
Abstract
Background:
Recalcitrant lateral epicondylitis (LE) is a common debilitating condition, with numerous treatment options of varying success. An injection of platelet-rich plasma (PRP) has been shown to improve LE, although it is unclear whether the method of needling used in conjunction with a PRP injection is of clinical importance.
Purpose:
To determine whether percutaneous needle tenotomy is superior to percutaneous needle fenestration when each is combined with a PRP injection for the treatment of recalcitrant LE.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 93 patients with recalcitrant LE were treated with a PRP injection and percutaneous needle fenestration (n = 45) or percutaneous needle tenotomy (n = 48) over a 5-year study interval. Preoperative patient data, including visual analog scale for pain (VAS-P), Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH), and Patient-Rated Tennis Elbow Evaluation (PRTEE) scores and grip strength, were obtained from a chart review and compared with postoperative values obtained prospectively. Secondary outcomes included the incidence of complications, need for additional interventions, return to work, and patient satisfaction.
Results:
At a mean follow-up of 40 months, significant improvements in VAS-P (mean, –6.1; 95% CI, –6.8 to –5.5; P < .0001), QuickDASH (mean, –46; 95% CI, –52 to –40; P < .0001), and PRTEE (mean, –57; 95% CI, –64 to –50; P < .0001) scores and grip strength (mean, +6.1 kg; 95% CI, 4.9 to 7.3; P < .0001) were observed across the entire study cohort, with no significant differences noted between the fenestration and tenotomy groups. Nine of 45 patients (22%) underwent additional procedures to treat recurrent symptoms in the fenestration group compared with 5 of 48 patients (10%) in the tenotomy group (P = .05). No complications occurred in any patients, and no patients expressed dissatisfaction with their treatment course.
Conclusion:
A PRP injection with concomitant percutaneous needling is an effective treatment for recalcitrant LE, with sustained improvements in pain, strength, and function demonstrated at a mean follow-up of longer than 3 years. Although the method of concomitant needling does not appear to have a significant effect on treatment outcomes, more aggressive needle tenotomy is less likely to require conversion to open tenotomy than needle fenestration in the short term to midterm.
Keywords
Lateral epicondylitis (LE) is a commonly occurring condition that affects up to 3% of the adult population while accounting for significant costs related to medical care and lost wages. 14,30,43,53 Often referred to as tennis elbow, the underlying cause of LE involves noninflammatory processes of mucoid degeneration with neovascularization, scarring, and microtearing at the extensor origin at the lateral elbow, collectively termed angiofibroblastic hyperplasia or tendinosis. 1,39 As LE is considered to be self-limiting in the majority of patients, first-line treatment options generally focus on addressing the primary symptom of pain and may include oral and/or topical anti-inflammatory drugs and analgesics, bracing, stretching, and other physical therapy measures. 6,30,40,45 Although for most patients, pain resolves within 1 year of onset with nonoperative treatment alone, a smaller but significant population will continue to have persistent symptoms that are refractory to noninvasive treatment and will be deemed to have recalcitrant LE. 26
Patients with recalcitrant LE are particularly difficult to treat, as outcomes are generally suboptimal, while the most favorable treatment regimens continue to be debated. The least invasive options involve injections of corticosteroids, platelet-rich plasma (PRP), or other autologous derivatives, such as whole blood and tenocyte concentrate. 2,37,41,51,54 However, these treatments are not without complications of their own; this is particularly true for corticosteroids, which carry the risks of tendon atrophy and blood glucose spikes. 8,13,49 Furthermore, while most evidence suggests that PRP is superior to corticosteroids in the long term, the superiority of one over the other has still not reached consensus. 2,11,12,22,27,28,37,45 This is important, given the fact that corticosteroid and PRP injections are thought to act in opposing pathways, as corticosteroids are known inhibitors of inflammation, while animal models suggest that PRP induces a transient inflammatory response to stimulate a repair response. 23
Surgical treatment for recalcitrant LE, pioneered by Nirschl, included lateral release with debridement of the common extensor origin and has been shown to result in sustainable relief for over 1 decade. 10,16,17,39 Nirschl and Pettrone 39 suggested that the success of this procedure was secondary to the removal of diseased tissue, combined with bony decortication stimulating local blood flow. Since then, this concept has been modified to include arthroscopic and less invasive techniques, although the underlying method of tendon release or debridement has persisted. 3,16,29,47,50 Percutaneous tenotomy is favored by some, as it is reported to yield a lower severity and incidence of complications compared with open techniques. 4,31 –36,38,42,44,52
While positive outcomes after either a PRP injection or percutaneous needle tenotomy alone have been reported for the treatment of recalcitrant LE, to our knowledge, results after the two performed in conjunction have not been reported. Furthermore, it is not known if a PRP injection combined with more aggressive percutaneous needle tenotomy provides superior symptom relief than a PRP injection performed with a needle fenestration technique. Given the potential additive effects of PRP stimulating a repair response and decortication promoting increased blood flow, we hypothesized that a PRP injection performed in conjunction with needle tenotomy would result in superior outcomes compared with a PRP injection with needle fenestration. The purpose of this study was to determine if outcomes differed between patients with LE treated with a PRP injection plus percutaneous needle tenotomy and those treated with a PRP injection and percutaneous needle fenestration.
