
Abstract
Background:
The role of lateral extra-articular tenodesis (LEAT) to augment primary anterior cruciate ligament reconstruction (ACLR) remains controversial.
Purpose:
To determine whether the addition of LEAT to primary ACLR provides greater control of rotational laxity and improves clinical outcomes compared with ACLR alone and to assess the impact of early versus delayed ACLR.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
Two reviewers independently searched 7 databases for randomized and nonrandomized clinical studies comparing ACLR plus LEAT versus ACLR alone. Animal, cadaveric, and biomechanical studies; revision or repair procedures; and studies using synthetic ligaments and multiligamentous-injured knees were excluded. Risk of bias was assessed with a modified Downs and Black checklist. The primary outcome was postoperative pivot shift. These data were pooled by use of a fixed-effects meta-analysis model. The studies were divided into delayed (>12 months) and early (≤12 months) reconstruction groups for meta-analysis. A best-evidence synthesis was performed on the remaining outcome measures.
Results:
Of 387 titles identified, 11 articles were included (5 of high quality). Meta-analysis of postoperative pivot shift in 3 studies of delayed primary ACLR showed a statistically significant difference for the pivot-shift test in favor of ACLR with LEAT (odds ratio [OR], 0.44; 95% confidence interval [CI], 0.24-0.81; P = .008; I 2 = 0). Meta-analysis of 5 studies of early primary ACLR found no statistically significant difference with the addition of LEAT (OR, 0.60; 95% CI, 0.33-1.09; P = .10; I 2 = 33%). Insufficient evidence was available to determine whether the addition of LEAT had any effect on clinical, objective, subjective, and functional outcomes.
Conclusion:
In primary ACLR, no evidence is available showing additional benefit of LEAT in reducing the postoperative pivot shift in early reconstructions (≤12 months); however, LEAT may have a role in delayed ACLR. Strong evidence exists that a combined ACLR and LEAT reduces lateral femoral translation, but there is insufficient evidence to identify any benefit for other clinical outcomes.
Keywords
Interest in the concept of anterolateral rotatory instability of the knee has been renewed following recent descriptions of the anatomic features of the anterolateral ligament (ALL). 6,7,13,14,26 Hughston et al 24 postulated that this type of instability was caused by a tear of the middle one-third of the lateral capsular ligament but may be accentuated by other tears, principally rupture of the anterior cruciate ligament (ACL). Investigators have reported that anterolateral rotatory instability was most accurately demonstrated by the jerk test, a variation of the pivot-shift maneuver. 24,27 It has since been established that the lateral one-third of the lateral capsule and the ALL are continuous. 6
Surgeons have long recognized that extra-articular augmentation procedures offer a powerful tool to control rotation of the knee. 42 The concept of combining a lateral extra-articular augmentation with an intra-articular reconstruction for the treatment of ACL injury emerged with the objective of decreasing the failure rate of either technique carried out in isolation. 8,50,62 The approach became popular in the 1980s and was adopted by a number of surgeons using a variety of extra-articular augmentation procedures. 16,17 Although most of these procedures diminished or obliterated the pivot shift, extra-articular augmentation fell out of favor when reports emerged about its unpredictability and unsatisfactory results. 18,25,58 Biomechanical and clinical studies suggested that intra-articular reconstruction of the ACL alone would be sufficient in the treatment of knee instability following isolated ACL tear and that extra-articular procedures added little to the overall functional outcome. 1,2,37,38,51 As the incidence of ACL reconstruction (ACLR) has increased significantly over the past 2 decades, so too have the revision rates for this procedure, which now represent a significant surgical burden. 20,28,29,39,55,59 Consequently, interest has been renewed in lateral extra-articular tenodesis (LEAT) in combination with ACLR in the primary setting as a way of potentially reducing the rate of reinjury.
