
Abstract
Primary anterior cruciate ligament (ACL) reconstructions (ACLRs) are being performed with increasing frequency. While many of these will have successful outcomes, failures will occur in a subset of patients who will require revision ACLRs. As such, the number of revision procedures will continue to rise as well. While many reviews have focused on factors that commonly contribute to failure of primary ACLR, including graft choice, patient factors, early return to sport, and technical errors, this review focused on several factors that have received less attention in the literature. These include posterior tibial slope, varus malalignment, injury to the anterolateral ligament, and meniscal injury or deficiency. This review also appraised several emerging techniques that may be useful in the context of revision ACL surgery. While outcomes of revision ACLR are generally inferior to those of primary procedures, identifying these potentially underappreciated contributing factors preoperatively will allow the surgeon to address them at the time of revision, ideally improving patient outcomes and preventing recurrent ACL failure.
Keywords
The annual incidence of revision anterior cruciate ligament (ACL) reconstruction (ACLR) continues to rise. 5,44 It is estimated that 200,000 ACLRs are performed annually in the United States, 44 with reported revision rates ranging from 1% to 13%. 5,68,123 Reconstruction of the ACL is a reliable procedure, with 90% of patients reporting improvement in functional outcomes following surgery. 7,8,36 However, patient-reported outcomes following revision ACLR have produced less favorable results in the literature. 1,41,65,130,131 Furthermore, functional outcomes have been noted to decline further after multiple ACL revisions. 126,128 Following ACL revision, patients sustain lower rates of return to sport, 4,61 higher rates of chondral damage, 1,13,126 and higher rates of subsequent revision surgery. 131
Most reviews that address the factors that commonly contribute to failure of primary ACLR have focused on graft choice, patient factors, and technical errors, including tunnel placement, graft tension, and failure of graft fixation. 38,95,124,133 The purpose of this review was to highlight several underappreciated factors in the literature that must be considered when evaluating a patient in whom ALCR failed and to appraise novel surgical techniques that have recently been reported to manage these complex patients. Such factors include alignment (both sagittal and coronal), injury to the anterolateral capsule, emerging concepts involving the importance of the injured menisci, and contemporary considerations regarding anatomic features of the ligament and single-stage revision surgery.
Anterior Cruciate Ligament Reconstruction Failure
A consensus on what constitutes ACLR failure has yet to be reached, with failure being defined through a variety of objective and subjective measures. According to Johnson and Fu, 51 failure can be attributed to 1 or more of 4 main categories: recurrent pain or arthritis, arthrofibrosis or loss of motion, extensor mechanism dysfunction, or recurrent instability patholaxity. 47 Kamath et al 52 highlighted various causes for recurrent instability, which they classified as either early or late presentations. Early instability (<6 months) may be attributed to technical error, failure of graft incorporation, premature return to high-demand activities, or overly aggressive rehabilitation. Late causes may include repeated trauma to the graft, poor graft placement, generalized ligamentous laxity, and concomitant abnormality not addressed at the time of the reconstruction. 52
While technical errors have frequently been cited as the most common cause of ACLR failure, 38,39,52,121 a study by the MARS (Multicenter ACL Revision Study) group 74 acknowledged the multifactorial nature of ACL revision failure, recognizing that most failures are due to a combination of technical error, trauma, and/or biological factors. Objective failure of the native ACL was defined by Daniel et al 26 as a side-to-side difference of greater than 3 mm. Revision ACLR failure was later defined by Wright et al 131 as a pivot-shift grade of 2+ or 3+ or a positive side-to-side difference greater than 5 mm. Previous authors have also identified failure to return to sport or persistent feelings of knee instability as subjective failures. 38,47,83 Given the complex nature of ACL failure, outside of graft rerupture, objective measures and subjective feelings of instability must be addressed on an individualized basis when revision surgery is being considered.
