
Abstract
Background:
The lever sign test is a new physical examination tool to diagnose anterior cruciate ligament (ACL) tears. Preliminary results suggest almost 100% sensitivity and specificity to diagnose acute and chronic complete ACL tears and clinically significant partial tears as compared with magnetic resonance imaging (MRI).
Purpose:
To assess the sensitivity and specificity of the lever sign test for the diagnosis of acute ACL injuries, as compared to MRI. We also aimed to determine the accuracy of the lever sign test compared with 3 other tests (anterior drawer, Lachman, and pivot shift) when performed by providers of various training levels, and with the patient awake or under anesthesia.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
We evaluated patients with a chief concern of acute (≤4 weeks) knee pain seen between October 2014 and January 2015, with a thorough history, physical examination, and standard radiographs. MRI was the reference standard; patients without an MRI evaluation were excluded. The 4 physical examination maneuvers were performed on each symptomatic knee during the initial clinic visit (for nonsurgical patients) or under anesthesia in the operating room (for surgical patients) by a randomly assigned undergraduate student, medical student, orthopaedic resident, or orthopaedic fellow. The senior author trained all staff to perform the lever sign test. Statistical analyses were performed.
Results:
Of 102 patients, 54 were surgical (28 female, 26 male), and 48 were nonsurgical (16 female, 32 male); the mean patient age was 23 years (range, 15-66 years). The overall accuracy of the lever sign test was 77% (63% sensitivity, 90% specificity); the accuracy was similar between patients under anesthesia and awake (77% vs 76%, respectively). There were no significant differences when comparing the sensitivity and specificity of the lever sign test with patients under anesthesia and awake (sensitivity: under anesthesia, 86%, and awake, 68% [P = .40]; specificity: under anesthesia, 85%, and awake, 96% [P = .17]). Furthermore, the accuracy of the lever sign test was similar when performed on female versus male patients (75% vs 79%, respectively) or when performed by undergraduate students and medical students compared with orthopaedic residents and fellows (84% vs 88%, respectively).
Conclusion:
Our study results challenge the exceptional sensitivity and specificity values (both 100%) of the lever sign test, as reported by the original author of the test.
The anterior cruciate ligament (ACL) is one of the most commonly injured knee ligaments, with nearly 200,000 injuries per year in the United States, and with an estimated 100,000 reconstructions annually. 2,28 The ACL consists of 2 distinct bundles, the anteromedial and the posterolateral, named for their respective insertion sites from the tibia to the femur. 29,39 The ACL is responsible for preventing anterior translation of the tibia relative to the femur and also acts as a secondary restraint to tibial rotation and varus/valgus rotation. 3,10,16
Early recognition of pathological processes of the ACL is crucial to selecting the correct course of care to optimize outcomes. The diagnostic standard for ACL injuries is direct arthroscopic visualization, but the accepted reference standard is magnetic resonance imaging (MRI), with sensitivity and specificity ranging from 94% to 98%. 5,18 Imaging is regularly preceded by a thorough history and physical examination, which is the physician’s first opportunity to identify an injury. The 3 most widely accepted clinical tests to diagnose an ACL tear include the anterior drawer, Lachman, and pivot-shift tests, all of which were initially described in the 1970s. 11,26,35 In a meta-analysis of 17 studies, these 3 clinical tests were found to have a wide range of diagnostic accuracy for an ACL tear (Table 1). 31 The accuracy of these examinations may be affected by patient factors such as swelling, pain, protective muscle action, and examiner experience. The maneuvers themselves can produce falsely normal results, particularly in patients with partial tears. 1,6,20,39 Furthermore, individual modifications are often implemented because of anatomic variability of the patient as well as differences in the training level of the physician. 12,21,24,36 In addition to orthopaedic surgeons, emergency medicine and primary care physicians, among others, are often tasked with the initial assessment of an acute knee injury. One study illustrated the misdiagnosis of ACL ruptures by emergency medicine physicians in 74% of acute knee injuries. 12
Results of Meta-analysis by Scholten et al 31

a Pooled values from 6 studies.
b Values from 4 studies. The values could not be pooled because of insufficient studies evaluating this diagnostic tool. This test had the highest positive predictive value of the 3 evaluated tests.