Two recent systematic reviews have been conducted on this topic. 21,48 Hewison et al 21 systematically reviewed all comparative studies to determine whether the addition of LEAT to ACLR would provide greater functional stability and improved clinical outcomes compared with ACLR alone. Although the results are comprehensive, the studies included were quite heterogeneous, consisting of multiple extra-articular reconstructions performed in combination, revision procedures, the use of synthetic ligaments, and nonconventional ACLR grafts. In the other systematic review, Song et al 48 included all levels of evidence and focused on the clinical outcomes of combined LEAT and intra-articular ACLR in both primary and revision ACLR addressing the high-grade pivot-shift phenomenon. While these reviews are helpful, they do not answer 2 key questions: Is there a role for LEAT in combination with intra-articular ACLR in primary ACL surgery? What impact does the interval from ACL injury to primary reconstruction have on the effectiveness of LEAT to control rotational stability?
The primary aim of this systematic review was to determine whether the addition of LEAT to a primary ACLR would result in improved rotational stability and clinical outcomes compared with ACLR in isolation. The secondary aim was to determine whether the time interval between injury and surgery influenced postoperative rotational stability.
Methods
This systematic review with meta-analysis followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 30
Search Strategy
Articles were identified via a search of the electronic databases MEDLINE, CINAHL, EMBASE, SPORTDiscus, the Cochrane Library, AusportMed, and PEDro. Database entries were searched from the earliest reported date (January 1950 for Medline) to April 2016. Search terms were mapped to relevant MeSH terms or subject headings where possible.
Search terms were entered into the database under 2 concepts: Concept 1—“anterolateral ligament,” “anterior oblique band,” “lateral capsular ligament,” “ALL,” “extra-articular,” “extraarticular procedure,” “lateral tenodesis,” “Segond,” “Lemaire,” “Losee,” “MacIntosh,” “Ellison,” “iliotibial band,” “knee,” “reconstruction”; Concept 2—“follow up,” “objective,” “subjective,” “patient reported outcome,” “clinical outcome.” Keywords in each concept were grouped with the “OR” operator. The results from each concept were then combined with the “AND” operator to produce the search strategy and the final yield. To supplement the electronic database search, the reference lists of relevant papers were cross-checked, and forward citation tracking via the Web of Science electronic database was conducted.
Publication details from all studies identified in the literature search were exported to bibliographic software.
Selection Criteria
The following inclusion criteria were applied to the final yield: Published peer-reviewed study: either randomized controlled trial (RCT) or case-control study (CCS) Outcome data presented following primary ACLR combined with LEAT procedure Minimum 2 years of follow-up
If a study included primary and revision ACL reconstruction with LEAT, it was only included if the number of primary ACL reconstructions accounted for more than 80% of the total cohort. In addition, only procedures performed on skeletally mature patients and reported in the English language were included. All criteria had to be satisfied for inclusion.
The exclusion criteria were as follows: Extra-articular procedure performed in isolation Synthetic graft used for ACLR or LEAT Cases with more than 2 surgically treated knee ligaments ACLR combined with alignment knee surgery ACL repair in conjunction with LEAT Reports on guidelines, technical notes, reviews, or systematic reviews
When the selection criteria were applied, the title and abstract of each study were initially reviewed. In the cases where it was not clear from the review of the title and abstract whether a study was appropriate for inclusion, the full text of the article was examined. Two reviewers applied the selection criteria independently (B.M.D. and S.W.B.). Consensus was used to resolve any disagreements between reviewers, and a third reviewer was consulted if consensus could not be reached. In the case of multiple reports on the same patient cohort with an increasing duration of follow-up, only the article with the longest follow-up was included.
Risk of Bias
The risk of bias of the included articles was independently assessed by 2 reviewers (B.M.D. and S.W.B.) using a modified version of the Downs and Black scale. 15 The Downs and Black scale is reliable for cohort and case-control study designs. 15 The modified version used in this study had a maximum score of 16, as previously reported; a score of ≥12 was defined as high quality, 10-11 as moderate quality, and ≤9 as low quality. 31,32 Any disagreements in initial ratings of methodological quality assessment were discussed until a consensus was reached between the 2 reviewers.
