
Abstract
Background:
Subcoracoid impingement has been implicated as a cause of anterior shoulder pain and subscapularis tendon tears.
Purpose/Hypothesis:
The purpose of this study was to evaluate the bony anatomy of the coracoid process and the subcoracoid space. We hypothesized that age-related changes that may contribute to subcoracoid impingement occur in the subcoracoid space.
Study Design:
Descriptive laboratory study.
Methods:
In total, 418 skeletal shoulder specimens were included in this study. We utilized 214 shoulders from a young cohort (25-35 years of age) and 204 shoulders from an older cohort (>55 years of age) for comparison. We evaluated several morphological characteristics of the coracoid process and the subcoracoid space: coracoid width, coracoid shape, coracoid thickness, and subcoracoid distance. Each coracoid was observed for the presence of spurring or other morphological changes.
Results:
The mean anteroposterior (AP) thickness of the coracoid tip was 7.9 and 9.4 mm in our young female and male cohorts, respectively, while the mean AP thickness was 8.1 and 9.7 mm in our older female and male cohorts, respectively. The coracoid tip was hooked in 31 of 108 young female shoulders compared with 55 of 102 older female shoulders, and the coracoid tip was hooked in 25 of 106 young male shoulders compared with 45 of 102 older male shoulders. The mean subcoracoid distance in neutral rotation was 14.8 and 12.5 mm in young and older female shoulders, respectively, while the mean subcoracoid distance in internal rotation in these same cohorts was 8.7 and 7.0 mm, respectively. The mean subcoracoid distance in neutral rotation was 14.8 and 13.3 mm in young and older male shoulders, respectively, while the mean subcoracoid distance in internal rotation was 8.6 and 8.1 mm in young and older male shoulders, respectively.
Conclusion:
The principal findings of our study demonstrate that anatomic changes implicated in subcoracoid impingement may be developmental and worsen with age. The subcoracoid space was narrower in our older cohort of shoulders. Additionally, these older shoulders also had a greater AP width and a more hooked coracoid compared with young shoulders.
Clinical Relevance:
Narrowing of the subcoracoid space has been shown to be implicated as a cause of anterior shoulder pain and subscapularis tendon tears. This is the first study to show that the morphological changes implicated in subcoracoid impingement become more prevalent with age. This may help to explain the increasing prevalence of subscapularis tendon tears in older patients. Furthermore, subcoracoid decompression may be seen as an option for older patients with anterior shoulder pain and subscapularis tendon tears.
Anterior shoulder pain can have many different causes. The true cause of this pain can be difficult to determine clinically. Subcoracoid impingement has been implicated as a rare cause of anterior shoulder pain and abnormalities. 1,7 -9,14,20,22 -24 Gerber et al 8 provided the first comprehensive description of subcoracoid impingement. These authors described the clinical syndrome of subcoracoid impingement and helped to delineate the anatomy of this entity using computed tomography. 8
Patients with anteromedial impingement typically present with dull pain in the anterior shoulder, which may radiate to the arm or forearm. Pain is often aggravated by forward flexion and internal rotation. Subcoracoid impingement pain is thought to be caused by impingement of the subscapularis and bursal structures between the coracoid and the lesser tuberosity. 15,16,23 In progressive diseases, subcoracoid impingement syndrome has also been associated with subscapularis tendon tears. 1,16,23 Richards et al 23 demonstrated a significantly narrowed coracohumeral distance in patients with subscapularis tendon tears compared to a control group of patients. Balke et al 1 have recently shown that the coracohumeral distance in patients with degenerative subscapularis tendon tears is significantly decreased when compared to patients with traumatic tears.
Several anatomic studies have delineated the anatomy of the subcoracoid space. 5,12 Bhatia et al 2 performed a large-scale anatomic study of 101 human scapulae and found significant differences in several anatomic parameters between male and female specimens. Ferreira Neto et al 5 confirmed these sex-based differences in the subcoracoid space. Specifically, there was a smaller distance between the coracoid apex and the lesser tuberosity in female specimens compared to male specimens. 5 Gumina et al 12 also characterized the shape of the coracoglenoid space in 204 scapulae. No study to date has demonstrated an association between age and the anatomy of the coracoid process and the subcoracoid space.
The purpose of the present study was to compare the anatomy of the subcoracoid space in a young cohort of shoulders versus an older cohort of shoulders. We hypothesized that age-related changes that may contribute to worsening subcoracoid impingement with advancing age occur in the subcoracoid space.
