
Abstract
On October 15, 2016, experts met at Clínica CEMTRO in Madrid, Spain, under the patronage of the Spanish Society for Sports Traumatology (SETRADE), the Spanish Society of Sports Medicine (SEMED), the Spanish Association of Medical Services for Football Clubs (AEMEF), the Spanish Association of Medical Services for Basketball Clubs (AEMB), F.C. Barcelona, and Clínica CEMTRO. The purpose was to consider the most appropriate clinical management and treatment of tendinopathies in sports, based on proven scientific data described in the medical literature as well as on each expert’s experience. Prior to the meeting, each expert received a questionnaire regarding clinical management and treatment of tendinopathies in sports. The present consensus document summarizes the answers to the questionnaire and the resulting discussion and consensus regarding current concepts on tendinopathies in sports.
Tendon injuries are frequent in sports practice, accounting for between 20% and 30% of all sports injuries. Tendinopathy as a pathological episode may prevent any athlete from sports participation but has received relatively little research attention. Only recently has research interest arisen in the anatomic, biomechanical, and clinical structures involved in tendinopathy. Treatments have been based on doctors’ experience, and usual treatment approaches have entailed anti-inflammatory drugs, physical therapy, and surgery if conservative treatment was not sufficient. Knowledge regarding the tendon has been lacking in regard to basic science, anatomy, histology, and biochemistry. A tendon’s response to physical exercise and its ability to adapt were also previously unknown.
Advances in research on the causes and pathophysiological characteristics of tendinopathies have led to various medical concepts that explain features of tendinopathies and conditions in which they appear. Tendinopathy studies are currently guided by 2 main lines of work, led by Cook 8 –10 in Australia and Alfredson in Sweden, 1,2,4,5,21 both of which have established core concepts concerning physiopathology, clinical aspects, and treatment approaches. Nevertheless, treatment approaches among practitioners differ so much that any comparison is impossible; this, together with the absence of clearly defined concepts, constrains the ability to expand our knowledge regarding tendinopathies. Standard definitions and clearly described concepts are needed.
Thus, we set out to bring together experts in sports tendinopathy with the aim of establishing a precise definition for each pathological condition and reaching a consensus regarding clinical and therapeutic factors, in order to produce a document that can be used as a guide for everyday clinical practice.
Methods
Thirty experts in sports traumatology (university professors, orthopaedic surgeons, and/or sports physicians), all of whom were medical doctors with more than 15 years of experience in this specialty and were nationally recognized, participated in this project. Prior to the meeting, all participants received a questionnaire that contained 2 blocks of questions: a clinical management block and a treatment block (Appendix).
The questionnaire was prepared, revised, and completed by the experts themselves. All participants signed a conflict of interest declaration, and none received economic compensation of any kind from any of the companies that supported this event.
On October 15, 2016, the participants met at Clínica CEMTRO in Madrid, Spain, to discuss and reach a consensus for each of the included questions. Levels of consensus were described as unanimous (100%), highly recommended (75%-99%), recommended (55%-74%), and controversial (<55%).
Statistical Analysis
For analysis, participants were grouped as surgeons and nonsurgeons, with a third group including both. A descriptive analysis was carried out to assess categorical variables, expressing each as an absolute number or percentage. Percentages refer, in all cases, to participants.
Results
Clinical Management Block
Analysis of the clinical management block of the questionnaire resulted in the following findings.
Question 1, tendinopathy: 59% considered tendinopathy present when the tendon was painful and dysfunctional; 24% believed there was a tendinopathy when, additionally, further tests indicated structural disorders.
Question 2, tendinosis: 43% considered tendinosis present when the tendon was painful and dysfunctional and had structural disorders, whereas 46% considered that tendinosis was not present when there was proof of structural disorders, whether with pain or not.
Question 3, peritendinitis: 82% defined peritendinitis as a pathology presenting with pain and inflammation of peritendon and considered it a different concept than tendinosis and tendinopathy.
Question 4, acute tendinopathy: 85% considered 6 weeks as the maximum time since onset of symptoms for tendinopathy to be considered acute.
Question 5, chronic tendinopathy: 49% considered such a condition when symptoms persisted for more than 6 weeks after their onset, while 31% considered a condition to be chronic if symptoms persisted for more than 12 weeks.
Question 6, consideration of a possible partial tear: Participants agreed unanimously that an abrupt, snaplike, stabbing onset of pain was a possible indicator of a partial tendon tear that could later be confirmed by imaging.
