
Abstract
Background:
Motocross is a form of motorcycle racing held on established off-road circuits and has been a recreational and competitive sport across the world for >100 years. In the United Kingdom alone, motocross has grown into a phenomenally ambitious and popular franchise. There are >200 motocross clubs across the country, permitting >900 events annually.
Purpose:
To assess the current trend of spine-related motocross injuries over the past 5 years.
Study Design:
Descriptive epidemiology study.
Methods:
Data were prospectively collected over 5 years (August 2010–August 2015) at our regional trauma and spine unit, regardless of whether the rider was performing the sport competitively or recreationally.
Results:
During the study period, spine-related injuries were identified for 174 patients (age range, 6-75 years) who were directly referred to our department following recreational or competitive motocross, with most injuries being sustained within the early spring and summer months, representing the start of the motocross season. A significant number of injuries were in males (n = 203, 94%), with the majority of injuries occurring within the 21- to 30-year-old age group. A total of 116 (54%) injuries required operative treatment. The most common spinal injury was thoracolumbar burst fracture (n = 95), followed by chance fractures (n = 26).
Conclusion:
This data series emphasizes the prevalence and devastation of motocross-related spinal injuries in the United Kingdom and may serve in administering sanctions and guidelines to governing bodies of motocross. The spinal injuries that occur during motocross have significant capital connotations for regional spinal centers. The recent surge in motocross popularity is correlated with the number of injuries, which have increased over the past 5 years by almost 500%.
Motocross and various modes of all-terrain motorcycling have emerged as one of the most popular sporting activities across the world, where it is practiced by millions of people; however, very little has been written on motocross spinal injury and its prevention. For >100 years, the sport of motocross has been practiced in competition and for leisure pursuit. Throughout the United Kingdom (UK) and the world, there are established off-road circuits where motorcycle racing events are carried out. 19,20 The first established competitions were held as early as 1906, and it is from here that the sport has grown in reputation and following. 19,20 The sport’s popularity has grown immensely across the world, with its image becoming more prestigious with its fame and approachability. In the UK alone, there are >200 motocross clubs, and >900 annual events are carried out throughout the country; this follows the first British national competition in 1924, which was held in Surrey. 3,4,6
There is a wide age range for competitive motocross, ranging from 6 to 65 years. There are also exceptions to this, with reports of children at the age of 3 years taking active part in competitive racing. 10 The advertising for motocross merchandise and equipment is diverse. The machines are terrifically forceful and vigorous, where speeds in excess of 100 mph and weights >100 kg are commonplace. 3,6,19
The motocross competitions are typically held on weekends throughout the spring and summer months, with approximately 100 to 200 registered participants. Despite the seasonal competition pattern, enthusiastic riders practice throughout the year. The accessibility of the competitions is particularly appealing with an online application and modest enrollment fees of approximately £100 (US$135).
The emergency doctors, surgeons, and spinal injury team at our regional spinal trauma unit have noticed an increase in severe spinal injuries during participation in motocross events. The circulation and magnitude of spinal injuries in the motocross population in the UK are not known, yet there is plenty in the literature regarding injuries in competitive motorcycle and motorcar racing. 13,18 Given that there is no published evidence analyzing the relationship between motocross sporting events and the associated spinal injury patterns in the UK, this study was designed to prospectively review our experience and quantify those observations.
The annual incidence of spinal injuries worldwide is approximately 50 cases per million people, and up to 90% of these cases are due to trauma. 24 The demographic trends of spinal injuries show that males in young adulthood are most at risk, with a ratio of 2:1 as compared with females. 7 In comparison with the general population, people with spinal injuries have an increased mortality rate, which is highest in the first year after injury. 9
The aim of this study was to evaluate the nature and number of spinal injuries related to motocross riding and their requirement for operative intervention. We present the first case series of spinal motocross injuries in the UK.
Methods
Data were prospectively collected over 5 years (from August 2010 to August 2015) at our regional trauma and spine unit. All injuries sustained via motocross vehicles were included in this study, regardless of whether the rider was performing motocross competitively or for training purposes. Patients were referred acutely via the emergency department.
Inclusion criteria comprised all spinal injuries sustained by motocross only, which included spinal cord injuries and vertebrae column fractures. Injuries sustained from off-road mountain biking or a motorcycle/motor vehicle were excluded.
Injuries were identified for 174 patients who were directly referred to our department following recreational or competitive motocross.
The data collected included basic demographic details (name, age, sex), the type of injury sustained, the need for admission/surgery, and any associated complications. The information was prospectively collected from dictated hospital notes (inpatient and outpatient) from trauma and orthopaedic consultants and specialist registrars in our department/regional spinal unit. Results were tabulated with Microsoft Excel.
Results
During the period studied (5 years), 174 patients were referred to our trauma and specialist spinal department. A total of 216 injuries were recorded, ranging from 1 to 6 injuries per patient. The majority of injuries occurred in patients engaged in the sport for competitive purposes, as opposed to recreational purposes.
A significant majority of injuries sustained were in male patients (n = 203, 94%) (Figure 1). The patients’ age range was 6 to 75 years, with the majority of injuries in the age group of 21 to 30 years (Figure 2). The greatest number of injuries occurred in early spring, with a noticeable peak again during the transition between autumn and winter (Figure 3). A total of 116 (54%) injuries required operative treatment (including halo orthosis immobilization) (Figure 4), with some requiring multiple procedures (≥2). The spectrum of spinal injuries is extensive; see Figure 5 for the distribution of injuries.