Methods
This study was approved by our institutional review board. We queried our departmental electronic database to identify patients who received a PRP injection with percutaneous needling for LE from January 2010 through December 2014 by 1 of 2 senior, fellowship-trained orthopaedic hand and upper extremity surgeons. Per their personal preferences, one surgeon (R.W.C.) performed needling with the fenestration technique, while the other (A.L.O.) performed needle tenotomy. Both surgeons utilized the following patient selection criteria: minimum symptom duration of 6 months, physical examination and magnetic resonance imaging (MRI) findings consistent with LE, and failed nonoperative management including all of the following: at least 1 prior corticosteroid injection, supervised therapy, and trial of splinting and/or counterforce bracing. Patients were excluded if they met any of the following criteria: open lateral epicondyle tenotomy, prior surgery or PRP injection for LE of the same elbow, corticosteroid injection within 3 months before the PRP injection, history of inflammatory arthropathy, or history of significant trauma about the elbow. For patients with bilateral LE treated with a PRP injection, only the first injection was included in the analysis.
Procedure and Postoperative Rehabilitation
All procedures were performed under sterile conditions in the operating room. Approximately 30 mL of venous blood was drawn from each patient and processed using the ACP Double Syringe System (Arthrex Inc) to obtain PRP for an injection. Anesthesia was typically administered either via axillary nerve blockade or local anesthesia with sedation. For both techniques, after the surface anatomy was mapped with a surgical pen, an 18-gauge needle was introduced through the skin overlying the common extensor tendon. The procedure in the fenestration group was performed in a similar fashion to previously reported studies (often referred to as “peppering”), whereby the needle was used to perforate the common extensor origin 5 times through the single skin entry site. 22,28,37,41 For the tenotomy group, after needle entry through the skin, the beveled edge of the needle tip was used to abrade the footprint of the common extensor tendon until a change in feedback was felt by the surgeon, after which PRP was then injected at the site. The change in feedback indicated a softening of tendinotic, diseased tendon with smoothening of bony irregularities. 33,34 After both techniques, the elbow was then ranged to rule out iatrogenic injuries to the lateral stabilizers, and a sterile dressing was placed on the elbow. Postoperatively, the patient was permitted to use the arm as tolerated. Rehabilitation protocols were identical between the groups and included range of motion exercises starting at 1 week and strengthening at 3 weeks.
Data Collection and Statistical Analysis
A retrospective chart review was performed to obtain patient demographic and disease-specific factors, including age, sex, handedness, medical comorbidities, work status, workers’ compensation status, duration of symptoms, and prior treatment. Examination findings included preoperative grip strength, tenderness over the common extensor origin (yes or no), and pain with resisted wrist extension (yes or no). Per our institution’s standard, documented grip strength was determined by the mean of 3 trials with the Jamar hand dynamometer (Sammons Preston Inc) on settings II and III for female and male patients, respectively. Preoperative visual analog scale for pain (VAS-P; 0 = no pain, 10 = worst pain imaginable) scores and Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) and Patient-Rated Tennis Elbow Evaluation (PRTEE) functional scores were also recorded. Patients were invited back to our center for a follow-up evaluation, which was performed by a study team member (M.P.G.) blinded to the original procedure. The follow-up evaluation included interval history taking; a repeat clinical examination; and postoperative VAS-P, QuickDASH, and PRTEE scores. Follow-up assessments of point tenderness and pain with resisted wrist extension were compared with preoperative findings using a custom Likert-type scale scored from 1 to 5 to maintain consistency with the format of the QuickDASH; in addition, patient satisfaction was assessed using a similar custom Likert-type scale (Table 1). Secondary data and qualitative outcomes that were recorded included patients’ preoperative and postoperative work status, incidence of complications, and need for additional interventions.
Custom Likert Scale to Assess Changes in Clinical Examination Findings and Final Patient Satisfaction With Treatment a

a Patients were asked to select the answer that best fit their self-assessment.
