
Abstract
Background:
Treatment of advanced osteochondritis dissecans (OCD) of the capitellum is controversial, especially in moderate-sized lesions.
Purpose:
To establish a treatment algorithm for capitellum OCD, we tried to determine the utility of and problems associated with anconeus muscle-pedicle bone graft with periosteal coverage (ABGP) for the treatment of moderate-sized articular OCD defects of the capitellum.
Study Design:
Case series; Level of evidence, 4.
Methods:
According to our protocol for elbow OCD, 16 patients (15 males, 1 female; age range, 12-17 years; mean age, 14.4 years) with a moderate-sized OCD lesion of the humeral capitellum were treated with ABGP. All patients had a full-thickness, unstable OCD lesion that was 10 to 15 mm in diameter. Clinical results and postoperative images, including radiographs and magnetic resonance imaging (MRI), were evaluated at a mean follow-up of 31 months (range, 24-66 months).
Results:
All but 1 patient had functional improvement after the procedure and returned to previous sporting activities within 6 months. One female patient needed 1 year for functional recovery due to development of postoperative chronic regional pain syndrome (CRPS). Two patients required additional surgery, including shaving of the protruding cartilage, and they returned to their previous level of activity. Mean arc of range of flexion-extension motion was 117° preoperatively and 129° at follow-up (P = .031). Mean elbow function as assessed with the clinical rating system of Timmerman and Andrews was 136 preoperatively and 186 at follow-up (P = .00012). Bony union of the graft as demonstrated by trabecular bone bridging on radiography was obtained within 3 months in all patients. Postoperative MRI was examined for 14 patients at 6 to 12 months after the procedure; the MRIs showed near-normal articular surface integrity in 9 of the 14 patients (64%) and underlying bony structure in 10 of the 14 patients (71%).
Conclusion:
Improvement after ABGP was obtained within 6 months in all except 1 patient, who developed CRPS. Postoperative radiography and MRI revealed near-normal articular surface integrity or underlying bony structure. This procedure is useful as a surgical option for a moderate-sized articular OCD lesion in the elbow.
Osteochondritis dissecans (OCD) of the humeral capitellum is a common sports-related disorder in young athletes such as baseball players and gymnasts. In cases of progressive OCD, the damaged articular cartilage detaches from the capitellum, forming a loose body that sometimes causes painful locking. The full-thickness articular cartilage defect causes radiocapitellar incongruity, resulting in irreversible osteoarthritic changes. A principle of treatment for OCD is prevention of this pathological progression. Treatment for early-stage OCD is conservative, although such treatment is not always successful. When the lesion progresses to full-thickness articular cartilage damage, arthroscopic debridement has been widely applied, with good results. 2,5,6,12,19,22 However, studies have shown that a large articular defect of the capitellum is a risk factor for subsequent degenerative changes. 22,24,27,28 Takahara et al 28 recommended repair or reconstruction for lesions exceeding either 50% of the capitellar width or 10 mm in diameter.
Results of reconstruction by multiple cylindrical osteochondral plug grafts for capitellar OCD using a nonweightbearing site from the knee (ie, mosaicplasty) have been encouraging. Several clinical studies have reported good outcomes for this procedure in severely damaged elbows. 1,8,9,26,31 However, unavoidable donor-site problems remain a key disadvantage of this technique. One report showed no adverse effects at the donor site, 10 but another reported donor-site problems after mosaicplasty. 20 Costal osteochondral autograft is another option, and some investigators have reported favorable outcomes. 16,18,23,25 Oka and Ikeda 18 used costal osteochondral autograft for a very large lesion. Shimada et al 25 applied this method for lesions exceeding 15 mm in diameter and reported good results in 26 cases, although rib harvesting has the potential to cause a pneumothorax.
Since 1998, we have used anconeus muscle-pedicle bone graft with periosteal coverage (ABGP) for reconstruction of capitellar articular defects between 10 and 15 mm in diameter. Grafts can be harvested from the ipsilateral elbow in the same operating field, so donor-site problems are minimal. The purpose of this operation is to reconstruct a stable, congruent articulation in moderate-sized capitellar OCD while causing minimal donor-site morbidity. This retrospective evaluation was performed to determine the efficacy of and problems associated with ABGP.
