
Abstract
Background:
There is no universally accepted definition of “contact” or “collision” sports in the literature. The few available studies evaluating contact and collision sports consider them to be synonymous. However, athletes in collision sports purposely hit or collide with each other or with inanimate objects with greater force and frequency than in contact sports, which could jeopardize functional outcomes.
Purpose:
To compare the functional outcomes, return to sports, and recurrences in a series of contact and collision athletes with a first-time anterior shoulder dislocation treated using arthroscopic stabilization with suture anchors.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 56 athletes were enrolled in this study, including 22 contact athletes and 34 collision athletes. All athletes underwent arthroscopic shoulder stabilization using suture anchors. Range of motion, the Rowe score, a visual analog scale (VAS) for pain, and the Athletic Shoulder Outcome Scoring System (ASOSS) were used to assess functional outcomes. Return to sports and recurrences were also evaluated.
Results:
The mean age at the time of surgery was 22.2 years, and the mean follow-up was 62.4 months (range, 36-94 months). No significant difference in shoulder motion was found between preoperative and postoperative results or between the contact and collision groups. The Rowe, VAS, and ASOSS scores showed statistical improvement in both groups after surgery (P = .001). Patients in the contact group returned to sports significantly faster than those in the collision group (5.2 vs 6.9 months, respectively; P = .01). In all, 43 athletes (76.8%) returned to near-preinjury sports activity levels (≥90% recovery) after surgery: 86.4% of patients in the contact group and 70.6% in the collision group (P = .04). The total recurrence rate was 8.9%. There were 5 recurrences (14.7%) in the collision group and no recurrences in the contact group (P < .01).
Conclusion:
Arthroscopic stabilization for anterior instability of the shoulder is a reliable procedure with respect to shoulder function, range of motion, and postoperative return to sports in contact and collision athletes. Compared with the contact group (0%), the collision group yielded a higher failure rate (14.7%). Moreover, patients in the contact group returned significantly faster (5.2 vs 6.9 months, respectively) and to and more returned to preinjury or near-preinjury activity levels (86.4% vs 70.6% of patients, respectively) than patients in the collision group.
The glenohumeral joint is the most commonly dislocated articulation in the body. The overall incidence of dislocations is 2.39 per 1000 person-years in the general population presenting to emergency departments. 28 Contact and collision sports, such as American football, ice hockey, and rugby, are associated with the highest risk for shoulder instability. 8,10–12,19 Sachs et al, 25 in a prospective study of 131 patients with a first-time dislocation, reported that 86% of patients with a recurrence were contact or collision athletes.
There is no universally accepted definition of “contact” or “collision” sports in the literature. The most widely used classification is the one from the American Academy of Pediatrics Committee on Sports Medicine. 23 In this classification, sports are categorized as contact, limited contact, or noncontact according to the relative risk of an acute injury to the athlete during the competition. However, there is no clear dividing line between the 3 groups, and many sports with very different risks are categorized in the same group.
As a solution to this problem, Rice 23 proposed categorizing the risk by subdividing contact sports into contact and collision sports. In collision sports (eg, rugby, boxing, ice hockey, American football), athletes purposely hit or collide with each other or with inanimate objects (including the ground) with great force. In contact sports (eg, basketball and soccer), athletes routinely make contact with each other or with inanimate objects but usually with less force than in collision sports. However, the few available studies evaluating contact and collision sports consider them to be synonymous. 1–3,5,7,9,20,22
The purpose of this study was to compare the functional outcomes, return to sports, and recurrences in a series of contact and collision athletes with a first-time anterior shoulder dislocation treated with arthroscopic stabilization using suture anchors. The hypothesis of this study was that because of the higher risk of collision sports to the shoulder, functional outcomes, return to sports, and recurrences would be different between contact and collision sports.