Posterior Tibial Slope
A risk factor for ACL injury that has received recent attention in the literature is a relative increase in the posterior tibial slope (PTS), which is the angle formed between a line perpendicular to the mid-diaphysis of the tibia and the posterior inclination of the tibial plateau (Figure 1). 40,59 Numerous radiographic studies have established an association between a high PTS and subsequent risk for ACL injury in adult 15,104,137 and pediatric populations. 27,88 However, not all studies corroborate this association 78 or have failed to do so in both sexes. 50,55,118 Dejour and Bonnin 29 reported that for every 10° increase in slope, an additional 6 mm of anterior tibial translation (ATT) can be expected in both the ACL-intact and the ACL-deficient knee. During axial loading through the tibiofemoral joint, vertical shearing forces are converted to anteriorly directed tibial translational forces. The ACL serves as the primary restraint to anterior translation, 16,37 so as the PTS increases, a greater force is applied to the ACL (or graft reconstruction) during functional loading. 73,77,99,100
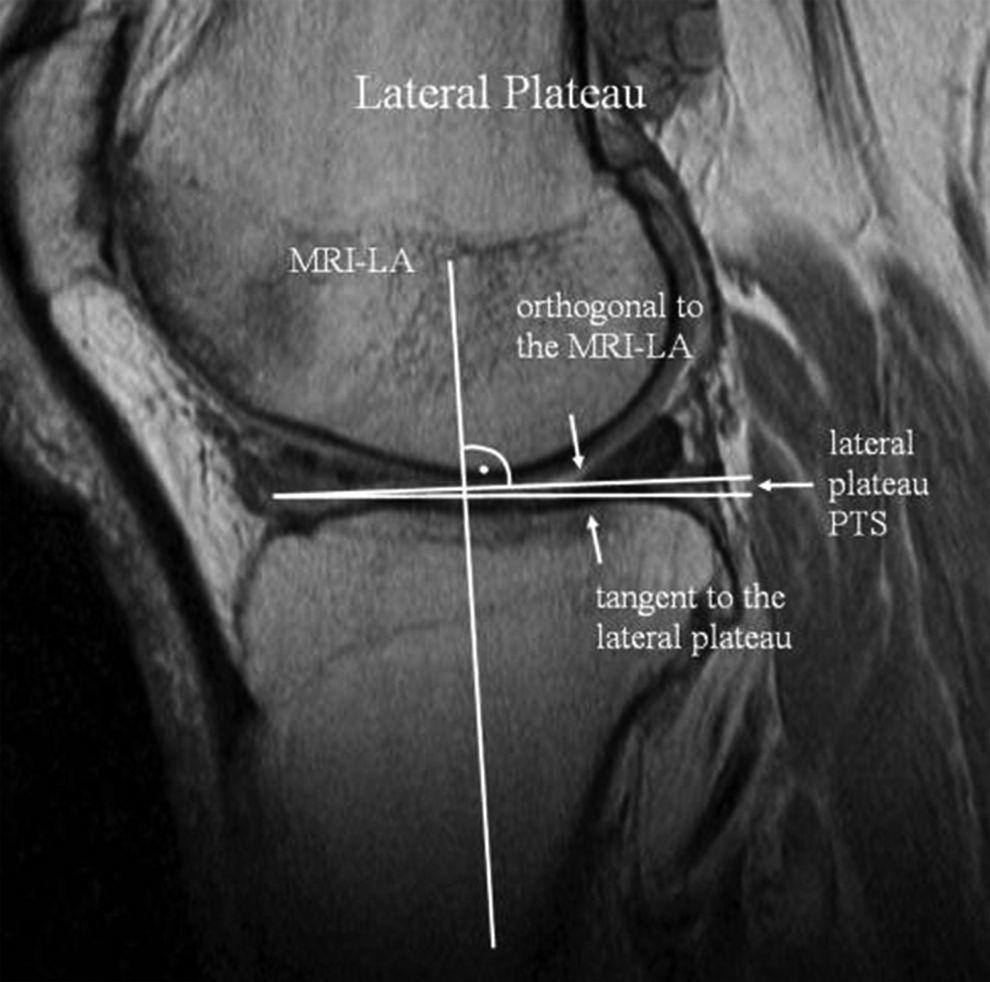
The center of the lateral tibial plateau with the preserved longitudinal axis (LA) determined on the central sagittal slice. The tangent to the lateral plateau is drawn to the proximal cortex border. MRI, magnetic resonance imaging; PTS, posterior tibial slope. (Reprinted with permission from Hudek R, Schmutz S, Regenfelder F, Fuchs B, Koch PP. Novel measurement technique of the tibial slope on conventional MRI. Clin Orthop Relat Res. 2009;467(8):2066-2072.)