Methods
We examined 418 osseous shoulder specimens from the Hamann-Todd Osteological Collection at the Cleveland Museum of Natural History. With over 3000 complete human skeletons, the Hamann-Todd Osteological Collection is the largest collection of its kind in the Western Hemisphere. This collection is unique in that it contains a variety of demographic data for each individual skeleton, including age, race, sex, height, and weight at the time of death. We chose this collection to evaluate a large number of specimens to answer our research question. We evaluated 214 shoulders (humerus and scapula) from a young cohort of specimens (aged 25-35 years at the time of death) and an older cohort of 204 shoulder specimens (aged >55 years of age at the time of death). There were 108 female shoulders and 106 male shoulders in the young cohort. We selected 102 female shoulders and 102 male shoulders for inclusion in our older cohort. All of these specimens were paired right and left shoulders. We included all specimens fitting our age constraints and where both left and right humeri/scapulae were present. We excluded any specimens without matched contralateral extremities, outside of our age constraints, with visible osseous deformities (fracture, infection, etc), and with visible degenerative changes in our young cohort.
We carefully examined each coracoid to characterize any morphological differences. Specifically, we noted the shape of each coracoid. When we viewed superiorly, we noted whether the coracoid was flat or hooked and whether there were any osteophytes. In the flat coracoids, the axis of the coracoid was generally straight from base to tip (Figure 1A). In the hooked acromion, the axis of the coracoid deviated posteriorly a few centimeters lateral to the base of the coracoid (Figure 1B). The presence of an osteophyte was signified by a visible posterior spur near the tip of the acromion, which was more focal (Figure 1C).

(A) Flat acromion. (B) Hooked acromion. (C) Osteophyte at the tip of the coracoid (arrow).
Several measurements were obtained utilizing digital calipers (±0.02-mm instrumental error; Mitutoyo). We measured the thickness of the coracoid (Figure 2). Next, we measured the coracohumeral distance, which is the distance from the posterior surface of the coracoid to the lesser tuberosity (Figure 2).

Coracohumeral distance (white double arrow) and coracoid thickness (black double arrow).
We measured the subcoracoid distance with the arm in neutral rotation and with the arm in 35° of internal rotation as described in the study by Brunkhorst et al. 3 We measured the glenocoracoid distance from a line tangential to the coracoid tip to the surface of the glenoid (Figure 3). The proper orientation of the humeral head to the glenoid was set by concentrically reducing the humeral head in the glenoid without any anterior or posterior subluxation. To account for the lack of cartilage in these specimens, we placed modeling clay at the glenohumeral interface to simulate the glenohumeral cartilaginous joint space. Several authors have shown the glenohumeral articular joint space to be approximately 2 to 3 mm wide. 11,18,26

Glenocoracoid distance.
The body of the scapula was positioned in line with the digital camera in the coronal plane. Angular measurements were obtained from digital photographs of the scapulae. The axes were drawn, and measurements were obtained using ImageJ software (https://imagej.nih.gov/ij/). We measured the glenocoracoid angle in both the frontal and axial planes. For frontal-plane measurements of the glenocoracoid angle, we used a photograph perpendicular to the plane of the scapula. One leg of the angle was defined as a line perpendicular to the face of the glenoid. The second leg of the angle was determined by a line drawn coaxial to the coracoid tip (Figure 4A). For axial-plane measurements of the glenocoracoid angle, the first leg of the angle was created from a line perpendicular to the face of the glenoid. The second leg of the angle was created by a line coaxial with the coracoid tip (Figure 4B).

(A) Coronal glenocoracoid angle. (B) Axial glenocoracoid angle.
These angles can also be utilized as an indicator of subcoracoid impingement. Smaller angles would bring the coracoid closer to the humeral head, which is a potential risk factor for subcoracoid impingement.
Statistical Analysis
We utilized a nonpaired Student t test to compare our digital caliper measurements and angular measurements. A P value of <.05 was used for statistical significance. The chi-square statistic was used to compare descriptive data on coracoid morphology.