Data Extraction
Two independent reviewers extracted data using a data-extraction form specifically designed for this review. The primary outcome of interest was the assessment of rotational stability as measured by the pivot-shift test. The secondary outcomes were clinical, objective, subjective, functional, and radiographic outcomes. The descriptive data extracted are outlined in Table 1.
Summary of Extracted Data a

a ACLR, anterior cruciate ligament reconstruction; HSS, Hospital for Special Surgery; IKDC, International Knee Documentation Committee; LEAT, lateral extra-articular tenodesis; ROM, range of motion.
Data Synthesis and Analysis
A meta-analysis was performed when sufficient homogenous data were reported in the outcome measures. Data were analyzed by use of ReviewManager (RevMan, Version 5.3). A P value of less than .05 was considered statistically significant.
To address the primary aim, pivot-shift data were dichotomized to positive postoperative pivot shift (grade 1, 2, or 3) or negative pivot shift and were compared between patients who had ACLR alone and those who had ACLR with LEAT. A pooled odds ratio with 95% confidence interval (CI) was used. The Cochran Q statistic and the I 2 index were used to assess heterogeneity. 22 A larger I 2 index indicates that a greater amount of the variability in the results is due to heterogeneity rather than to chance. 23 Where there was large statistical heterogeneity (I 2 < 50%), a fixed-effects meta-analysis model was used.
A subgroup analysis was performed to examine the influence of time between injury and surgery on the pivot-shift data. Patients who had early reconstruction (mean interval ≤12 months) 2,4,11,60,61 were compared with those who had delayed reconstruction (mean interval >12 months) 3,35,37,53 based on the time period from injury to surgery (Table 2). Studies in which the time period from injury to surgery was not clear or not listed were not included in the analysis. 5,54
Summary of Clinical Outcomes a

a Allo, allograft; Ant, anterior; BPTB, bone–patellar tendon–bone; DB, double bundle; DBH, double-bundle hamstring graft; DS, double-strand; ER, external rotation; GT, gracilis tendon; HS, hamstring; HSS, Hospital for Special Surgery; IKDC, International Knee Documentation Committee; IR, internal rotation; KOOS, Knee injury and Osteoarthritis Outcome Score; LEAT, lateral extra-articular tenodesis; LFC, lateral femoral condyle; MFC, medial femoral condyle; NS, not significantly different; PFC, patellofemoral crepitus; QAT, Quadriceps Activity Test; ROM, range of motion; RTS, return to sport; ST, semitendinosus; VAS, visual analog scale.
Best-Evidence Synthesis
To assist with evaluating the outcome findings that could not be assessed through meta-analysis due to the limited availability of homogenous data, a best-evidence synthesis combining RCTs and CCSs was performed. The method, proposed by Van Tulder et al 56 and adapted by Steultjens et al, 49 was used to ascribe levels of evidence of effectiveness, taking into consideration study design, methodological quality, and statistical significance of the findings (Appendix).
Results
Search Results
The database search retrieved 364 records, and an additional 23 studies were found after reference checks. Following title and abstract screening, 128 potentially relevant studies were obtained in full text. A total of 117 studies were excluded for the following reasons: no LEAT performed (n = 40), noncomparative cohort study (n = 22), isolated LEAT without ACLR (n = 11), synthetic ligament used with LEAT or ACLR (n = 11), outcome not applicable to the study (n = 11), multiple combined procedures performed (n = 10), technical note (n = 4), revision ACLR with LEAT (n = 2), ACL repair (n = 3), and systematic review (n = 2); 2 separate studies 37,38 reported on the same cohort of patients, so O'Brien et al 38 was excluded (Figure 1).
