
Abstract
Background:
Ultrasound (US)–guided intra-articular hip injections have been proposed in the literature to be accurate, reliable, and safe alternatives to fluoroscopy-guided injections.
Purpose:
To evaluate the accuracy of US-guided magnetic resonance (MR) arthrogram injections of the hip performed in the office setting by a single orthopaedic surgeon and elucidate the potential effects that patient age, sex, and body mass index (BMI) have on contrast placement.
Study Design:
Case series; Level of evidence, 4.
Methods:
From a review of the senior author’s office database, 89 patients (101 hips) who had US-guided MR arthrogram injections performed between December 2014 and June 2016 were identified. Official radiology reports were evaluated to determine whether extra-articular contrast was noted. Patient variables, including BMI, age, and sex, were evaluated between patients who had inappropriately placed contrast and those who did not.
Results:
Of the 101 hip injections, there were 6 cases that demonstrated inadequate contrast placement within the joint, likely secondary to extravasation or incorrect placement; however, an MR arthrogram was adequately interpreted in all cases. There were no significant differences noted between those with appropriate versus inappropriate contrast placement when evaluating BMI (P = .57), age (P = .33), or sex (P = .67), and neither group had an adverse event.
Conclusion:
US-guided injections are safe and accurate alternatives to fluoroscopy-guided injections in the office setting, with 94% accuracy. Furthermore, BMI, age, and sex did not play a statistically significant role among patients with inappropriately placed contrast.
Keywords
Magnetic resonance (MR) arthrography is widely accepted as a preferred imaging modality for evaluating abnormalities of the hip, including labral tears and acetabular impingement syndromes. While fluoroscopy has traditionally been the imaging modality of choice to ensure correct placement of intra-articular contrast, sonographic guidance is now becoming a preferred method among clinicians as excellent accuracy has been demonstrated. 5 Additionally, the use of ultrasound (US) eliminates the exposure of ionizing radiation to both the patient and the provider, allows the enhanced visualization of neurovascular structures, eliminates the possibility of an allergic response to iodinated contrast, is cheaper, and is more accurate than landmark-guided injections. 6,8 –10 In 2015, the American Medical Society for Sports Medicine systematically reviewed the literature for US-guided and landmark-guided injections of major joints (including hips) and concluded that there was strong evidence that US-guided injections are accurate and cost-effective. 7 A US-guided injection of contrast material can be performed in an office setting in a timely manner, reducing patient appointment times and allowing for expedited imaging results.
The purpose of this study was to investigate the accuracy of MR arthrogram injections of the hip in the orthopaedic office setting under US guidance. Patient-specific variables, including age, sex, and body mass index (BMI), were analyzed to determine whether they affect the accurate placement of contrast for MR arthrogram injections of the hip. Our hypothesis was that US-guided injections of the hip would be an accurate and safe way to deliver intra-articular contrast for MR arthrograms.
Methods
Institutional review board approval was obtained to conduct this study. A retrospective review of the billing data from the senior author’s (M.N.) practice from December 2014 to June 2016 was conducted to identify all patients who received diagnostic MR arthrograms of the hip. From this cohort, only patients who received US-guided intra-articular contrast injections in hips that had not undergone previous surgery were included in the study. None of the patients receiving US-guided intra-articular contrast injections in the hip were excluded. Medical records were reviewed for age, sex, and BMI. The radiologist-interpreted MR arthrogram reports were obtained for each patient and reviewed to determine if there was any mention of inadequate contrast material within the hip joint and/or extra-articular contrast.
Ultrasound-Guided Injection Technique
A US system (SonoSite) was positioned on the contralateral side to the affected hip with the screen in the line of sight of the operator. The skin overlying the hip was sterilized with an alcohol wipe. A wide, curvilinear probe was placed in a transverse plane parallel to the inguinal ligament and used to identify the femoral artery and vein above the hyperechoic femoral head. The probe was then moved laterally to just above the hyperechoic femoral head and rotated to an oblique sagittal position so that the probe marker was aimed toward the umbilicus. The probe plane was approximately 45° to the longitudinal axis of the body. The femoral head, femoral neck, anterior capsular recess, and iliofemoral ligament were visualized; any masses or fluid collections were noted. The probe was slid back and forth until an optimal view was obtained of the head and neck junction.