Percentage sex distribution of motocross injuries.

Age distribution of spinal motocross injuries.

Monthly distribution of motocross injuries.

Percentage of motocross patients receiving spinal surgery.
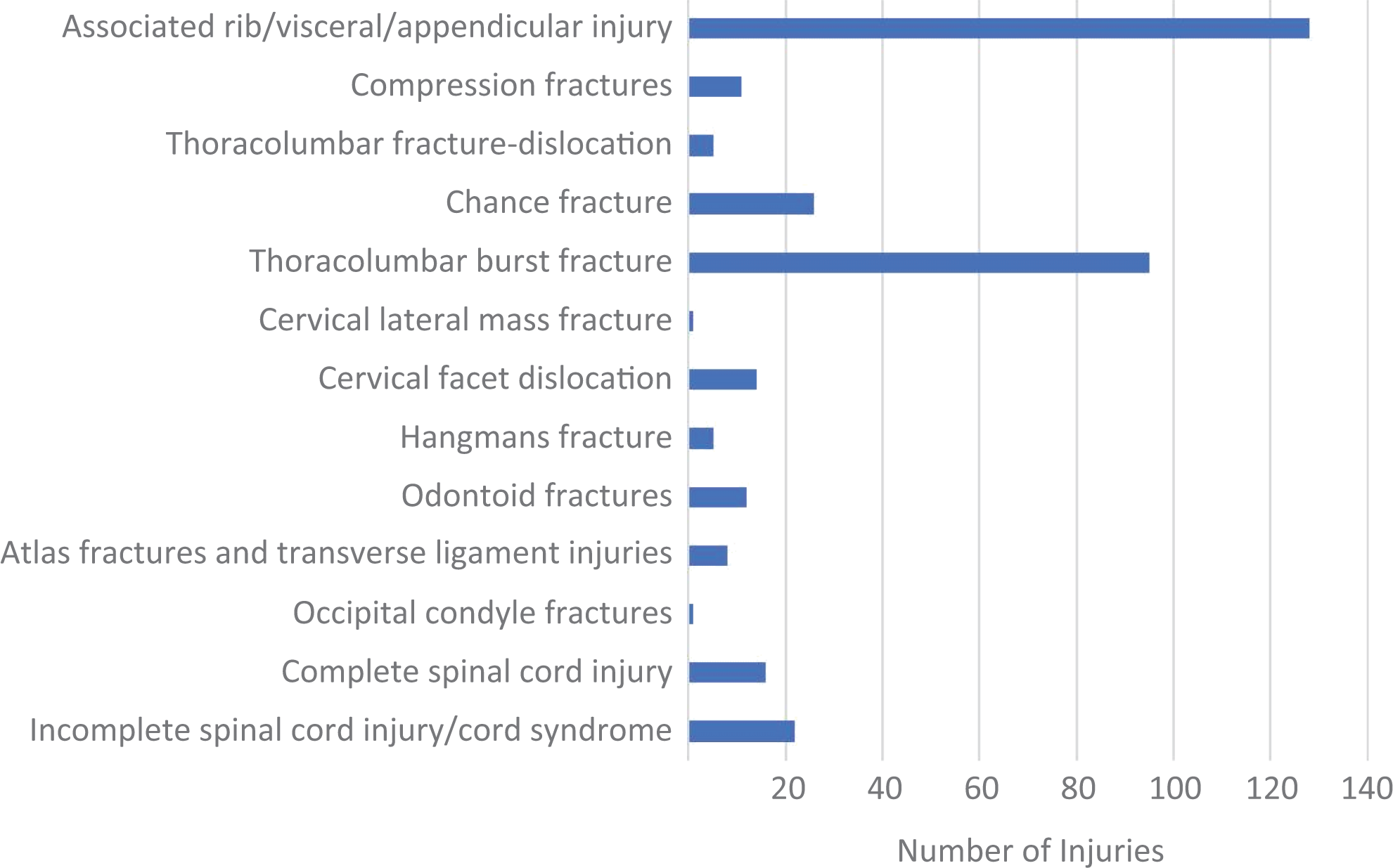
Distribution of spinal motocross injuries.
The most common injury sustained was associated rib and visceral injury, and the most common spinal injury was thoracolumbar burst fracture (n = 95), followed by chance fracture (n = 26). A convincing proportion of these injured patients sustained ≥2 injuries; overall, 110 patients (63%) suffered 128 associated injuries, including rib fractures, abdominal injuries, and appendicular skeletal fractures. The mean length of stay of all injured patients was 7 days (range, 2-12 days). Forty-five patients (25%) required admission to a high dependency unit or intensive therapy unit, 20 (11%) needed emergency laparotomy procedures, 5 required neurosurgical intervention, and 20 required monitoring following chest injuries.
All the patients in this series required formal spinal orthopaedic follow-up in fracture clinics or specialist spinal clinics. Forty-two patients were not residents in the local area of our unit; therefore, the follow-up for these patients was arranged at their respective local departments. All local patients required at least 3 follow-up appointments, regardless of whether their treatment was operative or nonoperative.
In this 5-year series, there was a substantial increase in the number of annual spinal injuries recorded (Figure 6). In addition to the increase in the number of injuries over the past 5 years, there was a constant increase in the number of spinal operations for these injuries (Figure 7). There were 125 (72%) cases of chronic pain reported in our series. Regarding return to work, only 54 (31%) patients returned to their preinjury mode of employment.