The desire for an easy-to-perform clinical test to diagnose partial and complete ACL tears, regardless of the elapsed time from injury, encouraged Dr Allesandro Lelli to report the lever sign test. 19 A preliminary analysis of the test suggested almost 100% sensitivity to diagnose acute or chronic, as well as complete or partial, ACL tears compared with MRI. 19
The purpose of the current study was to (1) assess the sensitivity and specificity of the lever sign test in the diagnosis of acute ACL injuries as compared with MRI; (2) determine the accuracy of the lever sign test compared with the anterior drawer, Lachman, and pivot-shift tests; (3) determine the accuracy of the lever sign test when performed by providers of various training levels; (4) determine the accuracy, sensitivity, and specificity of the lever sign test when performed with the patient awake or under anesthesia; and (5) determine if patient sex affects the accuracy of the lever sign test. Our hypothesis was that the sensitivity, specificity, and accuracy of the lever sign test are similar to those of the current physical examination tests. Additionally, no significant differences were expected when the lever sign test is performed by providers with different levels of training, in the 2 different settings, or based on the patient’s sex.
Methods
The study protocol was reviewed and approved by our institutional review board. This study evaluated consecutive patients seen at a single sports orthopaedic clinic between October 1, 2014, and January 31, 2015. All patients with a chief concern of acute knee pain who came for an evaluation within 4 weeks of their injury or the onset of symptoms were eligible to be enrolled. Previous surgery did not preclude inclusion in the study. All patients underwent a thorough history, physical examination, and standard radiographs. Patients who underwent MRI of their knee, ordered either by the referring provider or by the senior author (A.C.), were included in this study. Because MRI was used as our reference standard, patients were excluded if they did not undergo an MRI evaluation. All 102 consecutive patients were evaluated in the office. If they went to the operating room to address any surgical abnormality (meniscal, chondral, and/or ligament) before January 31, 2015, they were included in the surgical cohort. This methodology allowed for patients with all abnormalities to be included in both cohorts to minimize bias. If patients did not go to the operating room in the allotted time period, even if they needed surgery, they were included in the nonsurgical cohort, and MRI was used as the reference standard for ACL lesions.
To assess the integrity of the ACL, 4 physical examination maneuvers—the anterior drawer, Lachman, pivot-shift, and lever sign tests—were performed on each symptomatic knee by a single randomly assigned undergraduate student, medical student, orthopaedic resident, or orthopaedic fellow. In the nonsurgical group, the 4 tests were performed during the initial clinic visit, and in the surgical group, the 4 tests were performed in the operating room with the patient under anesthesia. The testers were blinded to the patient history, office physical examination findings, radiographic and MRI findings, and operative procedure. To keep testers blinded, the surgical patients were checked both in the clinic and in the operating room under anesthesia. The examination in the operating room was recorded and used for the surgical cohort, as the diagnosis in the awake patient was known by the tester by the time that the patient reached the operating room. The examination in the operating room was conducted by a different provider and used to minimize bias. For all surgical patients, the ACL was visualized directly during diagnostic arthroscopic surgery performed by the senior author. The definitive ACL status was determined by MRI in nonsurgical patients and by arthroscopic surgery in surgical patients.
Although current examination testing uses International Knee Documentation Committee parameters (1+, 2+, 3+), these tests are user and anesthetic dependent, 13 whereas Lelli et al 19 claimed that the lever sign test avoids these requirements. The anterior drawer, Lachman, and pivot-shift tests were performed as dichotomous tests, as described by Torg et al, 35 and were recorded as positive (ACL torn) or negative (ACL intact) findings. The lever sign test was also performed as a dichotomous test, as described by Dr Lelli’s VuMedi video description (https://www.vumedi.com/video/the-lelli-test-3/). The following technique was established: With the patient in a supine position, the injured knee in full extension, and the heel resting on the examination table, the examiner places a closed fist under the proximal third of the calf at the level of the tibial tubercle to act as a fulcrum. 38 With the other hand, the examiner pushes in an anterior-to-posterior direction on the distal third of the quadriceps muscle. If the ACL is intact, it will counteract the downward gravitational force on the foot, and the heel will rise off the examination table (negative result) (Figure 1A). If the ACL is not intact, it cannot counteract the gravitational force, and the heel will stay on the examination table as the tibia slides anteriorly on the femur (positive result) (Figure 1B).

Diagrams illustrating the lever sign test. (A) With an intact anterior cruciate ligament (ACL) (negative test finding), the patient’s heel comes off the examination table. (B) With a nonintact ACL (positive test finding), the patient’s heel remains on the table. Adapted from Lelli et al 19 (used with permission).