Other studies have suggested that the lateral posterior tibial slope (LPTS) may be a more sensitive risk factor for ACL injury. 102,112 Han et al 46 demonstrated that the slope of the medial and lateral tibial plateau can be disparate in patients, but advanced imaging is needed to reliably identify these differences. A preferential increase in lateral slope results in greater anterior motion of the lateral tibial plateau compared with the medial plateau. This results in relative internal rotation of the tibia compared with the femur, placing increased stress on the ACL during axial loading. 35,77 While numerous studies have implicated the LPTS specifically as a risk factor, 27,55,102,112 others have found an increased PTS in general to be a risk factor for injury to the native ACL. 15,88,104,137
Little has been written about the effects of PTS on ACLRs or revisions. In a case-control study of 40 patients who had undergone ACLR, Li et al 63 demonstrated that 20 patients with failed reconstructions had significantly higher medial and lateral PTS than their counterparts who experienced successful reconstructions. Their study demonstrated that medial PTS 5° or greater resulted in an odds ratio of ACLR failure of 6.8 (P = .007), while for lateral PTS 5° or greater, the odds ratio of ACLR failure was 10.8 (P = .000). In a series of 181 patients, Webb and colleagues 125 determined that patients with a PTS 12° or greater as measured on lateral radiographs had 5 times greater odds of subsequent ACL injury after reconstruction and had an ACL reinjury rate of 59% in their series. Christensen et al 21 further validated these findings in a case-control study of 70 patients, demonstrating that patients with increased LPTS were significantly more likely to have early ACLR failures and that an increase of 2°, 4°, and 6° in the LPTS resulted in an odds ratio for graft failure of 1.6, 2.4, and 3.8, respectively.
Dejour et al 28 assessed 9 patients who underwent second revision ACL surgery combined with tibial deflexion osteotomies to address PTS greater than 12°; patients had significantly improved outcomes at a minimum follow-up of 2 years. No patients in their series had graft rupture or recurrent instability, 7 of the 9 patients reported good or better subjective satisfaction ratings, and Lysholm and International Knee Documentation Committee (IKDC) subjective knee form scores were significantly improved. Sonnery-Cottet et al 105 reported similar improvements in stability and functional outcomes in a series of 5 patients with a mean PTS of 13.6° (range, 13°-14°) who underwent closing wedge osteotomies to correct PTS at the time of repeat revision ACL, achieving a postoperative mean PTS of 9.2° (range, 8°-10°). These reports, although limited to a small cohort of patients, indicate that an osteotomy should be considered in the setting of a failed revision ACLR when a PTS of 13° or more is identified. Magnussen et al 67 recommended deflexion osteotomies only for patients with a slope of this magnitude who also have significant chronic anterior laxity as evidenced by increased ATT of at least 10 mm relative to the contralateral knee on standing radiographs. Furthermore, Cantin et al 18 stated that while an increased PTS may warrant consideration of a tibial deflexion osteotomy, this procedure should not necessarily be performed in all cases of increased PTS, particularly when another source of graft failure can be identified.
While previous studies have highlighted the efficacy and safety of simultaneous tibial osteotomy and ACLR in the setting of primary procedures, 12,82,120,135 recent results by Dejour et al 28 and Sonnery-Cottet et al 105 indicate that osteotomy can safely be performed during ACL revision. This reduces the inherent morbidity associated with 2 surgeries and simultaneously addresses all of the aberrant anatomic features that may compromise the reconstruction. Additional work is needed to elucidate the relative contributions of PTS and LPTS in the literature.