Question 7, clinical signs of a peritendinitis: 97% agreed they would suspect peritendinitis when pinching the tendon, sliding it, and moving it were all continuously and constantly painful and, additionally, when the tendon showed inflammation, superficial pain, local warmth, redness, crepitation, and swelling.
Question 8, clinical signs of an intratendinous condition: 44% were suspicious of an intratendinous problem if pinching and sliding the tendon caused variation in pain; 38% believed there would also be swelling without inflammation.
Question 9, painless tendinous condition: 89% considered it to be a coincidental finding, 6% did not treat it, 69% followed it up, and 26% treated it.
Question 10, further tests: 96% of participants requested magnetic resonance imaging (MRI) and/or echography. Echography studies were the most requested imaging test, chosen by 38% of experts.
Question 11, the use of further tests to determine which treatment to apply: 43% found echography to be the most useful additional test, and 11% requested MRI. However, 46% considered either test just as useful.
Question 12, information considered relevant to decide on a treatment: 57% based their decision on echography and clinical findings and 26% based their treatment on clinical, echography, and MRI findings.
Question 13, information considered relevant under ideal conditions to decide on a treatment: 60% would base their decision on clinical, echography, and MRI findings and 31% would base such a decision on clinical and echography findings.
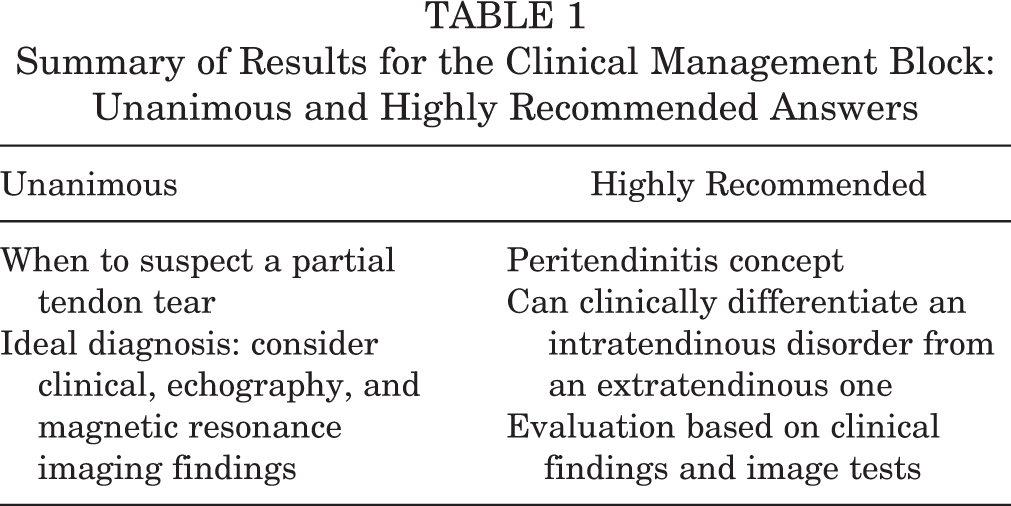
Question 14, the most appropriate definition for a pathological neovascularization detected by Doppler echography: 64% referred to it as a chronic tendinopathy and 22% thought a pathological condition was present if there was an increase in vascularization (Table 1).
Summary of Results for the Clinical Management Block: Unanimous and Highly Recommended Answers
Treatment Block
Analysis of the treatment block of the questionnaire resulted in the following findings.
Question 1: 39% treat pain-free tendinous disorders with preventive measures to correct any predisposing factors, and 26% follow them up; 32% also consider MRI and echography findings.
Question 2: 29% treat acute tendinopathies with measures adapted to the biological stage of the repair process, 26% use conservative measures, and 10% allow the condition to evolve naturally without treating it, simply indicating pain-free exercises.
Question 3: 69% agree on correcting the cause, predisposing factors, and pathological lesions found in echography and MRI.
Question 4: 32% apply physical therapy protocols and long-term strengthening programs (3-4 months) to tendinous neovascularizations, 14% perform infiltrations with sclerosing factors, 11% use high-volume washing procedures, and 14% use surgical or needle percutaneous tenolysis.
Question 5: 31% agree that chronic degenerative intratendinous origins that do not respond to conservative treatment should be treated with percutaneous needle tenotomy under echography control, 19% believe they should be treated with surgical scarifications, and 10% believe they should be treated with shock waves.
Question 6: 22% treat peritendinitis mainly with infiltrations, 19% use topical treatments and manual therapy, and 17% use active physical therapy.