Statistical Analysis
Descriptive statistics were used to evaluate our patient cohorts. The validity of the examination maneuvers was assessed by calculating the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The accuracy, defined as the proportion of true positive plus true negative findings for all results, was also calculated for each of the 4 examination maneuvers. Statistical analyses were performed with SPSS statistical software (SPSS Inc). Groups were divided on the basis of nonsurgical versus surgical cohorts (ie, awake vs under anesthesia, respectively), level of the tester (ie, undergraduate student/medical student vs orthopaedic resident/orthopaedic fellow), and sex of the patient. The chi-square test was used to compare the sensitivity and specificity of the various maneuvers. P < .05 was considered statistically significant.
Results
Patient Demographics
Overall, 102 consecutive symptomatic knees in 102 patients met the inclusion criteria and were included in the study. In the final cohort, 44 patients were female (43%) and 58 were male (57%), with a mean age of 23 years (range, 15-66 years) at the initial clinic visit. There were 50 left knees (49%) and 52 right knees (51%). The nonsurgical group included 48 patients (47%; 16 female, 32 male), and 54 patients (53%; 28 female, 26 male) were treated surgically (Figure 2). Of these 54 patients, surgery was initiated in 29 to address an ACL tear, which was confirmed by direct arthroscopic visualization and was reconstructed; the other 25 surgical patients had a normal ACL but other surgical abnormalities, and the appropriate non-ACL arthroscopic procedures were performed at the time of diagnostic arthroscopic surgery. Of the 29 patients who underwent ACL reconstruction, 2 had an isolated ACL injury, and 27 had associated injuries that required additional surgical procedures. In the nonsurgical group, MRI showed no acute meniscal, chondral, or ligament pathological processes in 33 patients; results showed the ACL to not be intact in 15 patients (Figure 2). As mentioned above, these patients were kept in the nonsurgical group to minimize bias by including those with surgical abnormalities in the nonsurgical group.

Patient flow diagram. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Clinical Diagnostic Tests
In the surgical group, MRI, our reference standard, was compared with direct arthroscopic visualization, the accepted diagnostic standard. MRI was found to have 97% sensitivity, 100% specificity, 100% PPV, 96% NPV, and 98% accuracy (Figure 3) for detecting ACL tears. MRI of 1 patient did not reveal a torn ACL, but direct arthroscopic visualization confirmed a tear. Clinically, the anterior drawer, Lachman, and lever sign test findings were positive for this patient; the pivot-shift test finding was negative.

2 × 2 contingency table. Comparison of findings from magnetic resonance imaging (MRI), our reference standard, with those of arthroscopic surgery, the diagnostic standard, for 54 surgical patients. ACL, anterior cruciate ligament.
For the lever sign test, the accuracy was similar in nonsurgical patients (awake in clinic, 76%) and in surgical patients (under anesthesia, 77%); the combined accuracy for all patients was 77% (Table 2). There were no statistically significant differences between the sensitivity or specificity of the test when performed in nonsurgical patients (awake) versus surgical patients (under anesthesia) (Table 3). Furthermore, the accuracy of the lever sign test when performed on female versus male patients (75% vs 79%, respectively) or when performed by undergraduate students/medical students versus orthopaedic residents/fellows (84% vs 88%, respectively) was similar. In this study, we did not statistically compare the accuracy, PPV, and NPV among our different populations because we did not stratify the prevalence of ACL tears in our population.
Parameters of Lever Sign Test: Predictive Values and Accuracy a
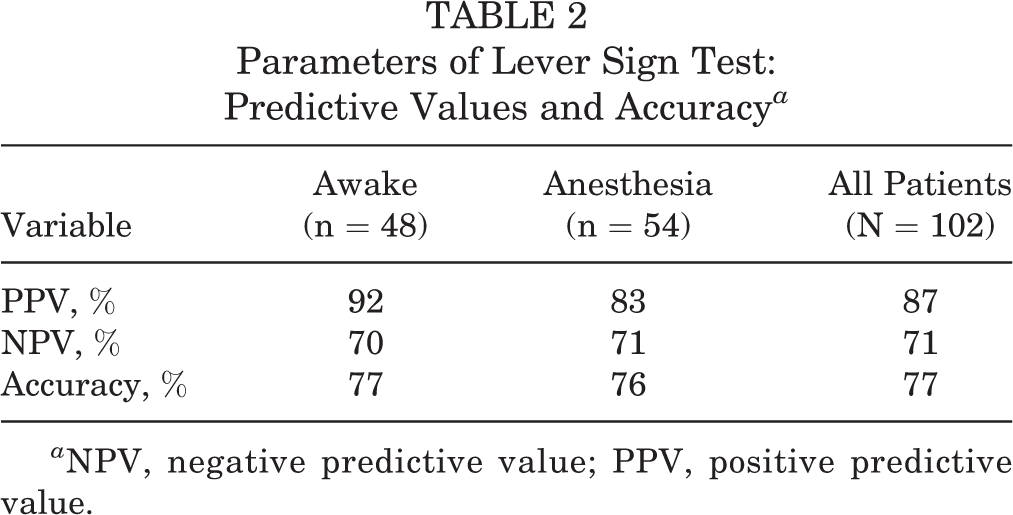
a NPV, negative predictive value; PPV, positive predictive value.