Therefore, a total of 11 studies reporting on comparative studies of ACLR versus ACLR with LEAT were included for qualitative and/or quantitative synthesis (Table 3).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; LEAT, lateral extra-articular tenodesis; N/A, not applicable.
Comparative Studies: ACLR Versus ACLR + LEAT a

a ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; AD, anterior drawer; Allo, allograft; AP, anteroposterior; BPTB, bone–patellar tendon–bone; CCS, case-control study; CPM, continuous passive motion; DB, double bundle; DBH, double bundle hamstring graft; FWB, full weightbearing; GT, gracilis tendon; IKDC, International Knee Documentation Committee; ITB, iliotibial band; KOOS, Knee injury and Osteoarthritis Outcome Score; LEAT, lateral extra-articular tenodesis; LFC, lateral femoral condyle; NWB, nonweightbearing; OTT, over-the-top; Pes, pes anserinus; PFC, patellofemoral crepitus; PS, pivot shift; PT, proximal tibia; pts, patients; PWB, partial weightbearing; RCT, randomized controlled trial; ROM, range of motion; ST, semitendinosus; VAS, visual analog scale.
Methodological Quality
The methodology quality scores ranged from 5 to 14 out of a possible score of 16 (Table 4). Five studies were considered high quality; 4 of these were RCTs, 2,53,60,61 and 1 was a CCS. 11 A further 4 studies were rated as moderate quality, 3,5,35,54 and 2 studies were rated as of low quality. 4,37 Two studies scored positively on item 14 (sample size calculation), while 5 studies reported blinding of assessors with respect to the postoperative pivot-shift assessment. None of the studies provided information on the possibility of selection bias.
Quality Assessment Tool: Modified Downs & Black a

a Adjustment, adequate adjustment for cofounding; Aim, aim of study; Bias, selection bias present; Blinding, attempt to blind measurers; Comparison, comparison group identified; Confounders, clearly described distributions of principle cofounders; Findings, main findings of study; Outcomes, clearly described outcomes; Patient, patient characteristics; Power, sufficient power in study; Quality, ≥12 = high quality, 10-11 = moderate quality, ≤9 = low quality; Random, estimates of random variability; Sample, sample is representative; Statistics, statistical tests used; Sample calc., reported sample size calculation; Valid, measures are valid and reliable.
Demographic Characteristics
The 11 included studies reported on 847 patients (66% men) (Table 3). The median age at surgery was 26 years (interquartile range [IQR], 4.1 years). A wide variation was noted in time from injury to surgery, with a median time period of 12.3 months (IQR, 33.5 months). In 1 study, time between injury and surgery was not reported, 5 and in 1 study a minimum time interval between injury and surgery was reported, which was 2 months. 54 In the early ACLR studies, the median interval between injury and surgery was 6.5 months (IQR, 6.8 months), and the delayed reconstruction studies had a median interval of 37.8 months (IQR, 5 months).
Nine of the 11 studies included data exclusively on patients undergoing primary ACLR. The other 2 studies 3,35 included data within their cohort of some patients who had undergone a prior ACLR, but these represented less than 20% of the total study population. Specifically, in the study by Barber-Westin and Noyes, 3 9 of 52 (17%) patients in the ACLR group and 5 of 32 (16%) of patients in the ACLR with LEAT group had a failed ACLR. Noyes and Barber 35 included 9 of 64 (14%) patients in the ACLR group and 8 of 40 (20%) patients in the ACLR with LEAT group who had failed ACLR. Only the study by Noyes and Barber 35 was included in the delayed reconstruction meta-analysis data.
Meta-analysis Data
Due to the heterogeneity of the outcome data, a meta-analysis was possible only for pivot-shift data. A fixed-effects model was used as a result of I 2 values being less than 50% in all cases.