Methods
Patient Selection
Between June 2008 and June 2013, 56 athletes (56 shoulders) who participated in contact or collision sports underwent arthroscopic shoulder stabilization after an acute traumatic first-time glenohumeral dislocation at our institution. The inclusion criteria for this study were patients younger than 30 years, a minimum follow-up period of 36 months, only 1 episode of a frank dislocation (defined as a dislocation that required reduction), and a competitive sports level (regular sports with competitions and practices at least 2 times/wk). 26 All patients participated in contact or collision sports according to the definition given by Rice. 23
Exclusion criteria were large bony Bankart lesions (bony defects of >25% on the anteroinferior portion of the glenoid), engaging Hill-Sachs lesions, humeral avulsion of the glenohumeral ligament (HAGL) lesions, associated superior labral from anterior to posterior (SLAP) lesions, posterior labral tears, rotator cuff injuries, or previous surgery on the same shoulder. We also excluded athletes who participated in martial arts because we believed that martial arts should be considered as a separate group. Many of the maneuvers used during the fights expose the glenohumeral joint to the maximum of its capacity, which could not only compromise return to the sport but also have an impact on the percentage of recurrences.
The study protocol was approved by the local ethics committee (No. 3055), and all patients provided written informed consent to participate in this investigation.
Evaluation
Preoperative and postoperative evaluations consisted of a patient-based questionnaire and a physical examination performed by a resident or a shoulder fellow who did not participate in the surgical procedure. Active and passive shoulder motion, including forward flexion, external rotation at the side, and internal rotation to the back, were measured preoperatively and at last follow-up. Instability was evaluated with apprehension and relocation tests.
Radiography and magnetic resonance imaging were performed in all cases. If, during these studies, bony defects were suspected, computed tomography was ordered to evaluate the magnitude.
The Rowe score was used as a global outcome measure. 24 Additionally, a visual analog scale (VAS) was used to assess “pain while performing shoulder sports” (ranging from a maximal score of 10 to a minimum of 0).
Shoulder-dependent sports ability was measured by a 6-item questionnaire: the Athletic Shoulder Outcome Scoring System (ASOSS). 17 This score measures subjective sports-specific perception of pain, instability, muscular strength and endurance, intensity, and proficiency level, with each point graduated and compared with the time before injury (defined as 100%). Range of motion was objectively recorded and compared with that in the untreated shoulder. 17 Patients were contacted by telephone and then examined at a minimum follow-up of 36 months. Patients were also asked if they had been able to practice their previous sports and if they had been able to perform them at the same level as before the dislocation. According to Cho et al, 3 we divided the levels of postoperative sports activity into 5 grades: 1, complete return to preinjury activity level; 2, near return to preinjury activity level (≥90% recovery); 3, return to preinjury activity with moderate limitations (≥70% recovery); 4, return to preinjury activity with severe limitations or inability to return to preinjury activity but without any discomfort or pain in the shoulder during daily activities of living (≥50% recovery); and 5, inability to return to preinjury activity with discomfort or pain in the shoulder during daily activities of living. All surgery-related complications and reoperations were documented.
Surgical Technique
The patient was placed in the lateral decubitus position. The arm was abducted 60° to 70° with forearm traction of 10 to 15 kg. We used a standard posterior portal with 2 anterior portals, and flow of irrigation was maintained by an arthroscopic pump (40-60 mm Hg). Looking from the posterior portal, we evaluated the relation of the Hill-Sachs lesion with the anterior glenoid, reproducing the dislocated shoulder position. Moreover, a final evaluation of the glenoid bone defect was performed intraoperatively. The labral edge was debrided after complete liberation and release of the capsulolabral ligament beyond the 6-o’clock position. Then, the anterior and inferior glenoid rim and neck were lightly abraded with a shaver. Typically, 3 anchors with No. 2 nonabsorbable sutures were placed on the cartilage edge of the glenoid surface. The first one was placed in the inferior area of the anterior glenoid rim below the 5-o’clock position. Additional anchors were placed in a similar manner at both the 3- and 4-o’clock positions. Capsular plication was performed, starting 1 hour inferior to the anchor placement and lateral depending on capsular laxity, between 5 and 15 mm, to create superior tensioning of the inferior glenohumeral ligament and eliminating inferior capsular redundancy. Once the sutures were placed in the correct position, they were secured with sliding knots.
