
Abstract
Background:
Elbow ulnar collateral ligament (UCL) injuries are common, particularly in adolescent athletes playing overhead sports. While the incidence and outcomes of surgical UCL injuries are well documented, the nonsurgical UCL injury patterns and injury management in this population are not yet known.
Purpose/Hypothesis:
The purpose of this study was to retrospectively assess the injury severity and subsequent management of UCL injuries among competitive athletes aged 11 to 22 years. We hypothesized that nonsurgical UCL injuries would occur more frequently in younger athletes compared with older athletes.
Study Design:
Descriptive epidemiological study.
Methods:
Electronic medical records (using International Classification of Diseases, 9th Revision and 10th Revision and Current Procedural Terminology codes) and keyword searches were used to identify all patients with sports-related UCL injuries between January 2000 and April 2016. A total of 136 records were included. Patients were stratified into 3 age brackets (age 11-13 years, n = 17; age 14-16 years, n = 49; age 17-22 years, n = 70). There were no prior elbow surgical interventions. The main outcome measures included the frequency and severity of UCL injuries and injury management (surgical, nonsurgical). Independent variables included age, UCL injuries per year, and sport classification.
Results:
There were 53 surgical and 83 nonsurgical UCL injuries. The number of nonsurgical cases increased 9-fold from 2000-2008 to 2009-2016. The UCL injuries were distributed as follows: 60 sprains, 39 partial tears, 36 ruptures, and 1 rerupture. Moreover, 7% of sprains, 51% of partial tears, and 78% of ruptures underwent UCL reconstruction. Nonsurgical management was most common in the youngest athletes (age 11-13 years, 100.0% of total injuries; age 14-16 years, 71.4% of total injuries; and age 17-22 years, 44.3% of total injuries) (P = .007). UCL injury volume was most commonly associated with javelin (odds ratio, 6.69; 95% CI, 0.72-61.62; P = .07) and baseball (odds ratio, 1.55; 95% CI, 0.69-3.51; P = .32).
Conclusion:
Younger athletes sustained less severe UCL injuries more often than older athletes. Participation in javelin and baseball was associated with a greater likelihood of UCL injuries based on our dataset. This is the first study to provide data on the volume of nonsurgical UCL injuries among athletes in various sports.
The ulnar collateral ligament (UCL) is the primary stabilizer of the elbow, and it resists valgus stress applied to the elbow joint. 32 Injuries to the UCL greatly compromise stability of the elbow. UCL injuries and subsequent ruptures are common among participants in overhead-throwing sports. 12,25 Damage to the UCL in the overhead-throwing athlete is a severe and potentially career-threatening injury. This injury can be managed conservatively or with surgical reconstruction (UCL-R).
UCL-R has become increasingly common among players at all levels of experience since the 1990s. 1,14,21,43 Evidence shows that the number of UCL-R in youth has increased 6-fold since the mid-1990s and continues to grow. 1,17 Unfortunately, this trend is expected to continue through the year 2025, particularly in athletes 15 to 24 years of age. 35
With a continuing rise in these injuries, there has also been a growth of misinformation in the media, which can lead to inaccurate information regarding UCL injuries in the general public. 8 Johnson et al 23 reported that patients are using the Internet for information regarding this injury and that the quality, accuracy, and readability regarding UCL injuries are potentially incorrect. Thus, a study of this type is warranted so that all physicians, including nonoperative physicians who care for athletes with this type of injury, are aware of the most up-to-date information.
At present, considerable information is known about the prevalence, incidence, and outcomes of UCL-R 8 –11 ; the epidemiology of UCL-R at advanced levels of competition 7 ; surgical techniques; and new research on UCL repair versus UCL-R. 13,15,49 The frequency and severity of UCL injuries and the proportion of those injuries that undergo surgical versus nonsurgical management remain unknown. These findings are important for clinicians who care for athletes with this injury.
The purposes of this study were to determine (1) whether the frequency and severity of UCL injuries differed based on an athlete’s age, sport, and time participating in competitive sports and (2) whether there were different patterns of surgical and conservative management for these injuries based on injury severity. We hypothesized that (1) less severe UCL injuries would occur more frequently in younger athletes in sports with repetitive, high-volume stress (such as baseball) compared with their older cohorts and (2) younger athletes would be managed conservatively for their injury, and older athletes would demonstrate the highest frequency of UCL-R among our patient groups.