Varus Malalignment
In addition to sagittal malalignment, deviations in the coronal plane, specifically varus malalignment of the knee, have been implicated as a potential cause for increased ACL strain. 81,122 Varus malalignment is traditionally defined as greater than 3° of varus between the mechanical axes of the femur and tibia 9 or as a weightbearing line that passes medial to the center of the knee. 34 Cadaveric studies have demonstrated that higher tension forces are observed in the ACL when varus torque is applied to the extended knee. 71,72,79,122 Furthermore, several studies have identified that knees with varus thrust that undergo ACLR may be more likely to fail if the varus alignment is not addressed at the time of the reconstruction. 56,81,85,86,122 Varus-aligned ACL-deficient knees have also been implicated as a risk factor for progression of chondral and meniscal lesions. 42,53,114
Varus thrust refers to a dynamic alignment typically observed in varus knees, identified by an abrupt worsening of existing varus during the weightbearing phase of gait, with a return to a reduced varus alignment during the nonweightbearing (swing) phase. 20 Van de Pol et al 122 conducted a cadaveric study investigating the effects of increasing varus moments on ACL tension and lateral joint opening under axial loading conditions. The investigators observed that an extreme varus knee (12° hip-knee-ankle varus angle), particularly when associated with a varus thrust, produced significantly higher ACL tensions in both extension and 10° of flexion. Van de Pol et al 122 concluded that under these conditions, enough tension may be placed on an ACL graft to cause failure of an ACLR; furthermore, the investigators suggested that a high tibial valgus osteotomy be considered in ACL-deficient patients with varus alignment and associated varus thrust. In 41 younger adult patients undergoing ACLR, Noyes et al 82 demonstrated the efficacy of high tibial osteotomy (HTO) in patients with ACL-deficient knees and associated varus malalignment. The investigators recommended HTO for symptomatic patients with instability and limited medial joint arthrosis who wished to return to a higher level of activity. Patients who underwent the procedure had statistically significant improvement in symptoms, and overall patient satisfaction was high (88%). In a study by Bonin et al, 12 at 12 years of follow-up, 83% of patients (25/30) who had undergone a combined ACLR and a valgus-producing HTO had returned to moderate, intense, or very intense levels of sporting activity. Additionally, a low rate of progression of arthritis (17%) was observed radiographically among these patients.
In patients with a noted varus knee, preoperative assessment should include clinical inspection of the patient’s gait to determine whether a varus or hyperextension thrust is present. Long-leg weightbearing radiographs should be obtained to assess osseous lower extremity alignment using the hip-knee-ankle angle and to identify medial tibiofemoral compartment degeneration. 52 Radiographs should also be used to identify patients with constitutional varus, who are not considered candidates for HTO. ACL revision may be performed as a staged or combined procedure. 30,84,129,135 While previous authors have identified a high rate of associated complications with combined procedures, 60,82 more recent literature has recognized simultaneous procedures to be efficacious and produce satisfactory results in double varus knees with associated ACL injury. 64,96,135
Indications for HTO in ACL-deficient knees with varus alignment include medial compartment arthritis or varus thrust in knees with tibiofemoral malalignment 2,56,60 and instability in double and triple varus knees. 14,84 In light of clinical studies demonstrating improved outcomes in symptomatic patients with varus malalignment who have undergone HTO during ACLR, it is reasonable to conclude that these procedures should be considered as a salvage procedure for young patients with double and triple varus knee malalignment for whom ACLR has failed and who wish to return to an increased level of activity or recreational sport. Not only does the procedure improve clinical outcomes, but biomechanical evidence suggests that it reduces stress on the ACL graft and reduces the progression of arthrosis. Lateral closing wedge HTO has recently been demonstrated in a cadaveric study to have the advantage of more reliable PTS correction than medial opening wedge HTO (Figure 2), in addition to significantly decreasing ATT. This led the authors of the study to advocate for lateral closing wedge HTO in the setting of recurrent ACLR failure, as it normalizes ACL kinematics, protecting the graft. 90 Furthermore, other studies have shown that opening wedge HTO has a tendency to increase the PTS. 33,75,111 However, we would advocate that surgeons perform the osteotomy with which they can reliably achieve the most predictable outcomes.

An anteroposterior weightbearing radiograph of the right knee demonstrates an anterior cruciate ligament reconstruction with medial opening wedge high tibial osteotomy. (Image courtesy of Jacqueline Munch Brady, MD.)