Postoperative Rehabilitation
The arm was supported with a sling for 4 weeks. All patients followed a standard postoperative rehabilitation protocol supervised by one of the authors (L.A.R.). After 1 week, supervised gentle physical therapy consisting of passive pendulum and gradual passive range of motion exercises was begun. Active-assisted range of motion exercises were started 2 weeks after surgery. When the patient could perform active forward elevation above the shoulder level, usually at 4 to 6 weeks after surgery, shoulder-strengthening exercises were started. Rehabilitation continued for 3 months. Return to sports was allowed when the patient was pain free, full shoulder range of motion had been achieved, and shoulder strength was the same as before the injury, which usually occurred at 5 months in contact sports and at 7 months in collision sports.
Statistical Analysis
Statistical analysis was performed using the independent Student t test with 95% CIs to calculate the differences between the groups in range of motion and functional scores. The chi-square test with 95% CIs was used to calculate the difference between the recurrence rates in the 2 groups. Statistical analyses were performed using the software STATA version 12 (StataCorp). A P value <.05 was considered statistically significant.
Results
The mean age of the 56 study patients at the time of surgery was 22.2 years (range, 18-30 years), and the mean follow-up period was 62.4 months (range, 36-94 months). No patient was lost to follow-up; thus, the analysis was made up of 56 patients. Patient demographic details for the contact and collision groups are summarized in Table 1.
Patient Demographics

Range of Motion and Functional Scores
No significant difference in shoulder range of motion was found between preoperative and postoperative results and between the collision and contact groups (Table 2). The Rowe, VAS, and ASOSS scores all showed statistical improvement after surgery (P = .001). Specifically, the mean Rowe score increased from 45.1 preoperatively to 90.6 (P = .001). The mean VAS score improved from 3.9 preoperatively to 1.6 at last follow-up (P = .001). No statistically significant difference was noted between the contact and collision groups in the postoperative Rowe or VAS score (Table 3). The mean ASOSS score improved significantly from 48.0 preoperatively to 82.5 (P = .001). However, the improvement was significantly more important in the contact group (from 66.9 to 91.9) than in the collision group (from 63.0 to 72.4) (P = .001).
Preoperative and Postoperative Range of Motion a

a Values are shown as mean or mean ± SD.
Preoperative and Postoperative Shoulder Scores a
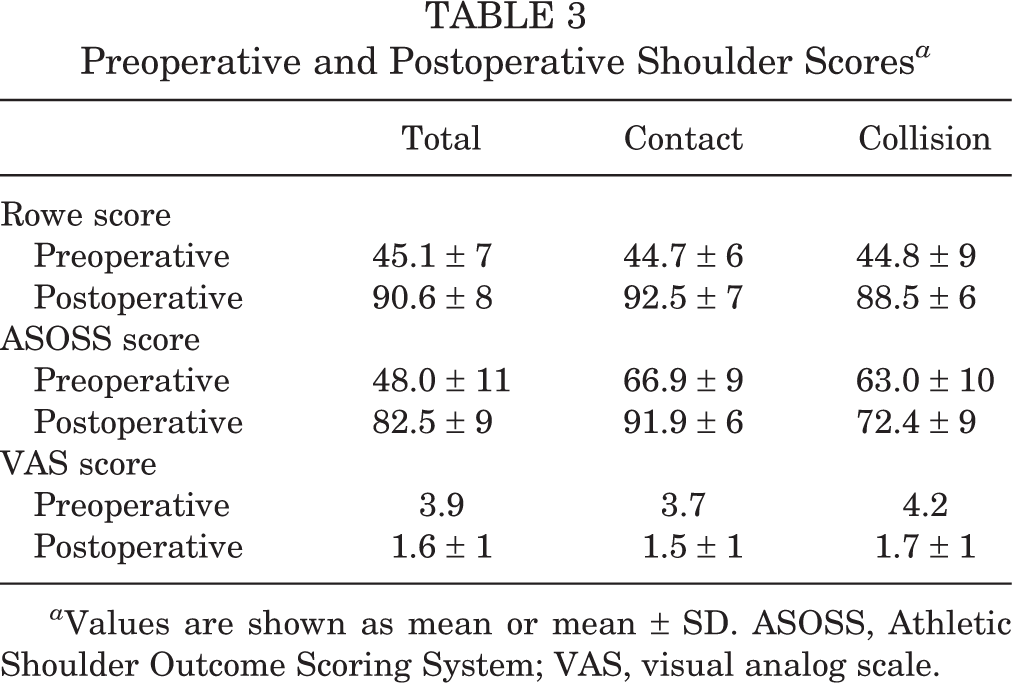
a Values are shown as mean or mean ± SD. ASOSS, Athletic Shoulder Outcome Scoring System; VAS, visual analog scale.