Methods
Study Design
This was a retrospective chart review study. Data were reviewed from medical records from January 1, 2000, to April 26, 2016. Approval was obtained from our institutional review board for all study procedures. Once approval was obtained, a formal medical request was made with the above criteria to our institution’s Faculty Practice Health Department for chart retrieval.
Patients
Patients aged 11 to 22 years who sustained a UCL injury to the elbow during a sports competition were included. International Classification of Diseases, 9th Revision (ICD-9) and 10th Revision (ICD-10) and Current Procedural Terminology (CPT) codes were used to find patients. Elbow sprain (ICD-9 841.1, 841.9, 842.00, 848.9 or ICD-10 [UCL sprain of the elbow] S53.449A, S53.441A, S53.442A), elbow UCL rupture (ICD-9 841.1, 905.7 or ICD-10 S53.30XA, S53.31XA, S53.32XA), and UCL rupture reconstruction (CPT 24346) were used as the main injuries for the patient search.
Data Abstraction
Patient charts were identified using ICD-9, ICD-10, and CPT codes. Using these codes, we added a keyword search to ensure that we obtained every possible UCL injury with our inclusion criteria. The keyword search involved any of the following words in combination with the above codes: athlete, athletic, baseball, basketball, college, elbow, football, high school, javelin, Little League, pitcher, professional, quarterback, soccer, softball, sports, swimming, and tennis. There were 300 total charts initially obtained. After an initial chart screen to check that inclusion was appropriate, this list was narrowed down to 136 charts. Charts that were not included (n = 164) described patient injuries that did not pertain to the above criteria. These included injuries to the olecranon, osteochondritis dissecans of the capitellum, loose bodies of the elbow, ulnar nerve injuries, medial epicondylitis, avulsions of the medial epicondyle, mallet finger, flexor carpi ulnaris strain, stress reactions of the distal humerus and olecranon, UCL injuries of the elbow due to trauma and not related to sports (such as falling off a bicycle), elbow dislocations, lumbago, triceps tendinitis, valgus extension overload syndrome, ulnar fractures, radius fractures due to blunt trauma, plica syndrome, and labral injuries of the shoulder (flow of chart selection process is shown in Figure 1).

Chart selection process for patients with an ulnar collateral ligament (UCL) injury.
Patient-related data points included age, time of injury per year, sport played, and position in sport. Injury-related data points included injury severity (sprain vs partial tear vs complete rupture of the UCL), hand dominance, injury management (surgical intervention vs nonsurgical management), and imaging modality used to diagnose the injury (clinical examination alone, radiography, magnetic resonance imaging [MRI], magnetic resonance arthrography [MRA], or combination). Injury severity was determined based on a clinical examination combined with imaging (119 underwent advanced imaging of which 82 underwent MRA plus radiographs, 34 underwent MRI plus radiographs, 16 radiograph only, 2 had MRI only, 1 MRA only, and 1 underwent radiographs plus ultrasound only). For statistical analyses, data were categorized based on patient age (11-13, 14-16, and 17-22 years), time frame (4-year clusters spanning 2000-2016), and sport (baseball, javelin, softball, and American football).
For the purposes of this study, the severity of UCL injuries was defined based on the presence of a sprain, partial tear, or complete rupture. This categorization was based on the scheme used by Ford et al. 20 A sprain of the UCL had no tear, thickening, or stripping with or without edema around the anterior band, with positive clinical symptoms (such as pain at the sublime tubercle and/or pain with valgus loading of the medial elbow). A partial tear was defined as at least a partial tear of the anterior band of the UCL. A complete rupture was defined as at least a complete tear of the anterior band of the UCL. Position in sport was determined via a chart review and listed per history in each chart.
All surgical reconstruction procedures were performed by board-certified orthopaedic surgeons. All patients were initially evaluated by board-certified primary care sports medicine physicians (primary specialties included physical medicine and rehabilitation, pediatrics, or family medicine), orthopaedic sports medicine surgeons, or pediatric orthopaedic surgeons. All 9 nonoperative primary care sports medicine physicians who were involved in the care of the included patients obtained a certificate of additional qualification in sports medicine and have been team physicians at the high school and/or collegiate levels.