Univariate analysis was utilized to obtain descriptive statistics of the entire cohort, and bivariate analysis was performed with the Fisher exact and independent t tests to compare baseline preoperative patient demographics between the tenotomy and fenestration groups. Preoperative and postoperative values within each treatment group were compared using paired t testing, while improvements between the 2 groups were compared using independent t testing. All statistical analyses were performed using Minitab for Windows (version 17.3.1; Minitab Inc). An a priori power analysis was performed using the QuickDASH in a manner analogous to the use of the PRTEE reported by Krogh and colleagues. 28 We elected to use the QuickDASH for power analysis, given the previously established minimal clinically important difference (MCID) for the QuickDASH of 14 ± 14 reported by Sorensen et al 48 and a more recent similar MCID of 15.8 reported that specifically pertained to LE. 46 Thus, for a 2-sided significance level α = .05 to achieve 80% power (β = .8), a sample size of 17 patients in each group would be necessary to detect an effect size of 1.0.
Results
Ninety-three patients (50 female, 43 male) satisfied the inclusion criteria for this study. The mean age across the entire cohort was 51.7 ± 8.1 years. The mean interval from the onset of symptoms to the PRP injection was 26.8 ± 23.6 months (range, 6.2-127.8 months), while the mean follow-up interval was 39.7 ± 19.3 months (range, 12.2-80.8 months). All patients had preoperative MRI findings consistent with LE, tenderness to palpation over the common extensor origin, and pain with resisted wrist extension. Additionally, all patients had failed a trial of conservative management including physical therapy (including stretching, splinting, and/or bracing) and corticosteroid injection(s); the mean number of corticosteroid injections before the PRP injection was 1.54 ± 0.83. Overall, 45 and 48 patients comprised the fenestration and tenotomy groups, respectively. There was no difference in the baseline demographics between the study groups, as outlined in Table 2.
Comparison of Baseline Demographic Data Between the Groups a

a Values are shown as mean ± SD or n (%).
Outcomes
Postoperatively, mean grip strength (+6.1 kg; 95% CI, 4.9 to 7.3; P < .0001) and mean VAS-P (–6.1; 95% CI, –6.8 to –5.5; P < .0001), QuickDASH (–46; 95% CI, –52 to –40; P < .0001), and PRTEE (–57; 95% CI, –64 to –50; P < .0001) scores were significantly improved across the entire study cohort compared with preoperative values. Mean postoperative pain with resisted wrist extension and tenderness values across the cohort were 1.98 ± 0.84 and 1.75 ± 0.71, respectively. A comparison of outcomes between the fenestration and tenotomy groups is depicted in Table 3.
Comparison of Treatment Outcomes Between the Groups a
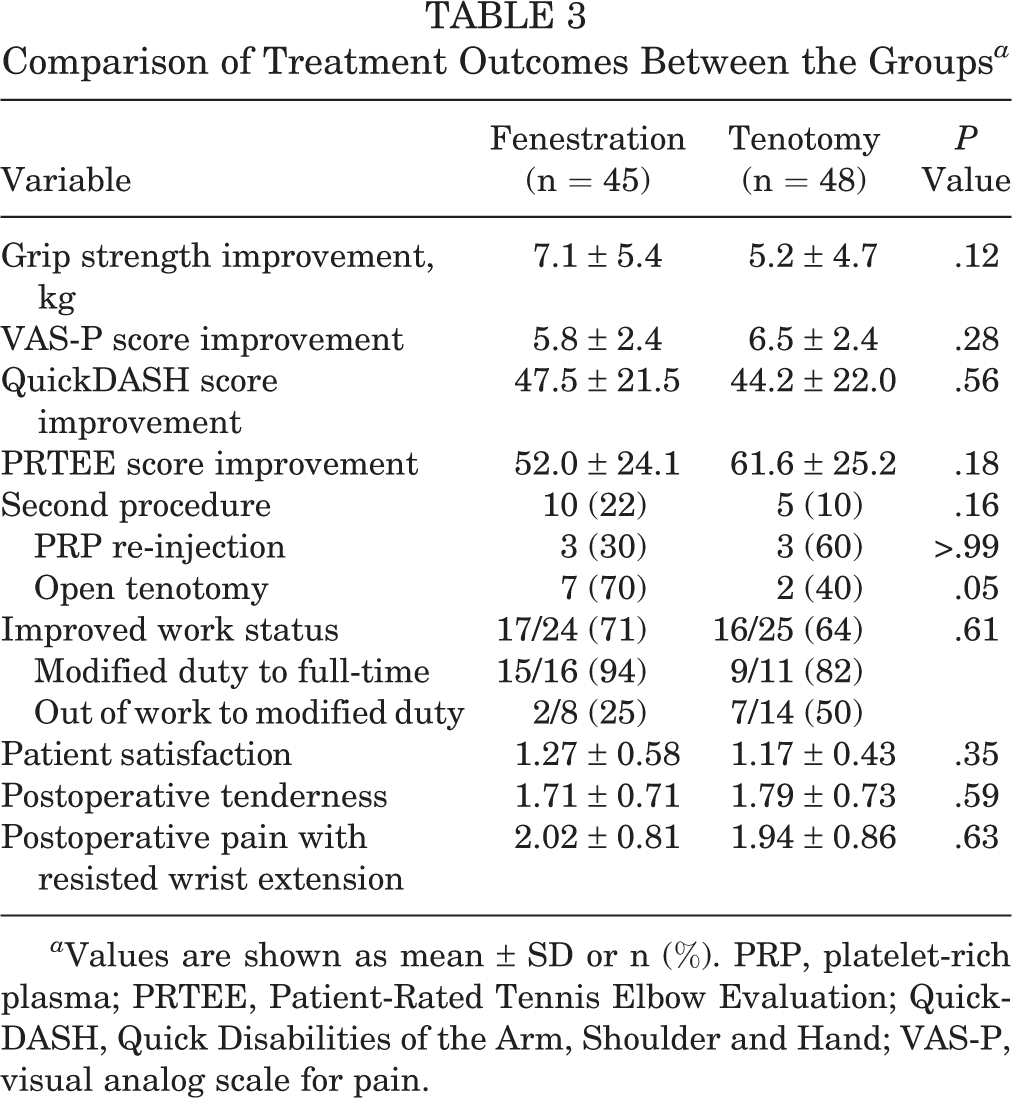
a Values are shown as mean ± SD or n (%). PRP, platelet-rich plasma; PRTEE, Patient-Rated Tennis Elbow Evaluation; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; VAS-P, visual analog scale for pain.
When comparing the final postoperative VAS-P score between the groups, the tenotomy group had a significantly lower VAS-P score than the fenestration group (Table 4), although the absolute preoperative versus postoperative difference was not significant (Table 3). Similarly, while the difference in final postoperative grip strength approached statistical significance (higher for the fenestration group), the preoperative versus postoperative difference between the groups was again nonsignificant. No other significant differences were found between the fenestration and tenotomy groups for any of the aforementioned variables (Tables 3 and 4).