Return to Sports
The mean time to return to sports was 6.1 months. Patients in the contact group returned to sports significantly faster than those in the collision group: 5.2 versus 6.9 months, respectively (P = .01). In all, 43 athletes (76.8%) returned to near-preinjury sports activity levels (≥90% recovery) after surgery. Specifically, 86.4% (19/22) of patients in the contact group were rated as grade 1 or 2 and 70.6% (24/34) in the collision group (Table 4). This difference was statistically significant (P = .04).
Time to Return to Sports and Reachieved Preinjury Proficiency Level a

a Grade 1: complete return to preinjury activity level; grade 2: near-return to preinjury activity level; grade 3: return to preinjury activity with moderate limitations; grade 4: return to preinjury activity with severe limitations; and grade 5: inability to return to preinjury activity with discomfort during daily activities.
Complications and Postoperative Instability
No intraoperative complications or infections were reported in either group. The total recurrence rate was 8.9%. There were 5 recurrences (14.7%) in the collision group: 1 subluxation and 4 dislocations. There were no recurrences in the contact group. This difference was statistically significant (P = .001). Detailed information regarding recurrences is shown in Table 5.
Information Regarding Recurrences

Discussion
There were 3 main findings in the current study. First, there was an increased recurrence rate in collision athletes treated with arthroscopic Bankart repair compared with contact athletes. Second, significantly more patients in the contact group achieved preinjury or near-preinjury levels of competition compared with those in the collision group. Finally, patients in the contact group returned to sports significantly faster than those in the collision group.
Advances in arthroscopic techniques have led to the more common use of arthroscopic procedures for shoulder stabilization. Although initial rates of recurrent instability were reported to be higher with arthroscopic stabilization, 2 recent systematic reviews of long-term outcomes after open or arthroscopic Bankart shoulder stabilization showed no significant difference in recurrence of instability between the arthroscopic suture anchor (8.5%) and open (8%) techniques. 6,21 Furthermore, there was no significant difference in the rate of return to sports between the arthroscopic suture anchor (87%) and open (89%) techniques, and there was no significant difference in the rate of postoperative osteoarthritis between the arthroscopic suture anchor (26%) and open (33%) techniques. 6,21
Previous authors have published similar results regarding recurrence rates after arthroscopic stabilization in collision athletes, ranging between 6.5% and 58%. 1,2,9,13,15,22 However, clinical reports so far have focused only on a heterogeneous group of collision and contact athletes, with dissimilar levels of competition, varied number of previous dislocations, and diverse ages. 14 Only a few articles have concentrated on the high-risk subgroup of athletes who participate in contact or collision sports at a competitive level. 14 Furthermore, no previous investigation has directly compared the results of arthroscopic stabilization between contact and collision athletes. Because of the high recurrence rate with the arthroscopic treatment of collision athletes, some authors have advocated for open procedures in this population. Neyton et al 18 retrospectively assessed 34 rugby players with recurrent anterior shoulder instability stabilized with the Latarjet-Patte procedure. They found no recurrence of either dislocations or subluxations in their study, and only 1 patient did not return to playing rugby because of his shoulder. 18 However, in this study, athletes with a first-time dislocation were excluded.