Statistical Analysis
Descriptive statistics of UCL injuries by sport and age group were performed. Differences in injury frequency and severity were determined using chi-square analyses. Odds ratios and 95% CIs were determined for sport type. Statistics were performed using the Statistical Package for the Social Sciences (v24; SPSS).
Results
Injury Severity and Injury Management
There were 136 total UCL injuries, including 53 that were treated with UCL-R and 83 that were managed conservatively. All patients were assessed clinically and with imaging modalities. There were a total of 60 UCL sprains, 39 partial tears, 36 ruptures, and 1 rerupture (Figure 2). Most sprains did not require surgery, however surgical management increased with greater injury severity. There were 16 patients who underwent radiography only, 34 who underwent radiography plus MRI, 82 who underwent MRA plus radiography, 2 who underwent MRI only, 1 who underwent MRA only, and 1 who underwent radiography plus ultrasound only. All cases of radiography only (plus the 1 case with combined ultrasound) were diagnosed as sprains and did not result in surgery.

Severity and management type (by No. of injuries) for ulnar collateral ligament injuries among athletes aged 11 to 22 years.
Age at Time of Injury
The mean age at the time of injury for all patients was 16.7 years. The mean age of patients undergoing UCL-R and conservative management was 16.0 and 17.1 years, respectively. Less severe UCL injuries occurred with a higher frequency in younger patients. Patients who sustained sprains had a mean age of 15.9 years, those with partial tears had a mean age of 16.9 years, and patients with ruptures had a mean age of 17.6 years (Table 1). There were increasing numbers of UCL injuries with increasing age (χ2(4, 136) = 14.209, P = .007) (Table 1).
Severity of UCL Injury by Age a
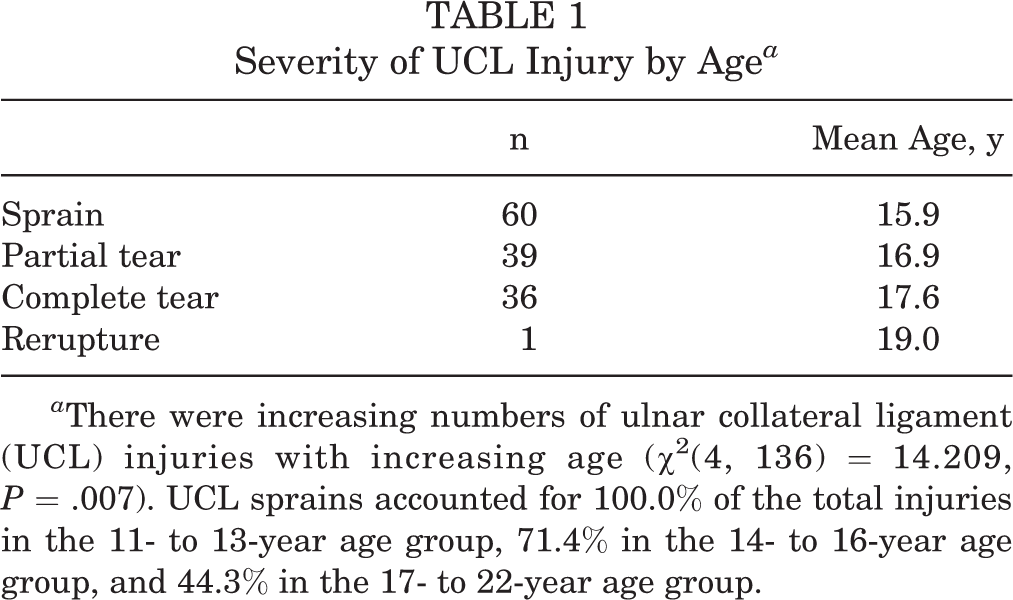
a There were increasing numbers of ulnar collateral ligament (UCL) injuries with increasing age (χ2(4, 136) = 14.209, P = .007). UCL sprains accounted for 100.0% of the total injuries in the 11- to 13-year age group, 71.4% in the 14- to 16-year age group, and 44.3% in the 17- to 22-year age group.