Results
The mean age of our young male and female cohorts was 31.5 and 29.9 years, respectively. The mean age of our older male and female cohorts was 69.3 and 68.3 years, respectively. The mean coracoid anteroposterior (AP) width was 7.86 mm in young female shoulders, 8.08 mm in older female shoulders, 9.41 mm in young male shoulders, and 9.67 mm in older male shoulders. The coracoid was hooked in 31 of 108 (28.7%) young female shoulders, 55 of 102 (53.9%) older female shoulders, 25 of 106 (23.6%) young male shoulders, and 45 of 102 (44.1%) older male shoulders. The mean subcoracoid distance (ie, subcoracoid space) with the arm in neutral rotation was 14.82 mm in young female shoulders, 12.48 mm in older female shoulders, 14.76 mm in young male shoulders, and 13.32 mm in older male shoulders. The mean subcoracoid distance with the arm in internal rotation was 8.65 mm in young female shoulders, 6.97 mm in older female shoulders, 8.63 mm in young male shoulders, and 8.13 mm in older male shoulders. The mean glenocoracoid distance was 8.26 mm in young female shoulders, 10.01 mm in older female shoulders, 8.21 mm in young male shoulders, and 9.99 mm in older male shoulders (Table 1).
Subcoracoid Morphology a
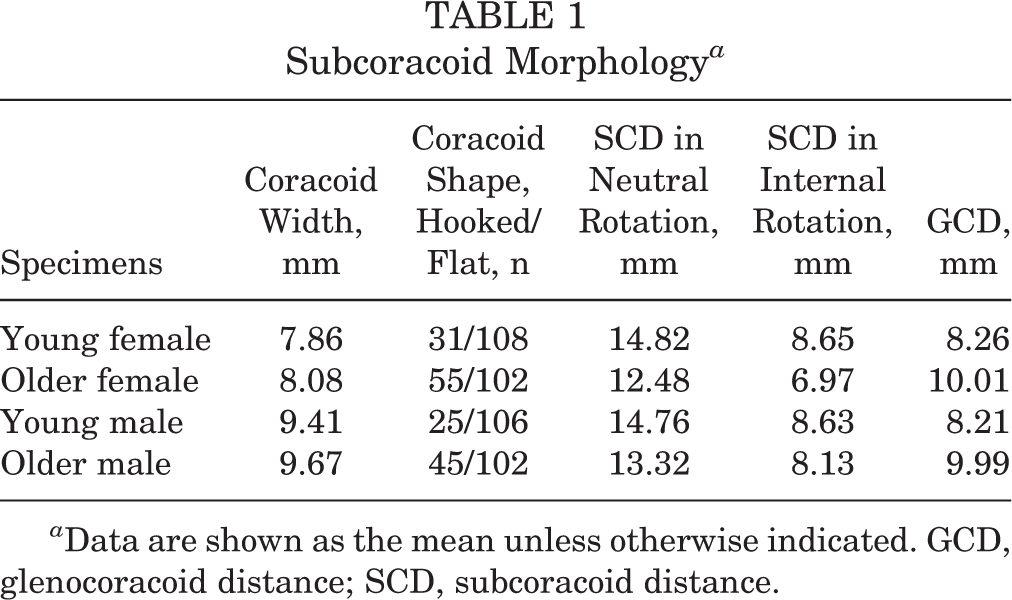
a Data are shown as the mean unless otherwise indicated. GCD, glenocoracoid distance; SCD, subcoracoid distance.
The mean frontal glenocoracoid angle was 31.4° in young female shoulders, 29.9° in older female shoulders, 34.6° in young male shoulders, and 32.0° in older male shoulders. The mean axial glenocoracoid angle was 44.5° in young female shoulders, 41.5° in older female shoulders, 43.9° in young male shoulders, and 44.0° in older male shoulders.
The AP width of the coracoid was not significantly different in young female shoulders compared to older female shoulders (P = .11) or in young male shoulders versus older male shoulders (P = .15). The difference in AP width of the coracoid was significant when comparing young female shoulders to young male shoulders (P < .0001) and older female shoulders to older male shoulders (P < .0001). The AP width of the coracoid was larger in male specimens compared to female specimens. The coronal glenocoracoid angle was significantly different in young male specimens versus older male specimens (P = .013), young female specimens versus young male specimens (P = .001), and older female specimens versus older male specimens (P = .03). The coronal glenocoracoid angle was not significantly different in young female specimens compared to older female specimens. The axial glenocoracoid angle was not significantly different in young male specimens versus older male specimens (P = .94), young female specimens versus young male specimens (P = .65), or older female specimens versus older male specimens (P = .05). The axial glenocoracoid angle was significantly different for young female specimens versus older female specimens (P = .02).