Methods
When we diagnose a patient with elbow OCD at our clinic, we evaluate radiography, computed tomography, and magnetic resonance imaging (MRI) results and choose a treatment option according to our protocol (Figure 1). In cases where the lesion is unstable and is diagnosed as International Cartilage Repair Society (ICRS) class III or IV OCD (Appendix Table A1), 4 arthroscopic debridement is performed. After removal of free bodies and complete debridement of the lesion, the diameter of articular defect is measured. For lesions smaller than 10 mm in diameter, the surgical procedure is concluded after debridement. For lesions larger than 15 mm in diameter, articular reconstruction procedures such as mosaicplasty or costal rib autograft are applied. For a moderate-sized lesion 10 to 15 mm in diameter, ABGP is performed. We started using this procedure in 1998.
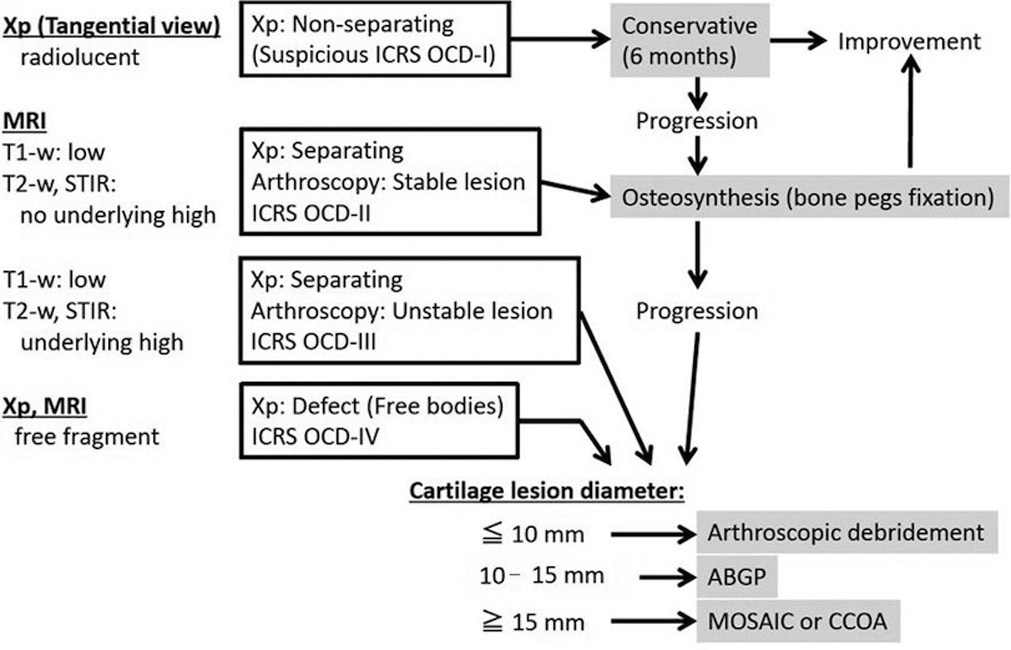
Treatment protocol for OCD of the capitellum. ABGP, anconeus muscle-pedicle bone graft with periosteal coverage; CCOA, cylindrical costal osteochondral autograft; ICRS, International Cartilage Repair Society; MOSAIC, mosaicplasty; MRI, magnetic resonance imaging; OCD, osteochondritis dissecans; STIR, short tau inversion recovery; Xp, radiography-proven.
In this study, 16 patients (15 males, 1 female; mean age, 14.4 years; range, 12-17 years) (Table 1) who underwent ABGP between 1998 and 2015 were observed for more than 24 months (mean follow-up, 31 months; range, 24-66 months). All patients agreed to the publication of clinical data, and approval was obtained from an institutional review board (No. 2016-35 from local committee) for this study.