Question 7: 37% would treat full-length diffused tendinopathy with active physical therapy (therapeutic exercises), 21% would use topical treatments and manual therapy, and 9% would consider surgery indicated.
Question 8: 36% would apply active physical therapy to insertion tendinopathies, 22% would use a topical treatment with manual therapy, and 21% would apply shock waves.
Question 9: 87% would consider surgery to be indicated in injuries that cannot be treated conservatively or do not respond to conservative treatment after 24 weeks; in injuries that entail partial tendon ruptures that affect more than 25% of the tendon diameter; in total tendon ruptures with functional insufficiency; and when conservative treatment does not allow athletes to return to play.
Question 10: 96% would use orthobiologic products (eg, enzymes, inflammation regulators, collagen) to treat acute and chronic tendinopathies, to treat peritendinitis, and as additional treatment in conjunction with invasive or surgical treatments.
Question 11: 28% would use platelet-rich plasma (PRP) to treat chronic tendinopathies, 23% would use it as additional treatment in conjunction with invasive or surgical treatments, and 19% do not believe it should be used.
Question 12: During the preseason, 31% perform biomechanical studies, analytical metabolic studies, specific strengthening programs, and preventive physical therapy, all according to individual needs; 50% would also apply further measures.
Question 13: During the season, 32% apply physical therapy techniques combined with other methods, 23% use physical therapy techniques only, and 14% use eccentric tendon exercises.
Question 14: 20% use the disappearance of pain as an exclusive return-to-play criterion; 39% use functional criteria such as mobility and pain-free strength; and 17% use a combination of disappearance of pain, normalization of structures as seen in echography imaging, time criteria (elapsed time from injury onset to moment of decision), and other functional criteria previously mentioned (Table 2).
Summary of Results for the Treatment Block: Unanimous and Highly Recommended Answers

Discussion
Clinical Management Block
The first concepts to be debated during the consensus session were definitions for the different types of tendinopathies, aspects that have been under continuous evolution since the 1990s. 17,22 This first step is essential, since it allows us to identify pathological entities on which to base therapeutic indications and so compare results for different treatments. Both surgeons and nonsurgeons consider a tendinopathy to be present when the affected tendon is painful and dysfunctional, with or without loss of muscular strength. We did not consider overload as a cause of injury, as other authors have, 20,23 or biochemical findings. 3
The term tendinosis refers to any tendinopathy showing structural alterations, with or without pain, thus requiring imaging studies such as echography, 6 sonoelastography, 16 or MRI. 19 The diagnosis of tendinosis is thus an issue in everyday practice because of the need for an imaging test. In contrast to tendinosis, peritendinitis has been defined as a condition that is diagnosed by the presence of inflammation and pain at the peritendon, regardless of other symptoms such as crepitation 11 or calcareous deposits. 18 Definitions of acute and chronic tendinopathy were also discussed, the consensus being that pain lasting 4 weeks indicates an acute tendinopathy and pain lasting more than 6 weeks indicates a chronic tendinopathy.
Participants said that if an athlete reported having felt a snap with an abrupt onset of pain while practicing sport, they would consider it a partial tendon rupture and would try to confirm with a specific imaging test (echography or MRI). It was also generally accepted that availability of such means of diagnosis would depend on the exact injury, the location of the injured tendon, and the clinician’s place of work (eg, hospital, sports club). 12,14,16,19
Participants discussed difficulties in diagnosing an intratendinous condition (tendinopathy) especially when differentiating the diagnosis of an extratendinous condition (peritendinitis), due to the specific anatomic features and locations of some tendons that do not allow for certain tests to be performed. Such circumstances force physicians to rely on clinical signs such as surface pain, local warmth, or redness of the affected area.
Opinions differ regarding tendinous disorders in pain-free athletes, 7,13,15 and such disorders are often asymptomatic coincidental findings that physicians come across during their exploration. Expert experience shows that when symptom-free conditions that do not hinder athletes’ performance are treated, the treatment itself can actually diminish athletes’ performance, perhaps due to psychological factors. Current consensus thus indicates that such findings should not be treated but should be followed up.
Recommendations for additional tests will depend on the athlete’s situation (eg, sports club, competition) at the time of injury, the quality of technical equipment available, and the experience of the physician reviewing the images, especially considering that some imaging results (such as echography) are operator-dependent and may influence the diagnosis.
