
Abstract
Background:
Until recently, anterior cruciate ligament (ACL) tears in older patients were treated conservatively; however, these patients often experienced significant pain and instability.
Purpose/Hypothesis:
The purpose of this study was to compare the patient-reported outcomes, patient satisfaction, and failure rates of primary ACL reconstruction between a younger (age 20-30 years) and older (age 50-75 years) patient cohort. It was hypothesized that patients in the older cohort could achieve comparable clinical outcomes and retear rates following ACL reconstruction with a bone-tendon-bone autograft or allograft compared with the younger patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective analysis of prospectively collected data was performed. All patients undergoing a primary ACL reconstruction between 2010 and 2014 by a single surgeon were collated. Patients were divided into 2 groups based on age at the time of surgery: a younger cohort (20-30 years) and an older cohort (50-75 years). Patients were excluded if they were outside the desired age intervals; had revision ACL reconstructions; had a previous intra-articular infection in the ipsilateral knee; underwent prior alignment correction procedure, cartilage repair, or transplant procedure; had a concurrent posterior cruciate ligament tear; received meniscal allograft transplant; or had an intra-articular fracture. Subjective outcome scores (Tegner activity scale, Lysholm, International Knee Documentation Committee [IKDC], Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC], Short Form–12 [SF-12] mental health component summary [MCS], and SF-12 physical component summary [PCS]), retear rate, and rate of secondary arthrofibrosis surgery were documented at a minimum 2-year follow-up and were compared between groups.
Results:
A total of 85 patients met the inclusion criteria for this study: 52 patients (33 males, 19 females) in the younger cohort and 33 patients (14 males, 19 females) in the older cohort. No significant differences were found in any demographic factor except for age. Significant improvement in outcome scores from pre- to postoperative assessments was found in both groups. The younger cohort had significantly lower postoperative WOMAC scores (P = .025). However, no significant differences were found between the younger and older cohorts in postoperative SF-12 PCS (P = .487), SF-12 MCS (P = .900), Lysholm score (P = .660), IKDC score (P = .256), Tegner activity score (P = .420), or patient satisfaction (P = .060). Within the older cohort, increasing age did not correlate with inferior postoperative outcome scores. Furthermore, no retears occurred in either group, and the rates of arthrofibrosis surgery were comparable (12% older cohort vs 13% younger cohort).
Conclusion:
Improved function and satisfaction, comparable to the younger age group, were achieved in patients older than 50 years undergoing ACL reconstruction. Furthermore, low failure rates can be achieved in both younger and older patients undergoing ACL reconstruction.
Musculoskeletal disorders are a common, disabling condition in the elderly population, affecting 14% of people older than 65 years. 21 The population of individuals older than 65 years is expected to increase to more than 80 million by the year 2050. 12 A recent survey of 1000 respondents aged 65 years or older from the Associated Retirement Community Operators showed that 70% of individuals desired to be more active. Given the growing elderly population and the proportion of elderly people who want to remain active, the incidence of anterior cruciate ligament (ACL) tears is expected to increase in this population.
Although ACL reconstruction in older patients is controversial, a recent systematic review suggested that this procedure can be recommended for individuals older than 40 years who intend to maintain an active lifestyle or to address symptomatic instability with daily activities. 19 Moreover, ACL reconstruction has been demonstrated to result in greater improvements in quality-adjusted life-years at a lower cost compared with nonoperative intervention. 20 With the advent of an anatomic surgical technique, the availability of enhanced instrumentation, the use of an improved and more aggressive rehabilitation protocol, and a better understanding of the immediate and long-term consequences of untreated knee instability, surgical indications for ACL insufficiency have been extended to active patients of all ages. 29
Previous studies have compared outcomes in patients older than 40 years versus a control group (<25 years); however, there are many in the fourth decade of life who are not considered old, who desire to remain active, and are good candidates for ACL reconstruction. Both the cutoff age for ACL reconstruction and the treatment of ACL tears in patients older than 50 years are controversial. While studies have investigated ACL reconstruction in patients older than 50, 3,9,13,30 to our knowledge no study has compared outcomes between a control group of young patients and patients aged 50 years and older. Therefore, the purpose of this study was to compare the clinical outcomes and failure rates in patients aged 20 to 30 years with those of patients aged 50 to 75 years at the time of primary ACL reconstruction. It was hypothesized that patients in the older cohort (50-75 years) would achieve comparable clinical outcomes and failure rates following ACL reconstruction with a bone-tendon-bone autograft or allograft compared with younger patients (20-30 years).