Anterolateral Ligament
Anterolateral rotary instability is another potential cause of failure that should be considered in patients with multiple failed ACLRs. Previous research has demonstrated that rotational instability can persist in up to 25% of patients following ACLR. 106 The anterolateral ligament (ALL) is an extra-articular structure of the knee that is often torn in association with ACL injuries, in as many as 78% of cases 22 (Figures 3 and 4). The ALL has been observed to act as a secondary restraint to ATT and rotational instability. 108,115,117 ACL-deficient knees with an associated ALL injury can display severe rotatory instability and cause persistent symptoms of giving-way. Injury to the ALL can be difficult to diagnose clinically, and therefore preoperative magnetic resonance imaging or ultrasonographic findings may suggest the diagnosis. 43,58 Terry et al 116 demonstrated that varying degrees of instability on pivot-shift and Lachman examination maneuvers in ACL-deficient knees did not correlate with ACL injury but instead correlated most closely with variations in injury to the ALL. Failure to address this may ultimately lead to articular cartilage and meniscal damage 3 if the ALL is not reconstructed concurrently with the ACL. 103

Photograph of a typical right knee after complete dissection of the anterolateral ligament (ALL), popliteus tendon, popliteofibular ligament, and lateral collateral ligament (LCL). (Reprinted with permission from Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J. Anatomy of the anterolateral ligament of the knee. J Anat. 2013;223(4):321-328.)

An anteroposterior weightbearing radiograph of the left knee demonstrates a Segond fracture. The Segond fracture is currently thought to be a bony avulsion of the anterolateral ligament from the lateral tibial plateau.
Historically, lateral extra-articular reconstruction, involving nonanatomic reconstruction of the anterolateral structures, has demonstrated mixed clinical results in the literature due to abnormal joint kinematics leading to poor long-term outcomes, including arthrosis, residual instability, and joint overconstraint. 6,69,87,103,119,136 Distinction between the ALL and the collective anterolateral structures (including the iliotibial band and anterolateral capsule) must be made when referring to literature about extra-articular reconstructions, as lateral-plasty or lateral extra-articular tenodesis procedures have more recently begun to be replaced by the development of anatomic ALL reconstructions (ALLRs). The ALL is increasingly recognized to be a distinct anatomic structure separate from the “capsulo-osseous layer of the iliotibial band” previously described, and thus these reconstructions seek to address this factor. 23,25,31,54,106 In the literature, ALLR has been described as providing rotatory stability without overconstraint, 48,106 a problem noted by Slette et al 103 in a systematic review of lateral extra-articular tenodesis procedures.
The stabilizing function of the iliotibial band and soft tissue elements of the lateral capsule have long been understood, 10,116 but until recently the biomechanical contribution of the ALL had not been fully elucidated. Several cadaveric kinematic studies have helped to identify the function of the ALL. 97,103,115,117 The intact native ALL has been shown to improve translational and rotational stability in ACL-deficient knees compared with the same knees with both the ACL and ALL sectioned. 92,115,117 Tavlo et al 115 demonstrated significantly increased internal rotation in ACL-deficient knees when the ALL was detached from its tibial insertion, and rotatory stability in these knees was not re-established by reconstruction of the ACL alone. Schon et al 97 found that anatomic ALLR in the setting of a concomitant ACLR significantly reduced rotational instability compared with ACLR without ALLR. However, no matter the angle of graft fixation, overconstraint was observed for internal rotation at greater than 30° of flexion and for the pivot-shift test at angles greater than 45°. 97 The senior authors’ (B.G.) preferred technique for ALLR is a modified Lemaire technique, which involves the use of a central slip (10 mm in size) of the iliotibial band. 127 Several authors have shown the modified Lemaire procedure to be biomechanically superior to the “anatomic” ALLRs. 57,127 This slip is harvested in an open fashion and then rerouted underneath the lateral collateral ligament. The central slip is then fixed with a medium staple proximal and posterior to the lateral condyle. The knee is placed at 90° of flexion and relative external rotation during final fixation.