Number of annual spinal injuries over the past 5 years.

Number of annual spinal operations for motocross injuries.
Discussion
This catalog of injuries is the first epidemiologic study of this weight in the UK for spinal injuries sustained as a consequence of motocross collisions. The majority of injuries occurred in early spring, which coincides with the start of the motocross season, where riders may be more susceptible after the winter break with regard to being unacquainted with the treacherous territory and inexperienced in terms of skill level. We suspect that the winter peak occurs as a result of the course being more venturesome as the conditions become precarious.
Injuries to the vertebral column and spinal cord are affiliated with a liability of complications that can be debilitating and even life threatening, such as pressure ulcers, chronic pain, and respiratory complications. 1 The management and prevention of these complications require continued nursing care and rehabilitation. The return-to-work rate in our series (31%) is lower than the published unemployment rate of 60% following spinal injury. 15,23 The health and socioeconomic consequences are serious following spinal injury, with a 20% to 30% risk of depression, which can occur as a result of reduced mobility and social independence. 8,23
There is a plethora of data in the literature describing spinal injury patterns that occur as a result of motor vehicle and motorcycle collisions. 14,17,21 However, patterns and outcomes of spinal injuries associated with motocross accidents in the UK have not been previously reported.
The sport of motocross has gained global popularity, with the annual number of completive racers doubling in the past 5 years. 3,20 This trend is represented by our data, as the number of injuries increased by a factor of 5 during our study period—from 15 (2010-2011) to 78 (2014-2015). This increase in the number of injuries is likely to be multifactorial regarding more referral and more participants. Historically, most spinal fractures have been treated conservatively, depending on mechanism and spinal stability. However, technological advances in spinal surgical equipment and the theater kit improve a surgeon’s options and potential surgical solutions for complex spinal injuries. 18,19 The data from this series reflect this, as the number of operations increased from 11 (2010-2011) to 41 (2014-2015)—an increase by a factor of 4.
This study shows the consequences and prevailing occurrence of spinal injuries as a result of motocross. The vehicles can reach speeds of 100 mph through risky land, and this seems to captivate the young male racer. The current literature examining motocross injuries states that between 1997 and 2006, the spinal injury rate increased by almost 500% in the United States. 16,22
The acute health care cost implications are certainly not trivial, as the estimated cost of an acute hospital bed in the UK is approximately £250 (US$336) for an overnight stay, in addition to the cost of operative intervention summating to approximately £5000 (US$6730) per day and, of course, the fees for patient follow-up. 5,11 It is also important to consider the supervening purse for continued care and sick pay.
The limitations of this study are that we have not followed up the patients formally with regard to pain and disability. The use of the Oswestry Disability Index is the most commonly used outcome measure for low back pain. 12 A further study can use this index to quantify the disability and pain. We have also not evaluated the power of the motorbike, track architecture, and course assurance plans; therefore, we cannot make any outcome about their effect on safety. The patients included in this study were followed up until the present time (August 2015).
The dominant sources of spinal cord injury are road traffic collisions, falls, and violence (including attempted suicide). However, there remains a substantial fraction of traumatic spinal cord injury resulting from sports-related injuries. Practical interpositions should be reviewed, such as course design and speed limits on vehicles, and an inspection of safety equipment should be conducted, including helmets and neck braces.
It is still well documented that some complications related to spinal cord injuries are a consequence of inadequate on-scene medical care and rehabilitation services. 2 Improvement dimensions should be aimed at efficient and expert prehospital management with prompt recognition and evaluation, followed by expeditious commencement of immobilization and appropriate transfer.
Conclusion
The study findings serve to emphasize the prevalence and devastation of motocross-related spinal injuries in the UK. This may service in administering sanction and guidelines to governing bodies of motocross. The spinal injuries that occur during motocross have significant capital connotations for regional spinal centers. The recent surge in its popularity is represented by the number of injuries increasing in the past 5 years by almost 500%. We feel that it is imperative that the accepting emergency departments take into account the high-velocity mechanism of a motocross injury and formulate a plan for potential sinister spinal injury resulting from this high-energy trauma.
Footnotes
Acknowledgment
The authors thank Ellen Stockton and the Trauma secretaries at Royal Shrewsbury Hospital.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was approved by the Robert Jones and Agnes Hunt Orthopaedic and District Hospital NHS Trust.