The difference in subcoracoid distance in neutral rotation was significant in young female specimens compared to older female specimens (P < .0001) and in young male specimens versus older male specimens (P = .01). The subcoracoid distance in neutral rotation was not significantly different in young female specimens versus young male specimens (P = .44) or in older female specimens versus older male specimens (P = .15). The subcoracoid distance in internal rotation was different in young female specimens versus older female specimens (P = .0001) and in older female specimens versus older male specimens (P = .007). The subcoracoid distance in internal rotation was not different in young male specimens versus older male specimens (P = .27) or in young female specimens versus older male specimens (P = .97). The glenocoracoid distance was significantly different in young female specimens versus older female specimens (P = .004) and in young male specimens versus older male specimens (P = .008). The glenocoracoid distance was not significantly different in young female specimens versus young male specimens (P = .91) or in older female specimens versus older male specimens (P = .97) (Table 2).
Comparative Subcoracoid Anatomy (P Values) a

a A P value <.05 was used for statistical significance. GCA, glenocoracoid angle; GCD, glenocoracoid distance; SCD, subcoracoid distance.
Coracoid morphology demonstrated a more hooked coracoid in older specimens compared to young specimens. In older specimens, 100 of 204 specimens demonstrated a hooked coracoid (49%), while in young specimens, 56 of 214 specimens had a hooked coracoid (26%). This difference was significant (P < .0001). In older female specimens, 55 of 102 coracoids were hooked (53.9%) compared to 31 of 108 (28.7%) in young female specimens. This difference also reached statistical significance (P = .016). Finally, young male specimens demonstrated a hooked acromion in 25 of 106 coracoids (23.6%) versus 45 of 102 coracoids (44.1%) in older male specimens (P = .0017).
Discussion
The principal finding of this study was that the anatomy of the coracoid process and the subcoracoid space differed among a young cohort of shoulders compared to that of an older cohort of shoulders. We also found that there were sex-based differences in the anatomy of the coracoid process and the subcoracoid space. The subcoracoid space was narrower in older shoulders. The coracoid was also more hooked in older specimens. These changes appeared to be more pronounced in female shoulders compared to male shoulders in both our young and older cohorts.
Subcoracoid impingement has been implicated as a potential cause of anterior shoulder pain. This clinical syndrome was first comprehensively described by Gerber et al. 8 These authors described subcoracoid impingement as symptomatic impingement of the rotator cuff between the coracoid process and the humerus. 8 These authors utilized computed tomography to define the constraints of the subcoracoid space. This limited space must accommodate the humeral head articular cartilage, joint capsule, subscapularis tendon, and its associated bursa while allowing gliding of these structures. Small changes in the subcoracoid space can have implications with respect to impingement of the subscapularis tendon and bursa. This impingement causes pain in the anterior shoulder that may be referred to the upper arm and forearm. 4,8,9 Provocative maneuvers include forward flexion of the arm with medial rotation. 4,6,8 Gerber et al 8 also noted that patient symptoms were relieved after decompressive surgery to increase the subcoracoid space. Several other authors have also described this clinical entity and proposed algorithms for treatment. 9,22
A thorough understanding of the anatomy of the subcoracoid space is essential to the management of this clinical entity. Several authors have described the anatomy of the subcoracoid space. 2,5,10,13 A key finding in subcoracoid impingement is a decrease in the subcoracoid space with the arm in internal rotation. 3,5 This has implications with respect to the diagnosis, symptom generation, and management of subcoracoid impingement. Brunkhorst et al 3 showed a significant decrease in the coracohumeral distance with internal rotation utilizing 3-dimensional biplane fluoroscopy. Our study successfully confirms this finding. In all cohorts, the subcoracoid space was significantly decreased in internal rotation. The magnitude of the decrease in coracohumeral distance in internal rotation may have clinical implications with respect to the development of subcoracoid impingement symptoms. Friedman et al 6 used cine magnetic resonance imaging to show that the subcoracoid distance is smaller in internally rotated shoulders with symptomatic subcoracoid impingement compared to asymptomatic shoulders. Furthermore, Park et al 21 found that patients diagnosed with subcoracoid impingement exhibited less shoulder internal rotation. All patients had increased internal rotation after coracoplasty surgery.
Another key finding outlined by several authors is sex-based differences in the anatomy of the subcoracoid space. 5,10,13 Specifically, the subacromial space has been shown to be narrower in women. Both Giaroli et al 10 and Hekimoglu et al 13 noted a smaller coracohumeral distance in women. In the study by Giaroli et al, 10 the smaller coracohumeral interval was not predictive of clinically diagnosed subcoracoid impingement syndrome. Conversely, Hekimoglu et al 13 did find a direct correlation with a narrowed coracohumeral index and symptoms of subcoracoid impingement. Our study did not show a significant difference in the subcoracoid distance in men versus women. We did, however, find a significant difference in the morphology of the coracoid process in women versus men. In our study, we found that hooked coracoids were more commonly seen in women. This trend has not previously been reported in the literature. Our findings also suggest that this morphological change in the coracoid may worsen over time, as a hooked acromion had a higher prevalence in our older cohort of male and female shoulders. The exact cause of the development of a hooked coracoid is unknown, but our study suggests that it may be partially a function of the aging process. This should be taken into account when evaluating anterior shoulder pain in older patients.