Methods
Study Design
This study was approved by the institutional review board at our institution (IRB No. 2002-03). This was a retrospective study of prospectively collected data. Patients were included in this study if they were between 20 and 30 years or 50 and 75 years of age at the time of primary ACL reconstruction between 2010 and 2015 by a single surgeon (R.F.L.). These age ranges were selected based on (1) age stratification in a previous large ACL registry study, 10 (2) literature reporting on younger patients after ACL reconstruction, 24,27,28 (3) current literature reporting outcomes in older patients after ACL reconstruction, 1,3 and (4) age ranges of the control group in a previously published study. 15 Patients were required to have a minimum 2 years of follow-up for inclusion.
Patients were excluded from this study if they were outside either the 20- to 30-year or 50- to 75-year age range at the time of surgery; had a previous intra-articular infection in the ipsilateral knee; or had undergone a prior partial or complete meniscectomy, cartilage repair or transplant procedure, meniscal allograft transplantation, or intra-articular fracture. Patients were not excluded based on the number of concomitant ligament reconstructions during the primary ACL reconstruction procedure. However, revision ACL reconstruction cases were excluded.
Patient-Reported Outcomes, Patient Satisfaction, and Failure Rates
At a minimum 2 years after the index surgery, patients were administered a subjective questionnaire, which included the following clinical outcome measures: Lysholm score, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, the International Knee Documentation Committee (IKDC) score, the Short Form–12 (SF-12) physical component summary (PCS) and mental health component summary (MCS), the Tegner activity scale, and patient satisfaction with outcome. Patient satisfaction was measured on a 1 to 10 scale, with 10 being very satisfied and 1 being very unsatisfied. Demographic characteristics were also recorded, including age, sex, body mass index (BMI), previous surgery, concomitant ligament injuries, and concomitant intra-articular injuries. Failure was defined as any subsequent ligament surgery for graft failure or arthrofibrosis, which was defined as any reconstruction that required an additional lysis of adhesions procedure.
Surgical Technique
All patients underwent anatomic, single-bundle, primary ACL reconstruction via a previously described and biomechanically validated technique. 16 The patient was placed in the supine position on the operating table. A bone–patellar tendon–bone (BPTB) autograft was chosen for all patients younger than 50 years with an intact patellar tendon; an ipsilateral or contralateral BPTB autograft was the graft of choice. A BPTB allograft was considered for patients aged 50 years and older or for any patient with an insufficient ipsilateral or contralateral patellar tendon. 5,14,17,26 Next, standard anterolateral and anteromedial portals were created. The stump of the native ACL was used as the most reliable landmark for anatomic reconstruction. In cases of chronic reconstructions, the resident’s ridge was used as the anterior margin of the tunnel, which was created with a 10-mm-diameter reamer to a depth of 25 mm. Then, the tibial ACL attachment was identified, and an ACL aiming guide was positioned in line with the center of the anterior horn of the lateral meniscus. The tibial tunnel was then reamed (10 mm), and the tunnel aperture was cleared of remaining soft tissue. The graft was pulled until the lateral wall of the tunnel was met with the bone plug. The femoral ACL reconstruction tunnel was drilled through the anteromedial portal in all patients. Femoral fixation of the ACL graft was performed with the patient’s knee in maximal flexion. A guide pin was inserted along the superior aspect of the graft through the accessory medial portal with visualization from the anterolateral portal. A 7 × 20–mm cannulated titanium interference screw was then placed under arthroscopic visualization. Tibial fixation of the ACL graft was performed with a 9 × 20–mm cannulated titanium interference screw with the knee fully extended and the joint reduced. Excess bone from the BPTB autograft that was saved during graft preparation was used as bone graft at the patellar and tibial harvest sites.
Rehabilitation
All patients were allowed to bear weight as tolerated upon discharge and were told to use crutches until they could ambulate without a limp, which was usually for the first 2 weeks. Physical therapy commenced within 24 hours after surgery to initiate early range of motion (ROM) and muscle reactivation and to control edema. Rehabilitation included straight-leg raises, which were performed in an immobilizer until the patient was able to perform them without any extension sag. It was anticipated that patients would not return to full activities until 7 to 9 months postoperatively.
Statistical Analysis
Data were tested for normal distribution by use of the Kolmogorov-Smirnov Z test. For preoperative and postoperative comparisons of dependent variables, the paired-samples t test was used for normally distributed data and the Wilcoxon signed-rank test was used for nonnormally distributed data. SF-12 PCS and SF-12 MCS preoperative and postoperative scores in each of the meniscal cohorts (medial, lateral, or both) were analyzed, and analysis of variance (ANOVA) was performed. Lysholm, Tegner, and WOMAC preoperative and postoperative scores in each meniscal cohort were analyzed with a Kruskal-Wallis test. Comparisons of categorical data, including age, sex, and BMI, were performed by use of chi-square tests and Fisher exact tests. Correlation analysis was performed with Spearman correlation coefficients. Assuming 2-tailed testing, alpha of .05, and an independent-groups t test, 32 patients per group were sufficient to detect an effect size of d = 0.72 with 80% statistical power. All statistical analyses were performed by use of SPSS version 9.4 (IBM Corp).