Experts refer to clinical symptoms and physical examination of the athlete, together with echography findings (if available), as the most useful way of diagnosing the condition and obtaining information upon which to base treatment. However, under ideal conditions, MRI complemented with ultrasonography is considered the best way to precisely diagnose a tendinopathy. Doppler echography is used to verify pathological neovascularization when chronic tendinopathies are detected, which does not correspond to a revascularization in a tendon’s normal healing stages.
Experts are far from reaching a consensus on the use of diagnostic imaging in painful tendinopathies, for rehabilitation monitoring, or to assess treatment response.
Treatment Block
When assisting a patient with a pain-free tendinous disorder, many experts consider it useful to correct predisposing factors, yet there are differences between surgeons and nonsurgeons: Surgeons prefer to simply follow up, while nonsurgeons apply preventive measures for predisposing factors. Experts strongly recommended that imaging studies be used to identify predisposing factors, although opinion differed between surgeons and nonsurgeons with regard to the athlete’s and physician’s available resources at their training/work sites.
Regarding acute tendinopathies, participants achieved consensus that treatment should depend on the biological repair stage of the tendon. There is no one-size-fits-all standard treatment, as can be seen from Table 3.
Frequency Distribution for Recommended Treatments of Acute Tendinopathies a

a Values are expressed as percentages.
In chronic tendinopathies, experts recommended addressing the cause of the tendinopathy, with emphasis on predisposing factors. Additionally, possible treatments for injuries found on MRI and echography should always be kept in mind.
Chronic tendinous neovascularizations should always be treated, and chronic tendinopathies should be treated depending on the location of the affected tendon. No consensus was reached as to the most appropriate treatment (Table 4).
Frequency Distribution for Indicated Treatments of Neovascularizations a

a Values are expressed as percentages.
There was no consensus on how to treat degenerative intratendinous origins, although discussions indicated that such treatment should include percutaneous needle tenotomies under echographic control, and open surgery should be considered in certain cases.
It is difficult to decide on a treatment for peritendinitis, because it is essential to first distinguish it from a tenosynovitis. Infiltration is the preferred treatment for peritendinitis. Conservative treatment should be applied within the first 2 weeks after minor injuries.
In diffused tendinopathies that affect the entire tendon length, active physical therapy with therapeutic exercises is recommended. Insertional tendinopathies will likewise be treated with therapeutic exercises, surgery not being generally indicated.
Surgery is the preferred treatment in tendinopathies that are resilient to conservative treatment of more than 24 weeks, in partial tears that affect more than 25% of the total tendon diameter, in total tendon tears with functional alterations, and in any other tendinopathy that prevents the athlete from playing, despite conservative treatment.
Orthobiologic products are strictly linked to the biological stage of the tendinopathy at the moment of application and may be used as a complement to applied treatments.
Use of PRP still presents many uncertainties. The health care community must carefully examine any scientific evidence as well as all literature mentioning such treatments. If PRP is used, it must always be given via peritendinous administration and never intratendinous due to the risk of secondary tendon tear.
In preseason stages, it is advisable for all athletes to undergo biomechanical studies and metabolic analysis. They should also perform preventive strength conditioning programs in combination with relative rest periods.
Once athletes are in season, or during maximum load periods, experts strongly recommended isometric, concentric, and plyometric exercises and physical therapy techniques (cryotherapy, massage, use of straps).
When advising athletes on return to play, experts consider individually based objective criteria concerning pain and exercise tolerance.
In summary, the participants had a higher degree of consensus when defining pathological entities from the clinical management block. A certain degree of controversy was found in the treatment block since there is no golden, one-size-fits-all therapeutic approach. Furthermore, depending on the availability of diagnostic tests and the conditions under which athletes train and compete, certain treatments are more likely to be therapeutically indicated. Last, surgeons’ and nonsurgeons’ points of view varied regarding all of the above.
Further studies and consensus sessions are necessary in translational medicine, with the aim of adapting treatments to each tendon pathology.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by Bioiberica, Diafarm, and Heel and was produced in conjunction with the following organizations and institutions: the Spanish Society for Sports Traumatology (SETRADE), the Spanish Society of Sports Medicine (SEMED), the Spanish Association of Medical Services for Football Clubs (AEMEF), the Spanish Association of Medical Services for Basketball Clubs (AEMB), F.C. Barcelona, and Clínica CEMTRO.