Parameters of Lever Sign Test: Sensitivity and Specificity

The sensitivity and specificity, in addition to the PPV and NPV, of the 4 physical examination maneuvers to test ACL integrity compared with MRI are shown in Table 4. In our cohort, the sensitivity was highest for the Lachman test (90%), followed by the anterior drawer (88%), lever sign (63%), and pivot-shift (59%) tests. The specificity was highest for the pivot-shift test (98%), followed by the Lachman (96%), anterior drawer (94%), and lever sign (90%) tests. The accuracy was highest for the Lachman test (93%) and lowest for the lever sign test (77%) (Table 4). In addition, in our cohort, we evaluated the accuracy of each examination test when performed under anesthesia versus awake compared with the MRI reference standard (Table 5).
Parameters of All Tests Versus MRI as Reference Standard a

a MRI, magnetic resonance imaging; NPV, negative predictive value; PPV, positive predictive value.
Accuracy of All Tests Versus MRI as Reference Standard a

a MRI, magnetic resonance imaging.
Discussion
No studies in the literature have assessed the lever sign test in different care settings, when performed by providers of different training levels, or when performed on male versus female patients. In the present study, the lever sign test was performed by different providers in all surgical patients under anesthesia and in all nonsurgical patients awake and was compared with MRI, the reference standard. No significant differences were found between the sensitivity or specificity of the test when performed in these different settings and by different providers. However, in our entire patient population, the sensitivity of the lever sign test (63%), as well as the pivot-shift test (59%), was low.
Historically, the Lachman test has been the most accurate and reliable for diagnosing an ACL rupture, 22 and the pivot-shift test is notably thought of as the least sensitive of the three. 8,9,14,17,23 Previous studies 7,19 have demonstrated the lever sign test to be more sensitive in correctly diagnosing both acute and chronic ACL tears, as well as complete and partial ACL tears, as compared with the anterior drawer, Lachman, and pivot-shift tests. This study, however, demonstrated the lever sign test to be less accurate than the Lachman test and slightly more sensitive than the pivot-shift test. In this investigation, administering the lever sign test did not rely on the strength of the examiner or the size of the patient; a provider with small hands can easily and effectively perform this test on a patient with a large leg, an advantage that no other test can offer. As demonstrated by the lack of significant differences between different levels of testers, this test can be an effective and useful clinical examination maneuver for physicians across different specialties, as well as for providers with different training backgrounds, to aid in the clinical diagnosis of an ACL tear.
Three studies have assessed the sensitivity of the lever sign test in relation to the other 3 clinical diagnostic tests. 7,19,33 The first study, published by Lelli and colleagues, 19 was the first to describe and assess the lever sign. The authors divided 400 patients into 4 equal-sized groups based on the time elapsed from the injury (acute [<20 days] or chronic [≥20 days] from injury) and MRI findings (complete or partial ACL rupture). The 4 tests were compared with MRI and found to be nearly 100% sensitive in patients with chronic, complete ACL tears. In patients with acute, partial tears, only the lever sign test was 100% sensitive; the anterior drawer, Lachman, and pivot-shift tests had sensitivities of 29%, 42%, and 11%, respectively. In addition, the lever sign test was performed on the contralateral noninjured leg of all patients and found to have 100% specificity (no false-positive findings); however, this result was not confirmed with MRI or arthroscopic surgery.
The second study, by Thapa and colleagues, 33 included 80 patients with knee concerns after an injury. The 4 physical examination maneuvers were performed on all patients and compared with arthroscopic surgery, the diagnostic standard. The sensitivity was 80% for the anterior drawer test, 91% for the Lachman test, 51% for the pivot-shift test, and 86% for the lever sign test. The authors concluded that the lever sign test can be used routinely in the evaluation of ACL function in both acute and chronic knee injuries; however, it is important to note that the time from injury to evaluation was not mentioned in this study.
