
Abstract
Background:
Isokinetic strength testing is an important tool in the evaluation of the physical capacities of athletes as well as for decision making regarding return to sports after anterior cruciate ligament (ACL) reconstruction in both athletes and the lay population. However, isokinetic testing is time consuming and requires special testing equipment.
Hypothesis:
A single-jump test, regardless of leg dominance, may provide information regarding knee extension strength through the use of correlation analysis of jump height and peak torque of isokinetic muscle strength.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 169 patients who underwent ACL reconstruction were included in this study. Isokinetic testing was performed on the injured and noninjured legs. Additionally, a single-leg countermovement jump was performed to assess jump height using a jump accelerometer sensor. Extension strength values were used to assess the association between isokinetic muscle strength and jump height.
Results:
The sample consisted of 60 female (mean age, 20.8 ± 8.3 years; mean weight, 61.7 ± 6.5 kg; mean height, 167.7 ± 5.3 cm) and 109 male (mean age, 23.2 ± 7.7 years; mean weight, 74.6 ± 10.2 kg; mean height, 179.9 ± 6.9 cm) patients. Bivariate correlation analysis showed an association (r = 0.56, P < .001) between jump height and isokinetic extension strength on the noninvolved side as well as an association (r = 0.52, P < .001) for the involved side. Regression analysis showed that in addition to jump height (beta = 0.49, P < .001), sex (beta = –0.17, P = .008) and body mass index (beta = 0.37, P < .001) affected isokinetic strength. The final model explained 51.1% of the variance in isokinetic muscle strength, with jump height having the strongest impact (beta = 0.49, P < .001) and explaining 31.5% of the variance.
Conclusion:
Initial analysis showed a strong association between isokinetic strength and jump height. The study population encompassed various backgrounds, skill levels, and activity profiles, which might have affected the outcome. Even after controlling for age and sex, isokinetic strength was still moderately associated with jump height. Therefore, the jump technique and type of sport should be considered in future research.
A rupture of the anterior cruciate ligament (ACL) is one of the most common severe knee injuries in young and active patients. 12,36 A main challenge for the clinician during the rehabilitation period after ACL reconstruction (ACLR) is to decide when it is safe to return to competitive sports. 21 Several postoperative assessment methods, including laxity, strength, proprioception, and functional testing, exist to help make this decision. 1,15,17,30
Functional testing has become increasingly popular in the past decade 17,29,30 and is commonly used to predict an athlete’s ability to participate in sports. 17 To determine functional ability deficits in patients with ACL injuries, jumps for distance have been recommended. 21 In addition, the relationship between isokinetic testing and vertical jump tests has also been investigated. 21,35 However, even if athletes are cleared for unrestricted sports participation after ACLR, deficits in the performance of single-leg hop tests and quadriceps muscle strength are often present. 29 Quadriceps strength has always been considered an essential aspect of rehabilitation after ACLR, 20 and it is important to consider lower extremity muscle weakness and to implement strategies to improve lower extremity dynamic stability and strength within the rehabilitation protocol. 38
To detect these strength deficits, isokinetic dynamometry tests are commonly used to evaluate maximal force production after ACL injuries or ACLR. 30 Although it is unknown whether strength is a risk factor for an ACL graft rupture, quadriceps and hamstring strength contribute to successful return to sports. 20 Strength and power are important determinants of return to play in athletes, as strength deficits in knee extension and flexion lead to unnecessary stress on the ACL. 22,38,40 Therefore, isokinetic strength testing is an important aspect of the evaluation of the physical capacities in athletes, 7 as power depends heavily on maximal strength. 42 In addition, isokinetic testing is used in decision making regarding return to sports after ACLR 1,30 both in athletes and in the lay population. In this regard, a previous study found several relationships between leg extension power and jump test performance using a different testing device. 21 Although international knee experts stated more than 25 years ago that “adequate leg extension power” is a criterion for full weightbearing, 33 in a more recently published survey, only 41% of surgeons reported that strength tests contributed to their decision regarding an athlete’s return to sports. 34 The decreased use of this criterion may be because isokinetic testing is time consuming and demands special testing equipment; many clinicians do not have access to isokinetic testing equipment because of limited space and a limited budget. 21
It was hypothesized that a single-jump test, regardless of leg dominance, might provide information regarding knee extension strength through the use of correlation analysis of jump height and peak torque of isokinetic muscle strength. Therefore, the purpose of this study was to compare isokinetic leg extension muscle strength and jump height in patients after ACLR. An improved understanding of the usefulness of a single-jump test using a small testing device may provide additional information for clinicians to make return-to-play decisions if an isokinetic dynamometer is not available.