Comparison of Preoperative and Postoperative Quantitative Outcomes Between the Groups a

a Data are shown as mean ± SD. PRTEE, Patient-Rated Tennis Elbow Evaluation; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; VAS-P, visual analog scale for pain.
Excluding those patients who were retired or already working full-time at the point of their initial procedure, 33 of 49 (67%) patients with preoperative work restrictions, that is, those either out of work or working a modified time/light duty, increased their work capacity by final follow-up. All 16 of those patients whose work capacity did not improve were workers’ compensation patients. No patients in either group were working in a lesser capacity than preoperatively. The mean satisfaction score across the full study cohort was 1.22 ± 0.51, with no patients scoring worse than 3.
Additional Procedures
Of the 93 patients, 14 (15%) underwent a second procedure. Three patients in each group received a second PRP injection for recurrent symptoms; 5 of those patients subsequently did well and required no further interventions. One patient who received a second PRP injection in the fenestration group had minimal symptom relief after the second injection and was subsequently converted to open tenotomy. Six additional patients in the fenestration group were converted to open tenotomy versus 2 patients in the tenotomy group (P = .05). The mean interval from the initial PRP injection to the second procedure was 9.7 ± 7.6 months (range, 2.6-30.1 months). No complications occurred in any patients.
Discussion
Despite a wealth of treatments available for patients with recalcitrant LE, an effective consensus or gold-standard option remains elusive. Nirschl and Pettrone 39 first reported histopathological findings confirming the condition to be a degenerative process rather than one of an inflammatory cause. In their series of 88 elbows treated with open debridement and repair at the common extensor origin, over 97% demonstrated improvement compared with preoperative symptoms. 39 Less invasive variations of the now-eponymous Nirschl procedure have since been described to include arthroscopic or percutaneous tenotomy and debridement of the common extensor origin, while repair of the tendon is no longer considered to be critical. ‖ Needle tenotomy in particular has been shown to yield positive outcomes, although comparative data relative to other options are lacking. 32 –34,55 Furthermore, we found that there was a substantial variability between studies as to the true definition of tenotomy, ranging from needle fenestration of the diseased tendon to debridement of the underlying bone. 18,32 –34,55 McShane and colleagues 33 reported on a prospective series of 58 patients treated with needle tenotomy under ultrasound guidance, which they described as “repeatedly fenestrat[ing] the tendinotic tendon,” followed by abrading the periosteum of the lateral epicondyle with the beveled needle edge, and finally, injecting a corticosteroid. In that report, 80% of patients reported excellent or good outcomes, although no objective measures or validated outcome instruments were used. 33 In a follow-up study by the same authors, 57 patients were treated in an identical fashion but without a corticosteroid injection, resulting in over 92% of patients with good or excellent outcomes. 34 In a similar study, Zhu et al 55 reported on 76 patients treated with ultrasound-guided needle “puncture” (without periosteal abrading), yielding 87% good or excellent outcomes. None of the 3 aforementioned studies included a comparison group or validated outcome measures.