While ALLR may play a role in improving stability, caution should be taken with this approach in patients undergoing primary ACLR, 48,106 especially given the risk of overconstraint. 97 Sonnery-Cottet et al 106 suggested combined ACLR and ALLR only in the setting of chronic ACL lesions, grade 3 pivot shifts, participation in pivoting or competitive sports, the presence of a Segond fracture, or a lateral femoral notch sign. 49 Helito et al 48 similarly recommended that the combined ACLR and ALLR be reserved for cases of ACL revision without an apparent cause of failure or high-grade pivot shifts. Combined reconstruction in this setting offers the advantage of restoring the attenuated lateral structures, thus restoring normal joint alignment and kinematics. To date, only 1 case series is available, which involved 92 patients who underwent a combined ACLR and ALLR with a minimum 2-year follow-up. 106 Patients had significantly improved Lysholm scores and subjective and objective IKDC scores. This series of patients also had significant decreases in anterior laxity, as only 7 patients had a postoperative pivot-shift score of 1, whereas all patients had a preoperative pivot-shift score of 1 or higher. Only 1 patient in this series had ACLR graft of rupture. 106
Although these studies may suggest a potential role for ALLR in select patients with grade 3 pivot shifts and patients with ACLR failure in whom another cause cannot be identified, further prospective studies are needed to evaluate the efficacy of these procedures and further determine their indications. The Stability Trial is a multicenter randomized controlled trial that is currently being conducted by Getgood and others to compare the outcomes and rates of graft failure for high-risk patients who undergo an ALCR with and without lateral extra-articular tenodesis.
Meniscal Deficiency
Among patients with multiple previous knee surgeries undergoing revision ACLR, many patients are noted to have a high incidence of associated chondral and meniscal abnormality. 1,13,126 Meniscal integrity has been implicated as a possible cause for recurrent ACLR failure warranting consideration. It is well established from cadaveric studies that the medial meniscus serves as a secondary restraint to ATT in the ACL-deficient knee. 62,80,101 However, biomechanical studies have also implicated the lateral meniscus as a stabilizer during rotatory axial loading, exerting its effect by preventing the pivot shift 80 (Figure 5). In a multicenter retrospective study of 293 patients, Trojani et al 121 demonstrated that patients who underwent meniscectomy before, during, or after primary or revision ACLR had significantly worse stability than those patients with conserved menisci, as evidenced by lower pivot-shift control and subjective knee scores. Wu et al 132 obtained similar findings in 63 patients who had undergone ACLR and meniscectomy. These patients had significantly lower subjective function scores and ability to perform a single-leg hop test compared with patients with intact menisci at an average 10.4 years of follow-up. These studies validate the role of the menisci as stabilizers in the ACL-reconstructed knee and suggest the importance of performing meniscus-preserving procedures during ACLR.

The effect of medial meniscectomy (MM; n = 8) and lateral meniscectomy (LM; n = 8) in response to a pivot-shift test. Anterior tibial translation in the lateral compartment for the intact knee, isolated ACL deficiency ACL–single meniscectomy (ACL/LM-deficient or ACL/MM-deficient), and ACL–double meniscectomy (ACL/LM/MM-deficient) are shown. The MM group had a significant difference between ACL-deficient and ACL/LM/MM-deficient knees (P < .05). The LM group had a significant difference between ACL-deficient and ACL/LM-deficient knees (P < .01). ACL, anterior cruciate ligament; ACL out, ACL-deficient; ACL/MM out, ACL/MM-deficient; ACL/MM/LM out, ACL/MM/LM-deficient. (Reprinted with permission from Musahl V, Citak M, O’Loughlin PF, Choi D, Bedi A, Pearle AD. The effect of medial versus lateral meniscectomy on the stability of the anterior cruciate ligament-deficient knee. Am J Sports Med. 2010;38(8):1591-1597.)
Ramp lesions are a specific type of meniscal tear that have recently been reported to occur frequently in the setting of ACL injuries. 19,66,113 In a series of 868 patients by Liu et al, 66 16.6% of patients undergoing ACLR were found to have ramp lesions, which were defined as longitudinal tears of the peripheral attachment of the posterior horn of the medial meniscus. Some authors have referred to this tear pattern as the “Bankart” lesion of the knee. 70 The posterior horn is recognized as a critical stabilizer in the ACL-deficient knee, 80 and Bollen 11 originally described the lesion as being associated with anteromedial rotatory subluxation. In a more recent cadaveric study, sectioning of the posteromedial meniscocapsular junction in an ACL-deficient knee resulted in a significant increase in ATT and external rotation. 110 Ramp lesions play a role in disrupting an important secondary stabilizer of the knee, and arthroscopic examination of the posterior structures of the knee and repair of ramp lesions must always be undertaken when revision ACL surgery is performed (Figure 6).