Methods
A total of 169 patients who underwent ACLR at an average of 6.6 ± 3.4 months postoperatively were included in this retrospective cohort study (Table 1). Patients completed at least 1 isokinetic strength test and 1 functional test using a specific test battery that consisted of 7 functional tests. Tests were performed between the years of 2011 and 2015, and the same investigator conducted all tests. Before testing, participants were examined by an orthopaedic surgeon and cleared for functional testing with a subjective evaluation and objective clinical examination to determine knee and psychological readiness for proper testing. The study was approved by the Ethics Commission of the Medical University of Innsbruck (AN2016-0067) and was conducted according to the Declaration of Helsinki 43 ; the study staff was trained in good clinical practice, and all patients granted written informed consent for participation.
Participant Demographics a

a Data are presented as mean ± SD. NS, not significant.
Isokinetic Testing
A standardized testing protocol was utilized for each patient. Patients were instructed regarding the use of the isokinetic testing machine and were allowed to become fully accustomed to the device before testing. Before testing, patients completed a 10-minute warm-up on a stationary bicycle, and if needed, they were allowed to perform individual dynamic stretching and jumping. The isokinetic testing protocol was based on the protocol described by Liebensteiner et al. 23 All tests were administered by the same researcher, who followed a standardized method for measuring peak extension and flexion torque using an isokinetic dynamometer (Con-Trex MJ; CMV AG). The testing protocol consisted of concentric quadriceps and hamstring contractions. 23 The patients started with the noninjured leg and performed 4 repetitions at an angular velocity of 60 deg/s. Angular velocity was automatically prescribed and controlled by the Con-Trex testing device software. After a 2-minute break, the same procedure was repeated for the injured leg. Peak extension torques of the uninjured leg were recorded and used for statistical analysis.
Functional Testing
The Back in Action (BIA) test battery (CoRehab) is designed for athletes in a healthy condition or in any phase of recovery after an injury. It measures balance, agility, speed, and dynamic strength with respect to normative data from a large group of healthy participants. The BIA indicator is an available option. The BIA test can be accomplished in 45 minutes and requires minimal equipment and a single room. It consists of the following subtests: (1) a 2-leg and (2) a 1-leg stability test, (3) 2-leg and (4) 1-leg countermovement jumps (with height and power calculations), (5) plyometric jumps, (6) speedy jumps, and (7) a quick feet test. 15,17 The single-leg countermovement jump was used to assess jump height, and values from both the injured and noninjured legs were included. Jump height and power calculations were recorded with a jump accelerometer sensor (CoRehab). The system has been shown to be accurate in the evaluation of the countermovement jump, reporting a mean error of 0.7 cm 26 compared with the Myotest system. 4,6
Statistical Analysis
All variables are displayed as descriptive data including the mean, SD, and proportion. Because of the sample size (>30) and based on the low values for skew and symmetry of the descriptive statistics, parametric tests were applied. 3 Values from the injured and noninjured legs were included to assess the association between isokinetic muscle strength and jump height calculated for the single-leg countermovement jump using Pearson correlation analyses. Further correlation analyses were performed to evaluate the possible influence of age, sex, and body mass index (BMI) on jump height and isokinetic knee extension strength. If these correlations were statistically significant, subsequent regression analyses were performed to control for confounding variables, and the predictive value for extension strength was estimated. Effect sizes were classified as <0.3 (weak), ≥0.3 to <0.5 (moderate), and ≥0.5 (strong), according to the guidelines of Cohen. 5 Stepwise linear regression analysis was conducted to analyze the predictive value of jump height on extension strength. In step 1, jump height was included; in step 2, age and sex were included; and BMI was included in step 3. Statistical significance was accepted for P ≤ .05. All statistical analyses were performed with SPSS Statistics for Windows (version 24.0; IBM Corp).