In our study, we found a statistically significant increase in the recurrence rate in collision athletes (14.7%) compared with contact athletes (0%). Moreover, all the recurrences occurred as a result of high-impact trauma with another player or with the ground during competition. As proposed by Rice, 23 the rationale behind these results seems to be that in collision sports, athletes purposely hit or collide with each other or with inanimate objects repeatedly during a match or training with great force. While hits are also possible in contact sports, these usually occur with less force and frequency than in collision sports. 23 Although there is a lack of research directly comparing collision and contact sports, previous authors have published outcomes in collision versus noncollision athletes. Yamamoto et al 27 reported 49 athletes (22 contact vs 27 noncontact) who underwent arthroscopic stabilization with suture anchors and had a 14% redislocation rate in the contact group versus 4% in the noncontact group. Cho et al 3 reported a higher recurrent instability rate in the collision group, with a 28.6% postoperative recurrence rate compared with 6.7% in the noncollision group. Recurrences in contact athletes are more similar to those in noncollision sports than in collision sports. It is important for athletes to be informed accurately on this point before surgery.
A second relevant finding was that the collision athletes in the current series reported a 70.6% rate of return to sports at or near preinjury levels, which was significantly lower compared with 86.4% of contact athletes. This relatively large proportion of athletes in the collision group who did not return to preinjury levels may reflect the fact that these patients are exposed to high-demand activities where the glenohumeral joint requires the maximum of its capacity. Moreover, most collision sports such as American football and rugby involve a permanent impact to the joint, which could also compromise the results. Instead, in contact sports such as soccer and field hockey, which were the ones included in this study, shoulder demands are not so considerable. Previous authors have reported similar results regarding return to sports in collision athletes. Petrera et al 20 reported a 73% rate of complete return to preinjury levels in 22 collision athletes evaluated in their series. Cho et al 3 reported a 21.4% rate of complete return to preinjury levels in collision athletes, with only 57% of them returning to the same level with a slight or moderate limitation.
The third interesting finding of this study is that patients in the contact group returned to sports significantly faster than those in the collision group. Stein et al 26 prospectively evaluated shoulder sport–specific impairments after arthroscopic Bankart repair in 47 athletes. Patients were analyzed separately according to the shoulder sport: noncollision/nonoverhead (G1), collision (G2), overhead (G3), and martial arts (G4). Data were assessed at 4 points of treatment: preoperatively and postoperatively after 6, 16, and 32 months. These authors revealed that the progression of sports ability depended on the shoulder-dependent sport performed. Those athletes who participated in sports that needed more precision, load transfer, and endurance recovered significantly slower than those in the less shoulder function–dependent groups. Moreover, similar to our study, athletes who participated in shoulder function–demanding sports documented significantly inferior proficiency levels compared with those involved in less demanding activities. Other authors have also reported significant limitations of reattained shoulder proficiency levels based on intensive sports exposure. 4,9,16
Limitations
Some limitations of the current study should be mentioned: first, its retrospective nature, relatively small study population (43 athletes), and relatively short minimum follow-up (36 months). With more patients and an increased periods of follow-up, the overall redislocation rate may increase in both groups. Another limitation of our study is that the only collision sport analyzed was rugby, and the only contact sports analyzed were soccer and field hockey. These are the most popular sports in our country; however, other sports that are more common elsewhere were not included. Finally, almost all the patients included were male.
However, an important strength of our study is that outcomes of arthroscopic stabilization were compared between homogeneous groups of high-demand athletes after a first-time traumatic dislocation. In addition, the follow-up period and the main demographic and clinical characteristics of the 2 groups were similar, which provided an accurate comparison.
Conclusion
Arthroscopic stabilization for anterior instability of the shoulder is a reliable procedure with respect to shoulder function, range of motion, and postoperative return to sports in contact and collision athletes. Compared with the contact group (0%), the collision group yielded a higher recurrence rate (14.7%). Moreover, patients in the contact group returned significantly faster (5.2 vs 6.9 months, respectively) and more returned to preinjury or near-preinjury activity levels (86.4% vs 70.6% of patients, respectively) than patients in the collision group.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Hospital Italiano de Buenos Aires (protocol No. 3055).