Preoperative Status of Patients a
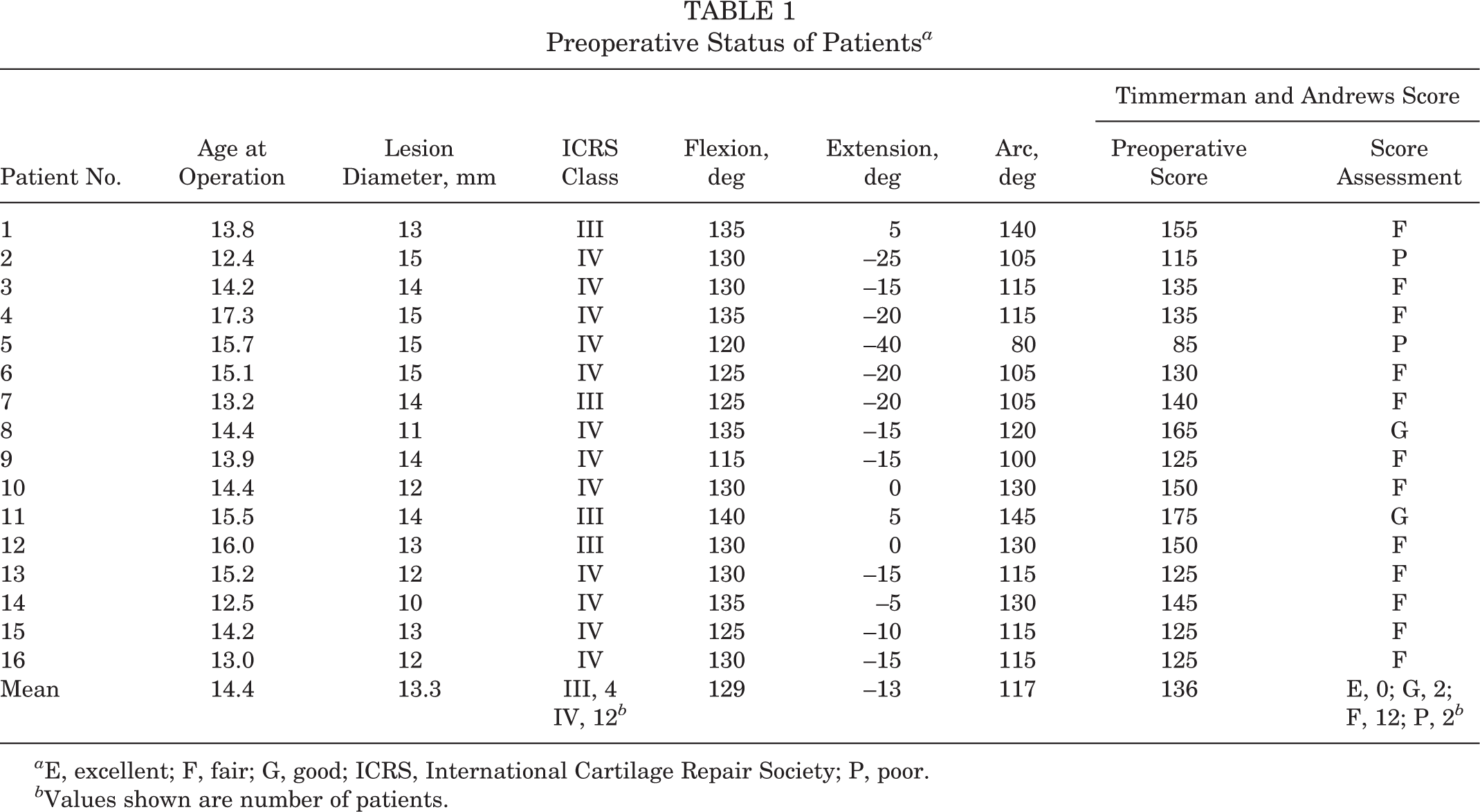
a E, excellent; F, fair; G, good; ICRS, International Cartilage Repair Society; P, poor.
b Values shown are number of patients.
Surgical Procedure
After arthroscopic debridement for progressive OCD and measurement of the lesion, an open posterolateral approach to the capitellum was performed with the patient’s elbow in full flexion. Through the anconeus muscle splitting approach, the articular defect of the capitellum is identified and anconeus muscle-pedicle rectangular bone is harvested from the posterior part of the lateral condyle with excess periosteum. The width of the harvested bone graft is the crater diameter divided by the square root of 2 (eg, graft width is approximately 9 mm for a lesion 13 mm in diameter) (Figure 2). The same width of anconeus muscle is elevated as a distal-based pedicle with approximately 1 cm of excess periosteum. The proximal end of the bone graft is covered with the excess periosteum fixed to the graft (Figure 3A). The longitudinal length of the graft is always about 20 mm, and the depth of the graft is comparable to the width. A rectangular bony defect is created on the posterior side of the lesion. A cylindrical bony tunnel is passed through the capitellum to the lesion by deepening the bony defect from both anterior and posterior directions. After debridement of the bony debris, anconeus muscle-pedicle bone is turned 90° anteriorly and pushed into the bony tunnel until the periosteum-covered bone graft reaches the surrounding articular surface (Figure 3B). The posterior bony defect is filled with artificial bone such as β-tricalcium phosphate (β-TCP) (eg, OSferion; Olympus Corp), which will be replaced by natural bone within a few months.