Results
Demographics and Concomitant Injuries
Initial database query returned 100 patients who met inclusion criteria. Of these 100 patients, 85 (85%) patients had complete follow-up at a minimum of 2 years after surgery. Fifty-two were included in the 20- to 30-year age cohort, and 33 patients were included in the 50- to 75-year cohort. Mean follow-up was 3.4 years for the younger cohort and 3.1 years for the older cohort. Preoperatively, there were no significant differences between concomitant injury patterns for the 2 cohorts. The older cohort had significantly higher preoperative SF-12 PCS compared with the younger cohort (P = .025). Of note, a concomitant collateral ligament reconstruction (superficial medial collateral ligament or fibular collateral ligament) was performed in both ACL reconstruction cohorts, with a combined procedure reported in 38% of the younger patients and 36% of the older patients. Arthrofibrosis was not observed in any of the isolated ACL reconstructions. Detailed demographic and concomitant pathology data are reported in Table 1.
Demographic Data and Preoperative Outcome Scores for Study Cohorts a

a ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; FCL, fibular collateral ligament; IKDC, International Knee Documentation Committee; MCL, medial collateral ligament; MCS, mental health component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Reported as mean values.
c Represents the P value for the comparison between the numbers of Outerbridge 3-4 lesions in both cohorts.
d Represents the P value for the comparison between the rate of meniscal repair versus meniscectomy between the 2 cohorts.
Postoperative Objective and Outcome Scores Cohort Comparison
All patient-reported outcome scores, with the exception of the IKDC score, improved from preoperative to postoperative status in both cohorts (P < .001). The younger cohort had a significantly lower WOMAC score compared with the older cohort at postoperative status. The mean postoperative ROM was –1° to 133° (range, –5° to 135°) in the younger cohort and –0.8° to 132° (range, –4° to 135°) in the older cohort (P = .657). Detailed postoperative outcome score information is reported in Table 2.
Postoperative Outcome Scores for Study Cohorts a

a Individual outcome scores are reported as mean values. IKDC, International Knee Documentation Committee; MCS, mental health component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Older Cohort Correlation Analysis
A Spearman rank-order analysis was performed to characterize the relationship between increasing age and postoperative outcome scores in the older cohort. No significant correlation was found between increased age and postoperative outcome scores. Detailed correlation information is reported in Table 3.
Result of Correlation Analysis for Increasing Age and Postoperative Outcome Scores in the Older Cohort a
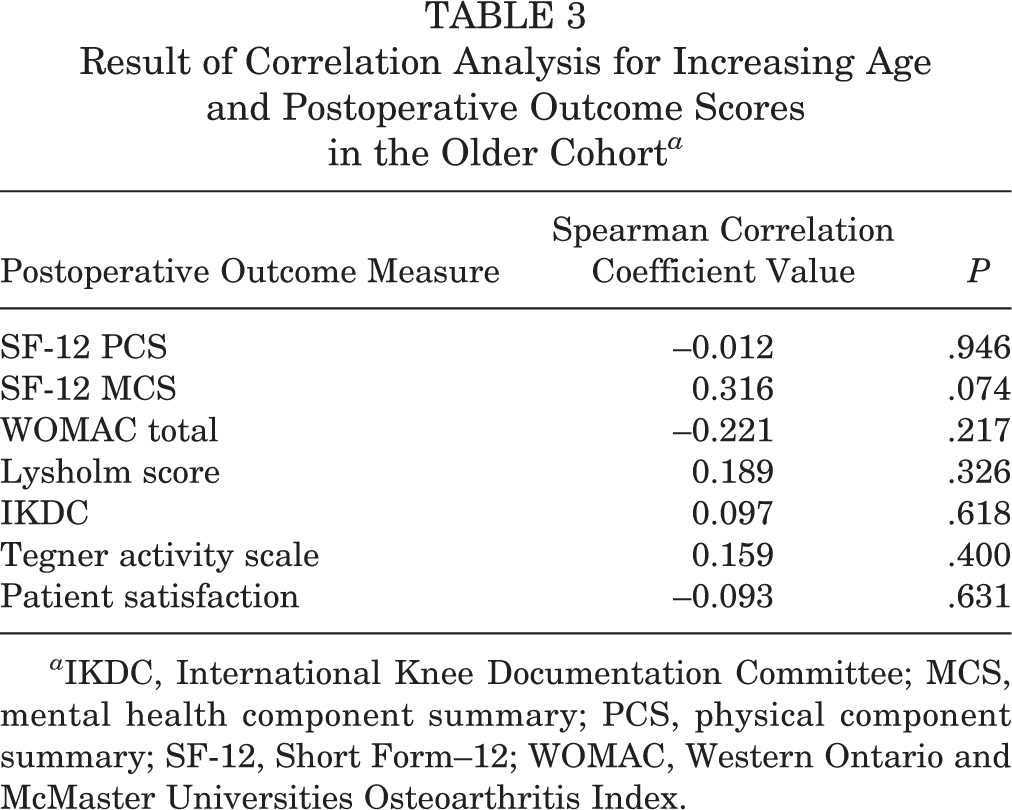
a IKDC, International Knee Documentation Committee; MCS, mental health component summary; PCS, physical component summary; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Discussion
The most important finding of this study was that comparable improvements in outcomes were achieved after anatomic, single-bundle, primary ACL reconstruction with biomechanically validated, anatomically based techniques in both the younger (20-30 years) and older (50-70 years) patient cohorts. 16 Furthermore, satisfaction in both groups was comparable, with a tendency for higher satisfaction in the older group compared with the younger group. Both the younger and older populations had improved outcome scores compared with preoperative scores. In the present study, all patients had a similar postoperative protocol, and no difference was found in the rate of arthrofibrosis requiring additional surgery.