Our study is the first to compare the subcoracoid space in a young cohort of shoulders versus an older cohort of shoulders. We found significant differences in the subcoracoid distance between older specimens and young specimens. The subcoracoid distance was significantly narrowed in older specimens compared to young specimens. This difference was most pronounced when comparing young female shoulders to older female shoulders. The implications of a narrowed subcoracoid space have not been clearly defined, but these findings further support the notion that changes in the subcoracoid space may, in part, develop over time as opposed to being static throughout a lifetime. These concepts have also been supported clinically by several authors. Balke et al 1 have shown that degenerative tears were more common in women, supporting our findings that the magnitude of subcoracoid changes was greater in female specimens compared to male specimens. These authors also found that degenerative tears were more common in older patients. 1 Richards et al 23 noted that the coracohumeral distance was markedly decreased in the setting of subscapularis tendon tears. The average age of this patient cohort was 61.9 years. These findings also support the concept that progressive narrowing of the subcoracoid space over time may contribute to subscapularis tendon tears in older patients. 23
The implications of a narrowed coracohumeral space continue to be defined in the literature. Our knowledge of the pathogenesis and management of subcoracoid impingement continues to lag behind our knowledge of other conditions involving the shoulder. Despite our incomplete understanding of this clinical entity, several authors have published favorable outcomes relating to the treatment of subcoracoid impingement. 7,16,19,25 Lo et al 16 evaluated a small cohort of patients with combined subacromial impingement and subcoracoid impingement. In that series, all patients underwent subacromial decompression, subcoracoid decompression, and rotator cuff repair. 16 All patients did well after this combined procedure. 16 Suenaga et al 25 identified subcoracoid impingement symptoms in patients after prior rotator cuff surgery. All patients improved after subcoracoid impingement surgery. 25 These authors noted that subcoracoid impingement may be a cause of persistent symptoms after rotator cuff repair. 25 Interestingly, Misirlioglu et al 19 showed that arthroscopic subacromial decompression in patients with both subacromial and subcoracoid impingement resulted in improvement of the coracohumeral distance and resolution of both subacromial and subcoracoid impingement symptoms. Garofalo et al 7 performed several different surgical procedures in patients with subcoracoid impingement syndrome (4 men/9 women). In that series, 8 of 13 patients underwent coracoplasty either alone or combined with another procedure; and 5 patients underwent stabilization surgery without coracoplasty. 7 All patients with subcoracoid impingement symptoms were relieved with surgery, suggesting that subcoracoid impingement may have varied causes. 7 For example, MacMahon et al 17 suggested that there may be a dynamic component to subcoracoid impingement. These authors demonstrated that supraspinatus tears may lead to dynamic changes in the subcoracoid space. 17 They also showed that subcoracoid impingement changes were more prevalent with increasing size and retraction of supraspinatus tendon tears. 17
Our study has several limitations. The specimens utilized were devoid of soft tissue. Because of the lack of soft tissue, we cannot comment on the role of soft tissue thickness in the pathological process of subcoracoid impingement. Also, the lack of articular cartilage could change the normal in situ relationship between the glenoid and the humeral head. To account for this, we placed modeling clay into the glenohumeral articulation to simulate the average thickness of the glenohumeral joint articular cartilage. Because of the nature of this anatomic study, we could not evaluate dynamic impingement. Last, we did not normalize our data to anthropometric parameters (ie, height, weight, humerus size) or race.
In conclusion, our study demonstrates that the parameters of the subcoracoid space differ in men versus women and that the coracoid process and the subcoracoid space undergo several changes with increasing age. This is the first study to suggest that the anatomic findings of subcoracoid impingement worsen with increasing age. These findings may help surgeons gain a better understanding of the subcoracoid space and the cause of subcoracoid impingement syndrome. The findings may also help surgeons with the identification of at-risk patients and the management of this important clinical entity.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study.
Acknowledgment
The authors thank Lyman Jellema for his assistance with access to the Hamann-Todd Osteological Collection at the Cleveland Museum of Natural History.