Acknowledgments
The authors thank Mario Wensell for his inestimable assistance in translating this document and BSJ Technical Assistance for their straightforwardness and transparency in keeping both the meeting and the follow-up interest-free. Collaborators for this document were Rodolfo Peña, Assistant Physician at Orthopaedic Surgery and Trauma Ward; Dr Jose Peña Hospital, Ciudad de Bahia Blanca, Argentina; and Juan Manuel Lopez Alcorocho, Biomedical Research Unit, Clínica CEMTRO, Madrid, Spain.
Appendix Tendinopathy Questionnaire a

|
|
|
| 1. Do you believe tendinopathy is present when a. There is both tendon pain and dysfunction? b. It is exclusively associated with tendon pain? c. It is exclusively associated with dysfunction? d. Option a is present with structural disorders? e. Option a is present with no structural disorders? f. Just structural disorders are present, with or without pain? g. Other combinations (specify) |
3. Do you believe peritendinitis is present when a. There is inflammation of the peritendon? b. The peritendon is painful? c. Peritendinitis is a different concept than tendinosis. d. Peritendinitis is a different concept than tendinopathies. e. All of the above. f. None of the above. g. Other combinations (specify). |
| 2. Do you believe tendinosis is present when a. There is both tendon pain and dysfunction? b. It is exclusively associated with tendon pain? c. It is exclusively associated with dysfunction? d. Option a is present with structural disorders? e. Option a is present with no structural disorders? f. Just structural disorders are present, with or without pain? g. Other combinations (specify) |
4. From the onset of pain, how long would a tendinopathy need to last to be considered acute? a. 2 more weeks b. 6 more weeks c. 12 more weeks d. 24 more weeks |
| 5. From the onset of pain, how long would a tendinopathy need to last to be considered chronic? a. 2 more weeks b. 6 more weeks c. 12 more weeks d. 24 more weeks |
11. Which further tests do you consider most useful in order to decide which treatment to apply? a. Radiography b. MRI c. Echography d. Blood tests e. b and c f. Other |
| 6. If pain appears suddenly, with a snap or a stab, would you consider it a possible partial tear? a. I would b. I would not c. I would, if I can confirm with imaging |
12. In your daily clinical practice, in order to decide on a treatment, which data do you consider relevant? a. Clinical: onset history, exploration b. MRI findings c. Echography findings d. a and b e. a and c f. b and c g. a, b, and c |
| 7. Which clinical signs would make you consider a peritendinitis? a. Pinching and sliding maneuver causes constant pain b. There is inflammation: superficial pain, warm to the touch, redness, crepitation, and swelling c. a and b d. None of the above |
13. Under ideal conditions, in order to decide on a treatment, which data would you consider relevant? a. Clinical: onset history, exploration b. MRI findings c. Echography findings d. a and b e. a and c f. b and c g. a, b, and c |
| 8. Which clinical signs would make you suspect an intratendinous condition? a. Pinching and sliding maneuver causes pain to increase and decrease b. Inflammation-free swelling: superficial pain, warmth, redness, and crepitation c. a and b d. Neither a nor b |
14. Which do you consider the most appropriate definition for a pathological neovascularization detected by Doppler echography? a. Hypervascularization in a chronic tendinopathy. b. Hypervascularization in an acute tendinopathy. c. Any kind of increase in vascularization. d. Hypervascularization after an injury. |
| 9. Regarding painless tendinous conditions, how do you address such findings? a. I consider it a causal finding and apply no treatment. b. I consider it a causal finding and follow it up. c. I consider it a causal finding and treat it. d. I neither consider it nor treat it. |
|
| 10. Which additional tests do you usually request? |
|
|
|
|
| 1. When I encounter a pain-free tendinous disorder, I address it |
3. Treatments for chronic tendinopathy should correct |
| 2. I treat acute tendinopathies with |
4. What kind of direct approach do you think tendinous neovascularizations should be treated with? |
| 5. What kind of direct approach should be used for chronic degenerative intratendinous origins when they do not respond to conservative treatment? |
10. When is the use of orthobiologic products (enzymes, inflammation modulators, collagen) indicated? |
| 6. How do you believe peritendinitis should be treated? |
11. Which are current indications for the use of platelet-rich plasma (PRP)? |
| 7. How should a diffused tendinopathy be treated when the whole tendon length is affected? |
12. Which preventive measures do you apply during the preseason? |
| 8. How should insertion tendinopathies be treated? |
13. Which preventive measures do you apply during the season? |
| 9. When are surgical procedures indicated? |
14. Which criteria do you follow when considering return to play? |
a MRI, magnetic resonance imaging.