Primary Analysis—All Studies Regardless of Time From Injury to Surgery
Of the 11 studies included, 9 reported postoperative pivot-shift test findings (738 patients). Five were of high quality, 2 of moderate quality, and 2 of low quality. The odds of having a positive postoperative pivot shift were 52% lower in patients who had ACLR and LEAT compared with patients who had ACLR alone (odds ratio 0.48; 95% CI, 0.32-0.71; P = .0003; I 2 = 22%; 95% CI for I 2 ) (Figure 2).

Meta-analysis using fixed-effects model to compare the pivot-shift test of anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LEAT) versus ACLR alone for all studies. M-H = Mantel-Haenszel test.
Subgroup Analysis—Early ACL Reconstruction (≤12 Months From Injury)
Five studies reported on ACLR plus LEAT that was performed within 12 months of the index ACL injury (394 patients). Four of these studies were of high quality and 1 was of low quality. No statistical difference was found in the number of patients with a positive postoperative pivot-shift test between those who had a combined ACLR plus LEAT and those who had an isolated ACLR (odds ratio, 0.60; 95% CI, 0.33-1.09; P = .10; I 2 = 33%) (Figure 3).

Meta-analysis using fixed-effects model to compare the pivot-shift test of anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LEAT) versus ACLR alone for early reconstruction (≤12 months from injury). M-H = Mantel-Haenszel test.
Subgroup Analysis—Delayed ACL Reconstruction (>12 Months From Injury)
Three studies reported on ACLR plus LEAT that was performed more than 12 months following index ACL injury (291 patients). One was of high quality, 1 of moderate quality, and 1 of low quality. The odds of having a positive postoperative pivot shift were 44% lower in patients who had ACLR plus LEAT compared with patients who had ACLR alone (odds ratio, 0.44; 95% CI, 0.24-0.81; P = .008; I 2 = 0) (Figure 4).

Meta-analysis using fixed-effects model to compare the pivot-shift test of anterior cruciate ligament reconstruction (ACLR) with lateral extra-articular tenodesis (LEAT) versus ACLR alone for delayed reconstruction (>12 months from injury). M-H = Mantel-Haenszel test.
Clinical Outcome
The results of the clinical outcome measures used by each study and the significant findings are outlined in Table 2. A best-evidence synthesis was performed on all outcome measures that were not suitable for meta-analysis.
Best-Evidence Synthesis
A summary of the best-evidence synthesis is listed in Table 5.
Summary of Best-Evidence Synthesis of Secondary Outcomes Comparing the Addition of ACLR With LEAT to ACLR in Isolation a
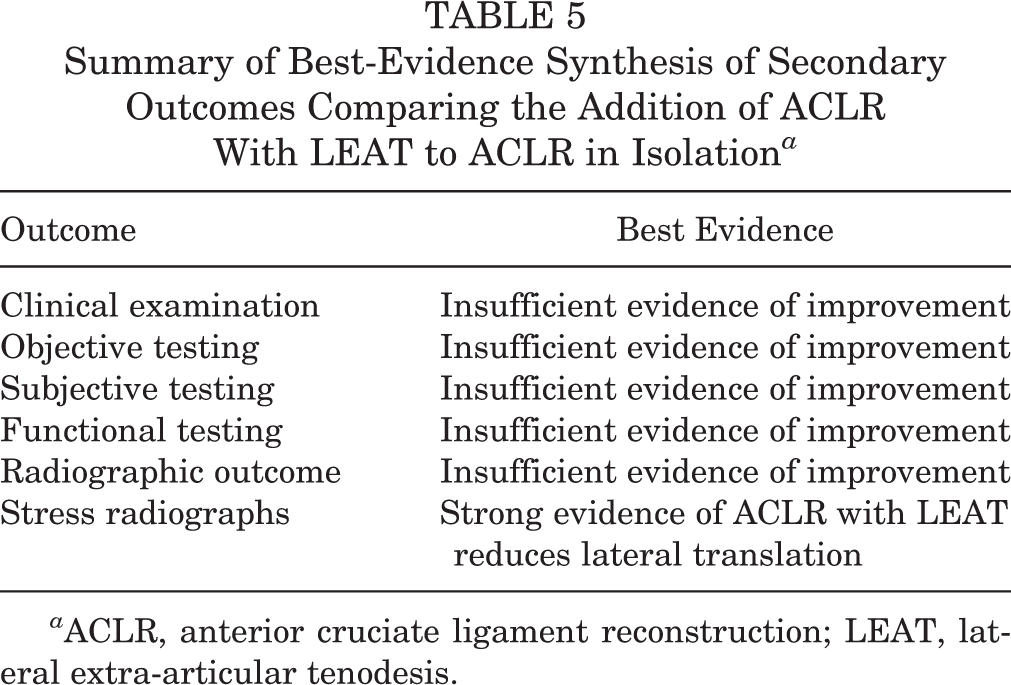
a ACLR, anterior cruciate ligament reconstruction; LEAT, lateral extra-articular tenodesis.