The most recent study, by Deveci and colleagues, 7 included 117 patients with an arthroscopic diagnosis of a chronic (≥4 weeks between trauma and surgery) ACL tear (further specified as complete or partial). All patients underwent the 4 clinical examination maneuvers both preoperatively and under anesthesia. Preanesthesia and postanesthesia sensitivities were 60% and 88%, respectively, for the anterior drawer test; 80% and 88%, respectively, for the Lachman test; 62% and 88%, respectively, for the pivot-shift test; and 94% and 98%, respectively, for the lever sign test. The authors concluded that the lever sign test can be easily applied clinically and seems to have a higher sensitivity than the classic Lachman test.
The lever sign test is intriguing, but some inherent limitations must be examined. First, there is no validated biomechanical explanation of the pathomechanics of the lever sign test. Dr Lelli proposed that an intact ACL enables the leg to act as a complete lever, allowing the applied downward force on the distal femur to offset the force of gravity acting on the foot and lower leg, and results in knee extension and heel rise off the examination table. An insufficient ACL is unable to offset the force of gravity on the lower leg, allowing the tibial plateau to slide anterior to the femoral condyles, and results in gravity pulling the heel down to the examination table. 19 However, there are no biomechanical studies on this proposed mechanism, and furthermore, there is no reference in the literature to this mechanism. Conversely, the biomechanics of the anterior drawer, Lachman, and pivot-shift tests have been extensively studied and debated. 3,14,25,27,32
Second, the limited literature on the lever sign test has failed to adequately address its diagnostic accuracy with regard to 2 important features of a suspected ACL tear: chronicity and type of tear (complete or partial). The chronicity of a tear, which may allow the ACL to scar down to the posterior cruciate ligament, may alter the diagnostic results of this test. 4,37 To date, only Lelli and colleagues 19 have evaluated and compared the lever sign test in acute and chronic settings, reporting no difference in the sensitivity of the test. The type of tear, complete or partial, is hard to distinguish solely by physical examination maneuvers; the anterior drawer, Lachman, and pivot-shift tests have been shown to be falsely normal in the setting of a partial tear. 6,15,20,39 The lever sign test was developed, in part, to try to address this shortcoming. However, aside from the study by Lelli and colleagues, 19 an analysis of the sensitivity of the lever sign test in relation to complete or partial tears has not been performed. Deveci and colleagues 7 did not report the outcomes of the lever sign test specifically with regard to complete versus partial tears. Furthermore, the lever sign test, similar to the anterior drawer and Lachman tests, uses pure translational displacement as its assessment method and does not assess the rotational component, which may lead to a missed diagnosis in a partial tear. 6,15,20,39
In our study, the lever sign test was easy to learn and carry out. The examination technique avoids rapid motion of the injured knee, thereby minimizing additional pain and inhibition. There was no difference in the results of the test when performed by undergraduate students and medical students versus orthopaedic residents and fellows, who were all blinded to the diagnosis. The test, therefore, can be performed by providers of various specialties and different training levels, which facilitates the opportunity to reach an appropriate and timely diagnosis. Although the results of our study did not approach the 100% sensitivity and specificity initially reported in the literature, we found that the lever sign test is easy to reproduce, regardless of training levels and independent of patient size. Additionally, the test is not affected by anesthesia, which cannot be stated for other ACL examinations. 30,34 Our study used prospective data collection and was adequately powered, which further strengthened it.
There were several limitations to this study. First, the examiners were only blinded to the diagnosis, not to the side of injury or the obtained clinical history. Second, the lever sign test was only performed on the injured side, with no comparison to the healthy leg. Third, in the surgical patients who underwent ACL reconstruction, we did not distinguish between partial and complete tears. Fourth, although several providers of various training levels performed the clinical examinations, we did not conduct interobserver or intraobserver analyses.
The lever sign test has inherent limitations that must be examined further, including a validated biomechanical explanation of the test and its application in the settings of ACL tears, multiligament knee injuries, and pre-existing ligamentous laxity. Among our patient population, the lever sign test was highly specific (90%) for diagnosing an insufficient ACL, but its sensitivity was only 63%. These statistics coincide with the high specificity and low sensitivity of the pivot-shift test that have been reported in the literature. 31,32 The results of our study challenge the exceptional sensitivity and specificity values of the lever sign test as reported by Lelli and colleagues. 19 Future studies must focus on the biomechanical explanation of the lever sign test and its application in the settings of complete ACL tears, partial ACL tears, and multiligament knee injuries. Finally, the lever sign test should be further evaluated by providers across all clinical settings.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Mayo Clinic Institutional Review Board (application No. 16-004428).