Arthroscopic view of a ramp lesion in a left knee. (A) View through the anterolateral portal; the posterior horn of the medial meniscus seems normal. (B) View through the intercondylar notch; the dashed area shows the ramp lesion. (C) View through the posteromedial portal. MFC, medial femoral condyle; MTP, medial tibial plateau; PM-Cap, posteromedial capsule; SN, spinal needle; PHMM, posterior horn of the medial meniscus. (Reprinted with permission from Liu X, Feng H, Zhang H, Hong L, Wang XS, Zhang J. Arthroscopic prevalence of ramp lesion in 868 patients with anterior cruciate ligament injury. Am J Sports Med. 2011;39(4):832-837.)
Several authors have noted that the increased strain placed on the ACL graft in patients with ACLR and deficient menisci may result in a higher risk of graft failure. 32,47,109 In a cadaveric study, the biomechanical interdependence of the ACL graft and the medial meniscus was demonstrated as in situ forces on the ACLR graft were 33% to 50% higher in the absence of the medial meniscus. 89 In another study of patients who underwent ACLR, patients with medial or lateral meniscal deficiency were 4.5 or 3.5 times more likely to experience ACLR failure, respectively. 94 In a cadaveric study by Spang et al 107 involving knees that had undergone medial meniscectomy, anterior-posterior loads up to 150 N were applied to knees in 30°, 60°, and 90° of flexion, resulting in significantly high tibial displacement at all angles. Subsequent meniscal allograft transplant (MAT) restored tibial displacement to normal at 30° and 90° of flexion and returned ACL strain values to normal at 60° and 90°.
In light of these findings, many have begun to advocate for the role of concomitant MAT in patients undergoing ACLR who have irreparable meniscal injury or have undergone previous total or near-total meniscectomy. 24,45,91,98,109 The goal of this intervention is to restore stability, thus protecting the ACL graft and delaying future chondral degeneration. 98 In general, MAT is indicated for younger patients with normal alignment and minimal chondrosis who have pain or in whom previous ACLRs have failed. 76,93 Our indications for a combined MAT/ACLR procedure are for patients with a previous failed ACLR who still have subjective joint line pain or symptomatic instability with an absent meniscus, including those with an absent posterior root or those with less than 40% of the meniscus intact.
Several authors have investigated the outcomes of MAT with concomitant ACLR. In a small series of patients who underwent valgus HTO, ACLR, and MAT, 6 of 7 (85.3%) patients experienced good or excellent results. 17 Sekiya et al 98 demonstrated that among 28 patients who underwent MAT and ACLR, 85.7% had normal or nearly normal IKDC scores and 90% had normal or nearly normal Lachman and pivot-shift tests. In another small series of patients who underwent the combined intervention, all patients had long-term satisfaction with the procedure at 8.5 years follow-up, and 7 of the 8 patients had normal or nearly normal restoration of stability following the procedure. 45 In a group of 31 patients who underwent isolated MAT (11 patients) or MAT with ACLR (20 patients), all but 1 patient reported that their knee function was normal or nearly normal; an average side-to-side difference of 2 mm was observed, and 63% of patients reported rare or no instability. 134 The combination of MAT and ACLR is safe and effective and should be considered in the context of revision ACLR to prevent recurrent failure of the ACL graft by improving stability.
Conclusion
Although recurrent ACL failure affects only a relatively small subset of patients who undergo ACLR, revision ACLR is a technically challenging procedure that requires careful attention to detail and consideration of all the factors that contributed to previous failures. Even though the vast majority of ACL graft failures occur as a result of technical errors, failure to recognize and address certain anatomic factors highlighted in this review may also represent missed opportunities to ensure a successful revision. If these factors are corrected, stress on the ACL graft can be minimized, thus reducing the risk of future graft disruption and failure. While improved stability of the knee can be achieved in revision ACLR, surgeons should counsel patients about their expectations preoperatively to ensure a successful outcome following surgery.
Footnotes
Acknowledgment
The authors acknowledge Richard Puzzititello for his assistance in the preparation of this manuscript.
One or more of the authors has declare the following potential conflict of interest or source of funding: B.R.S. receives research support from DePuy Synthes.