Sport Type and Injury
The injury incidence among different sports is shown in Figure 3. The odds ratio (OR) for UCL injuries was highest in patients who played javelin (OR, 6.69; 95% CI, 0.72-61.62; P = .07) and baseball (OR, 1.55; 95% CI, 0.69-3.51; P = .32) compared with all other sports activities. Of the 42 UCL-R procedures performed on baseball players, 37 were performed on pitchers. There were 20 pitchers who sustained complete ruptures, 14 partial tears, and 3 sprains (2 of which failed rehabilitation).

Ulnar collateral ligament (UCL) injuries by sport. Values represent the number of cases. MMA, mixed martial arts.
Time Frame and Injury Incidence
There were a total of 5 injuries from 2000 to 2003, 9 from 2004 to 2007, 50 from 2008 to 2011, and 72 from 2012 to April 26, 2016 (date determined according to institutional review board approval). This represented a more than 12-fold increase in less than 16 years (Figure 4).

Annual incidence of ulnar collateral ligament (UCL) injuries during the time frame from 2000 to 2016. Note that 2016 data were available for a partial year through April 26 (per Institutional Review Board approval).
Discussion
We report that among patients aged 11 to 22 years, those who had less severe UCL injuries were younger compared with patients who had more severe injuries. Fewer surgeries were performed among the patients with less severe injuries. These findings are consistent with our hypotheses. In addition, our data, similar to those of prior large-scale studies, revealed that baseball players (particularly pitchers) sustained the greatest number of UCL injuries. 4,41 In our dataset, 101 of our 136 patients were baseball players (74.3%). Furthermore, our findings agree with published trends of the increasing incidence of UCL-R over the past 20 years. 7,14,21
While UCL injuries are a well-known issue in baseball players, there have also been reports of UCL injuries in overhead athletes who participate in American football, javelin, gymnastics, softball, tennis, and water polo. 11,12,39 Our data revealed that 80% of our javelin athletes and 54% of our baseball pitchers with complete ruptures underwent UCL-R. This is likely in part because of sport-specific biomechanical factors. The severity of UCL injuries is influenced by the amount of stress placed on the medial elbow with overhead throwing. Javelin throwers can generate an angular velocity of about 1900 deg/s, while baseball pitchers can approach nearly 2480 deg/s of elbow angular velocity. 9,19 These 2 sports generate the greatest velocity and resulting stress across the medial elbow compared with other overhead-throwing sports. Older and higher-level pitchers throw with greater linear velocity and generate greater torque during the acceleration phase of throwing (nearly 50 N·m at the collegiate level). 19
A case can be made that older pitchers also throw more pitches. While it is difficult to differentiate whether higher-level and older pitchers suffer UCL injuries because of more pitches thrown versus greater velocity and forces on the elbow, restrictions have been enacted at the high school level in a majority of states to prevent overuse. 31,37 Given new pitch count regulations, future research may be able to differentiate whether an elbow injury was from greater velocity or a greater volume of throwing.
A significant volume of science surrounds UCL-R in the literature 4,7,14,41 but not on nonsurgical management. We found that 61% of our UCL injuries did not undergo UCL-R. One study of 18 National Football League players described that 100% of injured players returned to play after nonsurgical management, with a mean loss of game time of 0.64 games. 28 However, other studies have reported less success with nonoperative management. For example, 2 studies of overhead-throwing baseball athletes reported a 42% to 50% rate of return to play. 3,46 However, there are challenges interpreting these findings because of the absence of injury severity data. The time frame for making the decision to pursue surgery is based on several factors. These include location of the UCL injury, severity of the injury, timing of the injury (in season or out of season), year of the athlete in school, and potential ability to continue playing above the current level of play. 45 At our institution, nonoperative management of these injuries typically includes a period of nonthrowing physical therapy until the patient is asymptomatic. We make sure that there is no valgus force or strain applied in any maneuver during this time. The use of orthobiologics is also considered and made on a case-by-case basis. 10,44 After the first 6 weeks, return to a throwing program (if the patient is a thrower) is initiated over an approximate 6-week period. After this 3-month period, if the patient continues to have pain and/or difficulty with throwing or overhead activities without a significant improvement in symptoms, then a surgical referral is placed. While this program has evolved over the past 16 years, the overall components have remained the same.