A superficial wheal of local anesthetic was placed at the point of the planned needle entry, approximately 1 cm distal to the transducer. A 14.5-mL mixture of 0.5 mL Optimark (Mallinckrodt Inc) with 14 mL of 0.5% Marcaine (Hospira, Inc) was placed in a 20-mL syringe. A 20-gauge, 3.5-inch standard cutting spinal needle was guided in plane under real-time US guidance to the anterior capsular recess. When the needle tip was clearly visualized in the intracapsular head and neck junction, the entirety of the solution was slowly injected under low pressure. Successful targeting of the joint space was confirmed by the spread of anechoic fluid under the iliofemoral ligament within the anterior capsular recess (Figures 1 –3).

The patient is supine with the hip in a neutral position, and the ultrasound transducer is placed in line with the femoral neck.
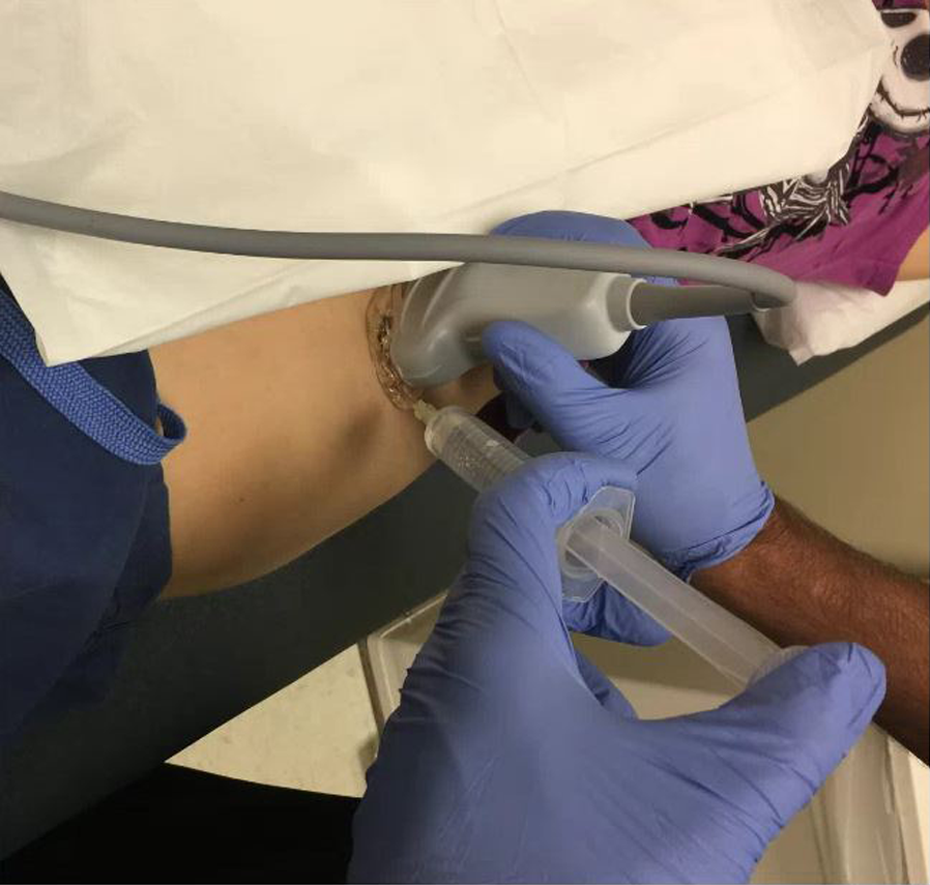
A 22-gauge, 3.5-inch spinal needle is placed in plane with the transducer and inserted into the anterior capsular recess for an intra-articular contrast injection.