Graft width (W) is determined as the length of the measured diameter of the lesion (D) divided by the square root of 2 (W = D /√2; eg, 13 / √2 = 9 mm for a 13-mm lesion).
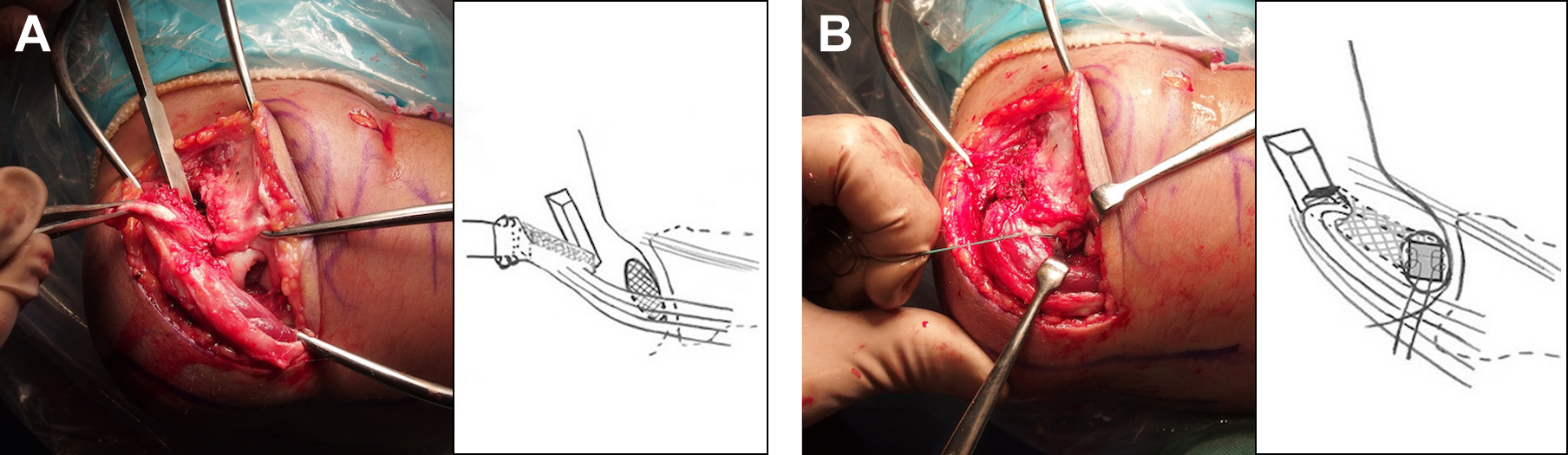
Surgical procedure for anconeus muscle-pedicle bone graft with periosteal coverage. (A) Graft elevation with excessive periosteum. (B) Pushing the graft into the bony tunnel to reach the surrounding articular surface. The posterior bony defect is buried with β-tricalcium phosphate.
Postoperative Rehabilitation and Guidance
After 2 weeks of immobilization, active range of motion exercises were started. The patient was not allowed to play sports for 3 months and was allowed to make a gradual return to sporting activities with some limitations once complete graft union (trabecular continuity on radiograph) had been achieved. We advise patients to try returning to their former activities without limitation 6 months after surgery. The patients attended postoperative follow-up is every 3 months during the first year after the operation and every 6 months during the second year in the outpatient clinic. Further follow-up was performed according to the patient’s desire.
Assessment
Clinical Assessment
We assessed all patients preoperatively and every 3 or 6 months after surgery as described above. Subjective evaluations (pain at rest and during sports or heavy activity, swelling, catching sensation, ability to perform daily and sporting activities) were obtained, and range of motion was measured with a goniometer (MMI-Jinnaka Goniometer; Muranaka). Elbow function was assessed according to the clinical rating system described by Timmerman and Andrews (Appendix Table A2). 29 Surgical complications were also evaluated.