The study included 33 patients older than 50 years who were surgically treated for symptomatic ACL tears. The preoperative Lysholm score was 49.6, which is defined as poor, and it improved to 84.4 (good) postoperatively. Furthermore, the other outcome scores (Tegner, WOMAC) significantly improved postoperatively. Historically, ACL reconstruction has been recommended for the young, active population with symptomatic ACL tears. Other authors 19,25 have advocated for ACL reconstruction to prevent meniscal and cartilage injuries in chronically unstable knees, both of which are associated with poor function and rapid progression of knee degenerative changes. The treatment of ACL tears in the elderly population is still controversial. Most of the elderly patients who sustained ACL tears modified their activities to be able to function. 7 Some orthopaedic surgeons are concerned with the risk of arthrofibrosis in elderly patients. Furthermore, the high prevalence of degenerative changes can result in poorer outcomes. 8,23,25 Another area of concern in the elderly population is bone quality and the healing response, which can affect graft incorporation and healing potential. 6,11
In the present study, 50 to 75 years was chosen as the cutoff age for the older cohort, and 20 to 30 years was chosen as the younger cohort. Most authors agree that symptomatic patients in the 20- to 30-year age group should be treated surgically. The cutoff age is still controversial, given that patients in their 40s are no longer categorized as “old.” The literature on ACL reconstruction in elderly patients is still lacking. Several studies have evaluated functional outcomes in patients 40 years and older. 2,4,7,18 Few studies have evaluated outcomes after ACL reconstruction in patients 50 years and older. 3,9,13,22,29,30 Blyth et al 3 reported improved outcomes in patients older than 50 years after ACL reconstruction with a follow-up of 2 to 8 years. The Lysholm score improved from 63 to 93, Cincinnati score from 49 to 89, Tegner activity scale from 3.7 to 5.2, and the IKDC score was normal or nearly normal in 25 knees (81%). The authors reported poorer outcomes in patients with advanced articular degenerative changes (Outerbridge grade 3 or 4). Even though the postoperative Lysholm score of 93 reported by Blyth et al 3 was higher than the one in this study (85), Lysholm scores between 84 to 94 are interpreted as “good” outcomes. Baker et al 1 recently reported improved outcomes in patients over 60 years of age after ACL reconstruction at a mean follow-up of 115.7 months.
This study is not without limitations. This was a retrospective study and carries limitations inherent to retrospective studies. Furthermore, the sample size was small, which limits the generalizability of the finding. It is possible that a selection bias occurred with regard to which older patients underwent an ACL reconstruction. Additionally, the discrepancy in male-to-female ratios between the groups made comparisons of outcomes between the younger and older cohorts challenging. The majority of patients in the younger cohort were males (63%) while the majority of patients in the older cohort were females (58%). However, we found no significant difference when comparing sample sizes among sexes (P = .074). The majority of patients in the younger cohort received an autograft for their ACL reconstruction, which may have affected postoperative activity level and outcome scores. Finally, all surgeries were performed by a single experienced surgeon in a tertiary referral center, and these results might therefore not be generalized to the general population.
Conclusion
Improved function and satisfaction, comparable to results of the younger age group, were achieved in patients older than 50 years undergoing ACL reconstruction. Furthermore, it was found that low failure rates can be achieved in both younger and older patients undergoing ACL reconstruction.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. receives royalties from Arthrex and Smith & Nephew; is a paid consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Smith & Nephew, Ossur, and Linvatec.
Ethical approval for this study was obtained from Vail Valley Medical Center (protocol No. 2002-03).