Clinical Examination
Four studies (3 RCTs) reported on range of motion, 2,4,60,61 and a further 6 studies (2 RCTs) detailed postoperative Lachman testing. 2,4,5,37,54,61 Insufficient evidence was found to indicate whether the addition of LEAT to ACLR affected postoperative range of motion or Lachman testing.
Objective Testing
Nine studies (3 RCTs) carried out an objective assessment of anterior translation using the KT-1000 or KT-2000 arthrometer. 2 –5,36,37,54,60,61 There was insufficient evidence to suggest that the addition of LEAT to ACLR improved anterior laxity as measured with an arthrometer. Two studies (1 RCT) assessed quadriceps and hamstring strength. 2,35 Insufficient evidence was found to suggest whether the addition of LEAT had any effect on postoperative quadriceps or hamstring strength following ACLR.
Subjective Outcome
Eleven studies (4 RCTs) reported on subjective outcomes. Seven studies reported International Knee Documentation Committee (IKDC) scores, 3 studies reported Hospital for Special Surgery (HSS) scores, and 6 studies reported a variety of subjective outcome scores. The evidence was insufficient to indicate whether the addition of LEAT to primary ACLR results in improved subjective outcome.
Functional Outcome
Functional outcome was assessed with Tegner score in 4 studies (2 RCTs) 4,54,60,61 and Lysholm score in 2 studies. 4,54 No statistical differences were found in any of the reported studies. There was insufficient evidence that the addition of LEAT to primary ACLR affects functional outcome scores.
Two studies (1 RCT and 1 CCS) specifically detailed return to sport (RTS) as a functional outcome and found no significant difference based on the addition of LEAT. 11,53 Therefore, the evidence was insufficient to indicate whether the addition of LEAT affects RTS following primary ACLR. Two high-quality studies detailed the time to RTS. 60,61 Zaffagnini et al 60 found that the time to RTS was improved in double-bundle ACLR compared with double-strand hamstring with LEAT. In an earlier study, 61 the same authors reported that patients receiving double-strand hamstring ACLR returned to sport earlier compared with patients receiving bone–patellar tendon–bone (BPTB) and 4-strand hamstring ACLR. Therefore, insufficient evidence was found to suggest whether the addition of LEAT to a primary ACLR results in an improved time to RTS.
Radiographic Evaluation
Three studies (3 RCTs) studied postoperative radiographic evaluation. 2,60,61 The evidence was insufficient to indicate whether the addition of LEAT to primary ACLR affects short-term radiographic outcome.
Radiological stress testing was carried out in 2 high-quality studies. Trichine et al 53 reported decreased laxity of the lateral femoral condyle in the BPTB and LEAT reconstruction compared with BPTB alone. Similarly, Dejour et al 11 found that the addition of LEAT to BPTB ACLR was superior in reducing the anterior tibial translation of the lateral compartment as measured by Telos stress radiography. Therefore, strong evidence was found that the addition of LEAT results in decreased translation of the lateral compartment of the femur as measured by stress radiographs.