Results
Jump height and isokinetic extension strength values for the 169 participants are displayed in Table 2. For the noninvolved side, bivariate correlation analysis showed an association (r = 0.56, P < .001) between jump height and isokinetic leg extension strength. Further regression analysis showed that in addition to jump height (beta = 0.49, P < .001), sex (beta = –0.17, P = .008) and BMI (beta = 0.37, P < .001) also had an impact on isokinetic strength. The final model explained 51.1% of the variance in isokinetic muscle strength. Jump height had the strongest impact on isokinetic strength and explained 31.5% of the variance. Sex and age explained 9.0% of the variance, and BMI explained 11.7% of the variance. Age turned nonsignificant after including BMI in the last step (Table 3).
Jump Height and Isokinetic Extension Strength a
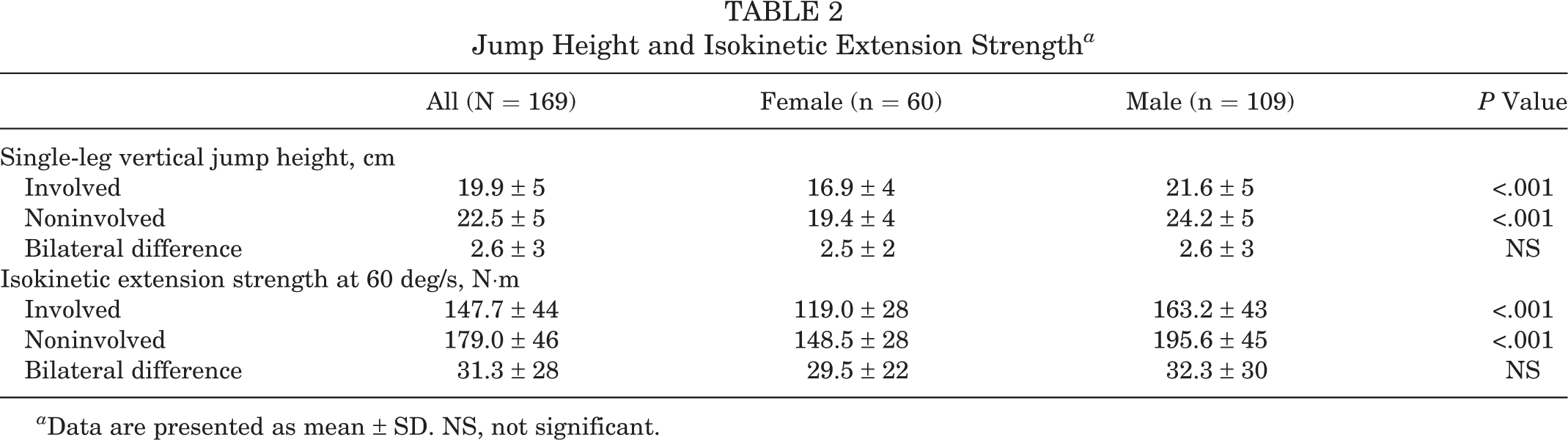
a Data are presented as mean ± SD. NS, not significant.
Results of Stepwise Linear Regression Analysis for Noninvolved Side a

a n = 167. NS, not significant; VIF, variance inflation factor.
b Corrected.
For the involved side, bivariate correlation analysis showed an association (r = 0.52, P < .001) between jump height and isokinetic extension strength. Further regression analysis showed that in addition to jump height (beta = 0.47, P < .001), sex (beta = –0.19, P = .007) and BMI (beta = 0.33, P < .001) also had an impact on isokinetic strength. The final model explained 44.0% of the variance in isokinetic muscle strength. Jump height had the strongest impact on isokinetic strength and explained 27.1% of the variance. Sex and BMI explained 8.7% and 9.1% of the variance, respectively (Table 4). Formulas to predict leg extension strength were produced from regression analyses for the involved and noninvolved sides (Table 5).