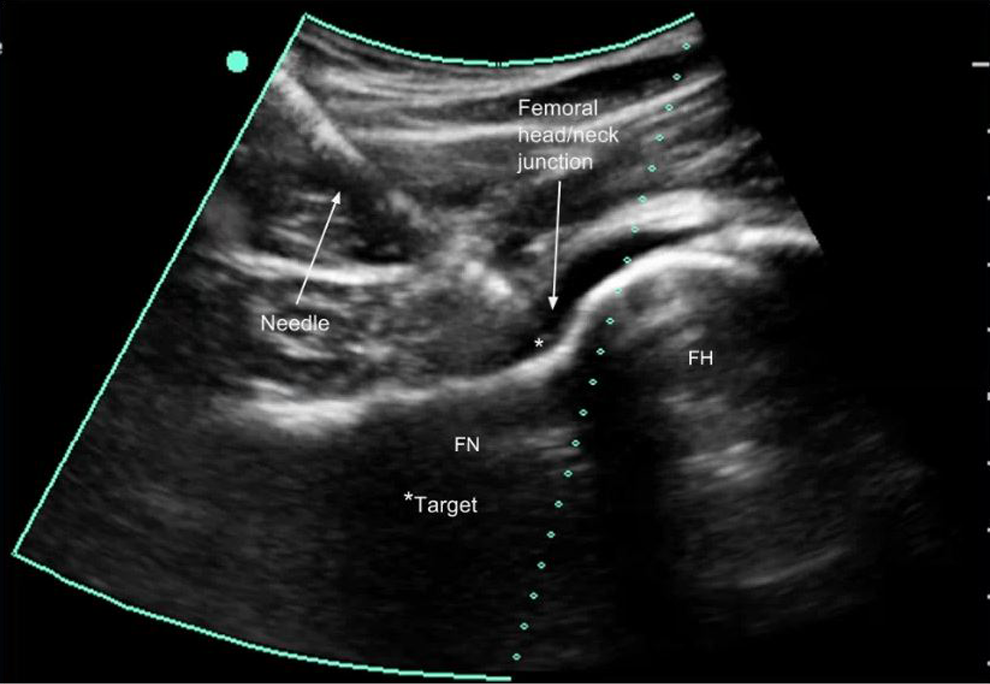
Ultrasound image with a needle in the anterior capsular recess. FH, femoral head; FN, femoral neck.
A single orthopaedic surgeon who was fellowship trained in sports medicine performed all injections with the aid of a portable SonoSite device. The MR arthrograms were performed immediately after the US-guided injections within the same facility, a large single-specialty private practice with clinics and a facility-owned MR imaging machine in the same building. This technique is only practical if the MR imaging machine is within the same facility where the injections are performed. MR arthrograms were interpreted by 4 fellowship-trained musculoskeletal radiologists at an unaffiliated radiology center that was contracted with the orthopaedics facility to interpret imaging. Accuracy was based on success rates of US-guided hip joint injections and was validated by radiology reports that commented on the paucity of contrast or extra-articular contrast. Secondary relationships were based on patient age, sex, and BMI as well as corresponding US-guided MR arthrogram results.
Data were checked for normalcy using the Shapiro-Wilk test. Data were not normally distributed; therefore, the Mann-Whitney U test was used to analyze continuous variables (age and BMI), and the Fisher exact test was utilized to analyze sex. Statistical significance was set at P < .05. All statistical analyses were performed with SPSS version 23 (IBM).
Results
Eighty-nine patients underwent US-guided hip injections. Of these, 12 patients underwent bilateral hip injections, for a total of 101 hips injected. Statistics were calculated for the total number of injections. The mean age of the patients in this study was 37 years (range, 12-75 years), with 27 male and 62 female patients. The mean BMI was 25.6 kg/m2 (range, 17.7-41.5 kg/m2). There were 6 instances of inappropriately placed contrast (in 1 male and 5 female patients), yielding a 94% success rate. The results are summarized in Table 1.
Patient Demographics

There were no significant differences between the patients with inadequately placed contrast versus adequately placed contrast regarding age (P = .33), BMI (P = .57) or sex (P = .67). None of the patients in our study population developed a hematoma, acute nerve damage, or an allergic reaction.