Discussion
This systematic review identified time from injury to surgery as an important factor in determining the effectiveness of adding LEAT to a primary ACLR to reduce the postoperative pivot shift. Meta-analysis of the pivot-shift data acquired from 5 studies comparing ACLR alone versus ACLR with LEAT in primary procedures performed within 12 months of injury revealed that the addition of LEAT did not significantly reduce the odds of having a postoperative pivot shift. However, when the same analysis was performed on 3 studies in which the ACLR was delayed in excess of 12 months following injury, the addition of the LEAT did reduce the pivot shift.
Of the 11 studies included for data synthesis, 5 were of high quality, 4 moderate quality, and 2 low quality.
Based on a best-evidence synthesis of outcome measures, evidence is insufficient to establish whether the addition of LEAT to a primary ACLR improves clinical examination findings, objective testing, or subjective and functional outcomes. There is, however, strong evidence to suggest that LEAT performed with ACLR reduces lateral compartment translation as measured by stress radiography.
Although the LEAT procedure has re-emerged as an adjunct surgical option for the treatment of ACL-deficient knees, clear indications for its use are still lacking. This systematic review demonstrated that the addition of LEAT to ACLR may improve rotational stability in a delayed reconstruction but does not offer the same benefit in early reconstruction. In addition, there is insufficient evidence to establish whether LEAT improves other clinical outcomes in primary ACLR.
The use of LEAT procedures has fluctuated over the years and, like many things in orthopaedics, has followed something of a trend. This is highlighted in this systematic review if one considers the time periods in which the studies were undertaken and published. Six studies emerged from the United States in the 1980s and early 1990s, but none have been published since then. The discontinuation of LEAT may be explained by the publication of seminal articles from high-profile institutions in the United States claiming that this procedure was unnecessary, especially in the acute setting, and might be potentially harmful. 35,37,46 Another explanation relates to the emerging technology of the era, particularly the increasing availability of magnetic resonance imaging (MRI) and the move to arthroscopic ACLR 9,10,19,40,41,57 ; the former facilitated an earlier and more accurate definitive diagnosis of ACL rupture, while the latter possibly steered surgeons away from making big incisions around the knee, which had previously been done.
One of the other concerns related to LEAT was the potential to overconstrain the lateral compartment of the knee, which raised fears regarding the development of lateral compartment osteoarthritis. This review has highlighted the strong evidence that the translation of the lateral compartment is reduced with the addition of LEAT. These clinical findings are supported by biomechanical studies that demonstrate an overconstraint of the lateral compartment with both anatomic ALL reconstruction and LEAT procedures. 44,47 However, a recent systematic review reported that there is no increase in the long-term rates of osteoarthritis with the addition of LEAT to ACLR. 12
Two recent systematic reviews of this topic have reported findings similar to those of the current study. 21,48 Both studies concluded that the addition of LEAT to ACLR was effective in eliminating pivot shift, particularly high-grade preoperative pivot shift. These results are consistent with our meta-analysis findings regarding delayed reconstruction but differ from our meta-analysis findings regarding early reconstruction. This difference may be explained in part by the use of different inclusion criteria. Song et al 48 included all levels of evidence but only ACL-deficient knees with a manual pivot-shift grade 2 (clunk) or grade 3 (locking). A study with exclusively revision cases was also included. In contrast, Hewison et al 21 included not only primary ACLR and comparative studies but also studies that used synthetic ligaments, multiple extra-articular reconstructions, and nonconventional ACLR grafts. As such, the patients included in these reviews may not be representative of the typical primary ACL-injured patient. However, the main reason for the difference is probably that, in the current review, a deliberate distinction was made between early and delayed reconstruction, which was not done in either of the other systematic reviews. We believe this distinction is important because a chronically ACL-deficient knee may have a much higher grade of pivot shift due to multiple subluxation events. For people with chronic ACL deficiency, the control offered by ACLR alone may be insufficient to diminish the pivot shift. 35 In contrast, people with a recent, primary ACL injury could be expected to have less rotational instability. 45 Therefore, adding LEAT to ACLR might not be warranted.