Results of Stepwise Linear Regression Analysis for Involved Side a
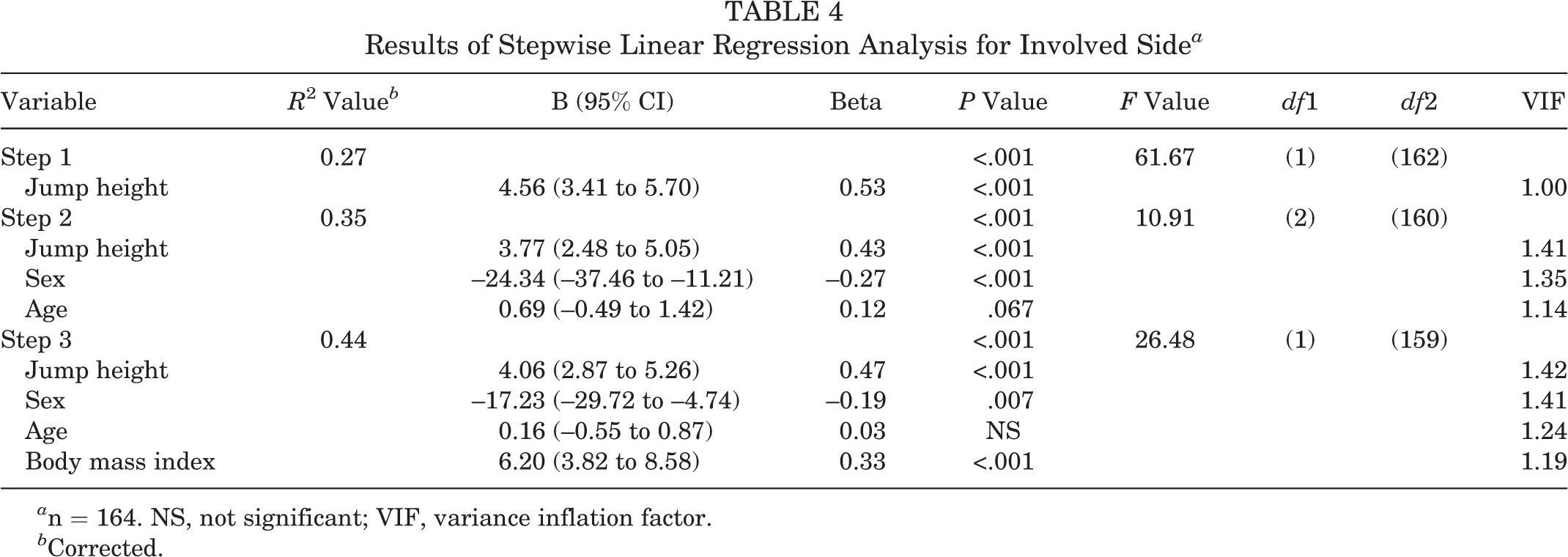
a n = 164. NS, not significant; VIF, variance inflation factor.
b Corrected.
Multiple Regression Equations for Leg Extension Strength a

a SE, standard error; X1, jump height; X2, sex (1 = male, 2 = female); X3, age; X4, body mass index.
b Corrected.
