to position the limb and the other to take the measurement), the same 2 examiners for all measurements, and video recording of the examination to ensure proper maintenance of the technique.
Conclusion
Contrary to the stated hypothesis, pitchers tended to have greater IR and TROM than position players at the beginning of the season. Over the course of the season, position players lost significantly more motion (particularly ER and TROM) than pitchers, with pitchers demonstrating increased ER and TROM compared with position players at the season’s end. Although this loss of motion did not correlate with workload for position players, increased total pitches, number of innings pitched, and mean fastball velocity weakly correlated with greater losses of hip motion in pitchers. These data may prove beneficial as the link between injuries and restricted ROM is becoming more established in the current literature. Further study is needed to determine if this injury risk increases over the course of the season, as players lose more hip motion, and to more precisely define “workload” in professional baseball players over the course of a season.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S.R. receives research support from Arthrex, DePuy Synthes–Mitek, and Stryker; is a paid consultant for Arthrex, CeramTec, Medtronic, MioMed, and Stryker-Mako; is a paid presenter or speaker for Arthrex, CeramTec, Medtronic, and Stryker-Mako; has stock/stock options in ConforMIS; and receives royalties from DePuy Synthes–Mitek, Springer, and Stryker-Mako. J.S.D. is a paid consultant for Arthrex, ConMed Linvatec, and Trice; is a paid presenter or speaker for Arthrex; receives research support from Arthrex; and receives royalties from ConMed Linvatec and Wolters Kluwer Health–Lippincott Williams & Wilkins. S.H.C. receives royalties from Blue Belt Technologies, has stock/stock options in Blue Belt Technologies and CyMedica Orthopedics, and is a paid consultant for Stryker–Pivot Medical.
Ethical approval for this study was obtained from the Hospital for Special Surgery (study No. 2016-252).