Although regarded as one of the most sensitive ways to diagnose ACL insufficiency, the pivot-shift test is subjective, and variability between examiners has been noted in previous studies. 34 However, despite much promise in attempting to objectify this measure with mechanical and optical tracking devices, the pivot-shift maneuver is still the most widely used method to assess rotational stability. 33,52 Moreover, all the studies included in this systematic review used the pivot shift to compare primary ACLR with and without LEAT. It is possible that the angle at which the LEAT was fixed may have affected the grade of pivot shift, as previously suggested with anatomic ALL reconstruction. 43 Unfortunately, of the 11 studies included, only 4 listed these details, which precludes any further analysis on the impact of these variables in the current study.
Limitations
Strict, predefined inclusion criteria were used in this study, and as a result some studies were excluded due to low subject numbers or the lack of controls. The search strategy included only studies published in the English language, and it is possible that studies published in other languages may have met the other inclusion criteria. There is, therefore, a risk of language bias in this systematic review. The results of this review are limited by the lack of consistent methods for collecting patient-reported outcomes and by a lack of long-term outcomes studies. Due to the heterogeneity of the data, a meta-analysis could be performed only on postoperative pivot-shift data. We acknowledge that the postoperative immobilization and rehabilitation techniques included in one of the early studies in this systematic review may not reflect modern practices. 37 Further, 2 studies included data on patients who had undergone a prior failed ACLR, 3,35 although this represented less than 20% of the individual study population, and only 1 of these studies 35 was included in the meta-analysis. In addition, 2 studies included data on ACLR performed through an open technique, which is no longer common. 4,37 Finally, the placement of the ACL graft in many of the studies may not be in keeping with current anatomic reconstruction techniques; however, we believe this reflects the diversity of ACLR techniques internationally.
Conclusion
The results of this systematic review revealed that the addition of LEAT to ACLR does not provide additional benefit in early primary reconstructions (≤12 months) but is effective in reducing the postoperative pivot shift in a delayed ACLR. A best-evidence synthesis determined that there is insufficient evidence to determine whether the addition of LEAT to a primary ACLR resulted in improved clinical, objective, subjective, or functional outcomes. However, there was strong evidence that LEAT results in decreased laxity of the lateral compartment as measured by stress radiography.
These results suggest that in the setting of primary ACLR, there is a limited role for LEAT. This procedure is likely to benefit only those patients undergoing delayed reconstruction with significant rotational instability.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Appendix
Best-Evidence Synthesis a

| Strong evidence | Provided by consistent, statistically significant findings in outcome measures in at least 2 high-quality RCTs. |
| Moderate evidence | Provided by consistent, statistically significant findings in at least 1 low-quality RCT or high-quality CCS. |
| Limited evidence | Provided by consistent, statistically significant findings in outcome measures in at least 1 high-quality RCT or provided by consistent, statistically significant findings in outcome measures in at least 2 high-quality CCS (in the absence of high-quality RCTs). |
| Indicative findings | Provided by consistent, statistically significant findings in outcome and/or process measures in at least 1 high-quality CCS or low-quality RCT (in the absence of high-quality RCTs) or provided by consistent, statistically significant findings in outcome and/or process measures in at least 2 noncontrolled studies with sufficient quality (in the absence of RCTs and CCS). |
| No or insufficient evidence | In the case that results of eligible studies do not meet the criteria for 1 of the above-stated levels of evidence or in the case of conflicting (statistically significant positive and statistically significant negative) results among RCTs and CCS or in the case of no eligible studies. |
| If the number of studies that show evidence is <0% of the total number of studies found within the same category of methodological quality and study design (RCT, CCS, or other design), no evidence will be stated. |
a CCS, case-control study; RCT, randomized controlled trial.