Discussion
The main finding from the initial analysis of this study was an association between isokinetic strength and jump height for the noninvolved (r = 0.56) and involved (r = 0.52) sides. After controlling for age, sex, and BMI, isokinetic strength was still found to be associated with jump height (beta = 0.49, P < .001). Using the produced regression formula and 95% CIs, clinicians without access to an isokinetic testing system can potentially use the jump test to estimate leg extension strength in patients after ACLR. Isokinetic strength and jump tests are common in the evaluation of physical capabilities to detect functional deficits among patients after ACLR. 1,30
Several studies have found decreased knee strength during various rehabilitation periods after ACLR. 9,25,39 Additionally, considerable variance in strength values around the time of return-to-play clearance has also been reported. 21 Further, greater bilateral strength differences were found in patients undergoing ACLR compared with a control group within the first year after surgery. 38 In a study by Hsiao et al, 18 injured knees showed a 25% to 30% decrease in quadriceps and hamstring strength, with normal patterns of length-tension and force-velocity relationships, within the first 6 months after surgery compared with the uninjured knee. The results of the present study show comparable outcomes in terms of leg extension strength within the first year after surgery, with an extension strength deficit of 17.5% in the involved leg compared with the noninvolved leg. These knee extension asymmetries have been shown to persist 6 to 9 months after surgery. 44 The literature suggests a side-to-side difference of less than 10% to 15% in muscle strength for patients returning to strenuous activities. 30 To achieve 90% of preinjury quadriceps and hamstring strength, as well as hopping performance after 2 years postoperatively, a combination of heavy-resistance strength training, plyometrics, and neuromuscular exercises is recommended. 12
To evaluate a patient’s functional status after ACLR, jump characteristics are often assessed using either a hop test for distance 2,31 or vertical jump performance. 21,28,35 Lower jump heights on the involved side compared with the noninvolved side have been reported in a single 1-leg jump. 21,35 The results of the current study support these findings, showing a decreased jump height of 11.6% for the involved side compared with the contralateral side. The risk of injuries may be increased with persisting side-to-side differences; therefore, jump height should be considered when evaluating an athlete’s return to play. 28
Isokinetic testing and jump height have been found to be beneficial in the evaluation of a patient’s rehabilitation progress after ACLR. 8,21,28 However, some clinicians may not have access to an isokinetic testing device. 21 Significant correlations between isokinetic knee extension strength and a single-leg jump test for distance 11 as well as for height 32 have been found in asymptomatic patients. In patients with ACL injuries, positive correlations between knee strength and hop for distance, timed hop, crossover triple hop, 41 and various jump tests for height 21 have been reported. The results of the current study show a similar relationship among the involved and contralateral legs in a single 1-leg jump for patients who underwent ACLR. Based on the relationship between results from jump tests and isokinetic knee-strength testing, 11 assessing jump height with a jump sensor might be an alternative choice, albeit used with caution, when clinicians do not have access to an isokinetic testing system. However, the results of this study show that sex and BMI must be considered, as they confound the association between jump height and isokinetic extension strength and explain 20.7% and 17.8% of the variance in the noninvolved and involved sides, respectively. It has been concluded from the results of previous studies that other aspects, such as the patient’s training level and age, 24 differences in muscle activation and knee joint power development, 19 and coordinative aspects, 37 should be considered when comparing isokinetic peak torques and jumping performance. 10 Finally, jump height can provide only a first indicator of strength, as 48.9% and 56.0% of variance in the noninvolved and involved sides, respectively, remain unexplained.
This study does have some limitations. Specifically, no record of sports participation and preferred jumping leg was considered; however, a previous study revealed that the uninvolved leg, regardless of dominance, can serve as a control when using dynamometric measurements in patients after knee ligament reconstruction. 35 The evaluation of the involved side requires critical consideration because the patients usually have been injured for some time and therefore probably have less than normal strength. 14 Testing the noninjured leg first may have led to altered results. A more sensitive classification of patients, such as <6 months, 6 to 9 months, and >9 months after the injury, might be considered; however, a previous study showed no association between time from surgery and functional deficits in athletes after ACLR. 28 The various backgrounds in terms of the skill level and activity profile of the study population might have influenced the outcomes. 10 Therefore, the jump technique and type of sport should be considered in future research.
Clinically, adequate quadriceps strength is desirable, as more symmetrical quadriceps strength before return to play has been shown to substantially reduce the reinjury rate. 13 Decreased relative hamstring strength combined with high relative quadriceps strength may be a risk factor for ACL ruptures. 16,27 To detect symmetrical quadriceps strength, a side-to-side comparison of the involved and uninvolved sides is possible with a single-leg jump test.
Conclusion
Isokinetic muscle strength testing is a useful practice for the evaluation of recovery progression and can be employed in the determination of return to sports. For clinicians without access to an isokinetic testing system, assessing jump height with a test battery is an inexpensive and easy-to-use tool that may be utilized to estimate leg extension strength in patients after ACLR. The formula produced from this study to describe extension muscle strength may serve as a framework for future studies to implement and improve the model in order to simplify the evaluation process for clinicians regarding return to sports after ACLR.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Institutional support for this research was provided by CoRehab.
Ethical approval for this study was obtained from the Ethics Commission of the Medical University of Innsbruck (AN2016-0067).
Acknowledgment
The authors thank all of the study participants for their efforts. Special thanks to Helmut Pointner for performing isokinetic and functional testing.