Discussion
The purpose of this retrospective study was to investigate the accuracy of MR arthrogram injections of the hip in the office setting under US guidance. Our results demonstrate the accuracy of US-guided hip injections, with a 94% success rate. Previous studies have demonstrated similar results; however, this is the largest cohort of patients consecutively injected by a single orthopaedic surgeon to date. Byrd et al 4 reported on a large series of 206 hip injections performed by a nurse practitioner, achieving a 98% accuracy rate. More recently, Balog et al 2 reported a 96% accuracy rate for a series of 48 US-guided hip injections performed in an orthopaedic clinic by orthopaedic surgeons and orthopaedic physician assistants. Upon review of the data, the sole limiting variable to a successful MR arthrogram was inappropriately placed contrast, which led to a decreased volume of contrast within the hip capsule on imaging. In the 6 instances of filling defects, the musculoskeletal-trained radiologists noted that contrast was placed primarily in the iliopsoas musculature. Despite inadequate contrast, the radiologists were still able to comment on hip abnormalities, including the presence or absence of labral tears, impingement syndromes, and arthritis.
Mei-Dan et al 11 investigated the accuracy and safety of an anterior approach technique for non–imaging-guided intra-articular injections of the hip by the use of anatomic landmarks. They found that increased subcutaneous adipose tissue could lead to inaccurate needle placement. Similarly, Singh et al 14 concluded that a higher patient BMI correlated with lower success rates of hip injections by the nonradiological method. In contrast, our results suggest that the accuracy of US-guided hip joint injections in obese patients is similar to that of nonobese patients, and we did not identify any significance between filling defects and patient BMI, age, or sex. Furthermore, there were no reported instances of hematomas, acute nerve damage, or allergic reactions, rendering a procedural complication rate of zero.
From a patient-centric standpoint, in-office US-guided injections of the hip have been shown to be more convenient and less painful than fluoroscopy-guided hospital-based injections and are preferred by patients who have undergone both modalities. 12 With health care reform increasingly relying on patient feedback and evaluation, optimizing patient comfort is a legitimate consideration for today’s clinician. Compared with fluoroscopy-guided injections, US-guided injections decrease the radiation burden to both the patient and the provider. While recent studies have suggested that fluoroscopy-assisted arthroscopic surgery of the hip is safe, with relatively low radiation dosing, 3,13 it stands to reason that any radiation exposure is an occupational health hazard. There are also financial incentives to performing US-guided injections in the office setting: the facility relative value unit in 2016 was 1.77 for a US-guided hip injection compared with the nonfacility relative value unit of 2.60. 1 Performing injections in the office expands the scope of one’s practice and allows for increased financial productivity.
As Otjen et al 12 noted in their study of US-guided joint injections for MR arthrography in pediatric patients, US is likely more technically challenging than fluoroscopy, requiring more dexterity because concomitant transducer and needle manipulation is needed. In our practice, we have experienced an expeditious learning curve for US-guided hip injections, which is similar to that reported by Byrd et al 4 and Balog et al. 2 While our data do not demonstrate a clearly defined significant decrease in filling defects over time, no instances of inappropriately placed contrast were reported in the final 10 months of the data collection period. In the hands of an experienced clinician, the US method is safe, reliable, and reproducible.
Limitations
The US-guided injections were performed by a single orthopaedic surgeon with a high level of training in both US-guided hip joint injections and hip arthroscopic surgery. Generalizing our results to a medical professional who possesses variable skill sets and less familiarity with hip anatomy could be potentially misleading. The patients in this study had a mean age of 37 years. The relatively high success rate for the intra-articular placement of contrast might theoretically be higher in this cohort compared with older patients with arthritic conditions and unpredictable anatomy. Further studies may be useful in analyzing groups of older patients. Ultimately, we were unable to find a relationship between rates of appropriately and inappropriately placed contrast when looking at age, sex, and BMI. A larger study with more patients may provide sufficient power to detect statistically significant variables.
Conclusion
In this study, BMI, age, and sex were not statistically significant factors for determining those patients who were at risk for inappropriately placed contrast. Our results suggest that US-guided injections are safe and reliable and may serve as an effective technique in an office setting. A larger multicenter study will be needed to validate the recommendations of this study for the overall safety and accuracy of US-guided injections, particularly in the obese patient population (BMI >30 kg/m2). Nevertheless, this study supports the current literature that US-guided hip injections are safe and accurate alternatives to fluoroscopy-guided injections in an office setting.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Community Medical Centers, Fresno, California, USA (No. 2016032).