As interest in more cost-efficient, nonsurgical methods has increased, definitive treatment with injectable therapies has also garnered more attention. ¶ PRP in particular has gained increasing popularity as an autologous therapeutic agent targeting a range of tendinopathies, including LE. 18,19 The exact mechanism by which PRP improves the symptoms of tendinopathy is still not entirely understood, although recent genomic work suggests that PRP incites a transient but substantial inflammatory process in fibroblasts within the diseased tendon, subsequently inducing signaling pathways involved in tendon regeneration. 23 This is supported by clinical reports demonstrating the positive effects of PRP to generally outlast those of corticosteroid injections. 2,22,28,41
Based on the potential individual benefits of tenotomy and PRP injections, we hypothesized that a PRP injection and percutaneous needle tenotomy would have an additive effect on outcomes, with superior results in patients with recalcitrant LE as compared with a PRP injection with the needle fenestration technique. We found that outcomes were largely similar between the groups, with the exception of final pain scores and grip strength. However, this difference was not observed when comparing the mean difference between the groups from preoperatively to postoperatively. Despite a potentially synergistic effect against recalcitrant LE, we found that needle tenotomy offered no significant additional benefit to needle fenestration regarding outcomes when both were combined with a PRP injection. We suspect that this is more reflective of a largely positive effect of the PRP injection rather than a marginal effect from tenotomy. From a pathophysiological standpoint, this may be explained by a large inflammatory effect of PRP, as described by Hudgens et al, 23 surpassing the combined mechanical effect of tenotomy on the degenerative tendon and its own mild incitation of inflammatory processes.
In addition to differences in symptomatic and functional outcomes, a key question that we aimed to answer was the relative complication and failure rates and the need for additional interventions. We found that the need for revision open tenotomy was significantly higher in the fenestration group than in the tenotomy group. One possible explanation for this difference is that the tenotomy procedure involves more aggressive abrading of tendinotic tissue than fenestration, with the latter process not adequately stimulate a repair response in the diseased tissue, thus allowing for symptoms to recur. Despite this difference, the overall revision rate of 15% across all patients lends further credence to the argument that a single PRP injection may serve as an alternative to surgery for the definitive treatment of recalcitrant LE. 20,21,24
This study is not without limitations, most notably the retrospective nature of preoperative data collection. This was especially likely to introduce bias with subjective assessments such as pain with resisted wrist extension or point tenderness. Although it would have been ideal to use the VAS-P or a Likert-type scale for these preoperative values, the lack of such details from clinical documentation precluded us from doing so. Thus, we elected to use the binary yes/no format and rely on our postoperative scales, which are of course subject to their own inherent recall bias. Another limitation is regarding the surgical technique itself. We did not use ultrasound for guidance to localize needle placement or for the evaluation of tendon quality postoperatively. This should be noted in light of recent findings by Keijsers et al, 25 who reported that the majority of injections were intra-articular rather than intratendinous. However, with the combined experience of the 2 senior authors (R.W.C., A.L.O.) who performed the procedure at more than 60 years in practice, we feel that this risk was likely minimal. Another noteworthy limitation was the absence of a true control group, such as a cohort treated with tenotomy and saline.
Despite these limitations, we feel that this study further supports the utility of PRP injections for the treatment of recalcitrant LE, with significant improvements observed in pain, function, and strength, for a mean duration of longer than 3 years and, in some patients, up to 6 years. Outcomes of a PRP injection combined with percutaneous needle tenotomy were not significantly different than those of a PRP injection and percutaneous needle fenestration, although more aggressive abrading with needle tenotomy resulted in a significantly lower rate of conversion to open tenotomy compared with needle fenestration. Future prospective randomized studies could further test this finding, and the addition of needle tenotomy and needle fenestration arms without a PRP injection would be warranted in such a study.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Thomas Jefferson University Institutional Review Board (study No. 15D.651).