When considering injury prevention in younger athletes, significant research exists surrounding the relationships between an overuse throwing injury and pitch volume, fatigue, rotator cuff weakness, poor pitching mechanics, and possibly year-round pitching. 16,18,26,33,50 However, there are no data on the severity of UCL injuries by age and management pathway (Figure 2). In this study, athletes who suffered less severe injuries were younger in age than players who had more severe injuries (Table 1). Surgery was used less frequently in cases where injuries were less severe (Figure 2). We feel that this finding does lend credibility to the notion that athletes are sustaining more UCL injuries at a younger age, and this may predispose these athletes to suffer more severe injuries as they become older. Prior research has reported that 26% to 29% of young baseball athletes suffer from elbow pain. 34,36 Even more concerning, youth pitchers between 9 and 14 years old have a 5% risk of a severe injury, which is defined as elbow or shoulder surgery, or retirement from the sport within 10 years due to an injury. 18,34
Application of Findings
The challenge is to prevent the further progression of a less severe UCL injury and/or to develop novel treatments as an alternative to UCL surgical intervention in non–full-thickness ruptures. Treatment decision making of UCL injuries is dependent in part on the severity of the injury. Imaging modalities are extremely useful in combination with a thorough history and physical examination. MRI has typically been the standard in identifying UCL injuries, particularly full-thickness tears. 20,48 However, there is evidence that MRA may provide additional imaging details for evaluating the severity of UCL injuries, particularly partial tears. 5,38,47
Additional challenges arise when trying to determine the severity of partial tears of the UCL. Ford et al 20 created an MRI grading scale to classify UCL injuries into 4 levels of severity: I (intact ligament with or without edema), IIA (partial tear with incomplete fiber disruption), IIB (chronic healed injury with thickened ligament but no fiber disruption), and III (complete tear with fiber disruption). Our definitions of a sprain, partial tear, and complete tear of the UCL were based on this scheme. Newer research has developed a UCL classification system using a combination of valgus laxity on radiography in conjunction with MRI. Joyner et al 24 proposed a 4-level grading system: type I, edema in the UCL only (called a low-grade partial tear); type II, a partial tear of the UCL with no extravasation of fluid on MRA (called a high-grade partial tear); type III, a complete full-thickness tear of the UCL with extravasation of fluid on MRA; and type IV, a tear in more than 1 location on the UCL. While these newer grading schemes are similar, it is important to note that a correlation of pain must be present to make the diagnosis of a UCL injury. Prior research has shown that overhead athletes, particularly baseball players, may be asymptomatic but still have abnormalities on MRA. 22,30,42 Thus, the combination of a clinical examination was required to make the diagnosis of a UCL injury. It should be noted that ultrasonography with an experienced operator is another imaging modality that can be used to make a diagnosis. 2,6,27,29
Limitations
This study has various limitations. The retrospective nature precludes the determination of the ultimate use of surgical management. Second, we were unable to ascertain the severity of the partial tears sustained in our dataset. Only reports of MRI and/or MRA were available in some cases, not the images themselves. This limited the classification of partial tears further into lower versus higher grades and could have affected decision making for operative versus nonoperative treatment. In addition, with the growing awareness of UCL injuries, it is possible that this diagnosis is identified more by clinicians now than in the past. 40 Injury incidence may not have changed among the sports over time, but the recognition and reporting of the injuries may have improved from 2000 to 2016. Finally, we could not determine what percentage of these injuries in the community came to our facility versus other offices and centers, although our center does have the largest number of fellowship-trained orthopaedic and sports medicine providers in the region.
Conclusion
Younger athletes are more likely to sustain less severe UCL injuries than older athletes in those patients who present for medical care. In this study sample, participation in javelin and baseball was associated with a greater likelihood of UCL injuries compared with other sports. This is the first study to provide data on the volume of nonsurgical UCL injuries among athletes aged 11 to 22 years in a variety of sports. Clinicians need to be aware of the significant rise in nonsurgical UCL injuries in adolescent athletes. These data suggest that the majority of UCL injuries sustained in such athletes do not necessarily require surgical intervention, only severe ones in throwing athletes.
Footnotes
Presented at the International Olympic Committee’s World Conference on Prevention of Injury and Illness in Sport, Monte Carlo, Monaco, March 2017.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the University of Florida (Institutional Review Board No. 201600546).