The pre- versus postoperative status of the patients was compared with paired t test for continuous variables such as range of motion and with the Wilcoxon signed rank test for nonparametric values such as elbow function score. Statistical significance was determined at P < .05.
Radiography
Postoperative union of the graft and subchondral bone remodeling were assessed on radiographs every 3 to 6 months. Bridging or continuity of the trabeculae was defined as bony union. Images were taken from 3 directions: anteroposterior, lateral, and tangential in 45° of flexion to assess the anteroinferior area of the capitellum.
Magnetic Resonance Imaging
MRI (Magnetom Symphony 1.5 T; Siemens) was performed at 6 or 12 months postoperatively in 14 patients and was repeated in some patients. Conventional MRI sequences, including T1-weighted, T2-weighted, and short tau inversion recovery (STIR) imaging, were performed in the sagittal plane. Assessment was performed for changes in underlying bone in T1-weighted images and for articular congruity including cartilage signal in T2-weighted and STIR images. Results were assessed as normal or near-normal or as abnormal according to the criteria described by Roberts et al 21 (Appendix Table A3).
Revision Surgery
Additional surgery was performed in 2 patients (arthroscopy at 16 months postoperatively in patient 1, and mini-arthrotomy at 21 months postoperatively in patient 13) because of minor symptoms. We assessed the reconstructed articular surface and shaved rough or protruding, irregular articular surfaces.
Results
The postoperative status of the patients is shown in Table 2.
Postoperative Status of Patients a

a Values in parentheses were recorded after revision surgery. E, excellent; F, fair; G, good; MRI, magnetic resonance imaging; P, poor.
b 1, normal or near normal; 0, abnormal.
c Values shown are number of patients.
Clinical Findings
All patients noted elbow pain during sports activity before the operation, with some patients experiencing elbow pain even during daily activities. This pain limited daily or sports activities preoperatively but had resolved or was reduced at follow-up. All except 1 patient returned to previous daily activities without pain within 4 to 6 weeks postoperatively and achieved a successful return to previous sporting activities by 6 months postoperatively. The mean arc of motion for elbows was 117° preoperatively (129° of flexion, –13° of extension), improving to 129° postoperatively (133° of flexion, –3° of extension). Range of motion was statistically improved in both extension and arc from preoperatively to postoperatively, although no significant difference in flexion was evident (flexion, P = .227; extension, P = .011; arc, P = .031). Elbow function as assessed with the Timmerman and Andrews score was 136 preoperatively (good, n = 2; fair, n = 12; poor, n = 2), improving significantly to 186 postoperatively (excellent, n = 13; good, n = 1; fair, n = 2; P = .00012).
Regarding complications, other than the 2 patients with revision surgery, 1 female patient needed 1 year to return to playing tennis because of postoperative chronic regional pain syndrome (patient 14). No other complications were recognized in this series.
Radiography
All patients showed radiological bony union by 3 months. Some patients had small cysts or defects in the capitellum, which may have represented voids between the graft and recipient bone, but the size was very small and no adverse effects on clinical findings were evident. As a result, bony congruity of the radiocapitellar joint improved after surgery (Figure 4).

Radiographs of patient 4. (A) Preoperative, (B) postoperative, (C) 3 months postoperatively, and (D) 1 year postoperatively.
Findings on MRI
MRI was performed at 6 months postoperatively in 6 patients, at 12 months postoperatively in 8 patients, and at ≥24 months postoperatively in 9 patients. On MRI, good surface integrity was seen in 9 (64%) and near-normal underlying bone was seen in 10 (71%) of the 14 patients examined at 6 to 12 months postoperatively; these findings had improved at ≥24-month follow-up in the examined patients. Some areas of articular surface roughness were evident in 5 patients, and cartilage signal and its thickness observed on MRI were not normal in most cases; however, no clear separation of the fragment or defects of the surface were recognized (Figure 5).

Magnetic resonance images in the sagittal plane for patient 5 at 6 months postoperatively. (A) T1-weighted, (B) T2-weighted, and (C) short tau inversion recovery.
Findings at Revision Surgery
Additional surgery on the reconstructed lesion was performed for 2 patients, as mentioned above. One of these involved the first patient to undergo this procedure (patient 1) (Figure 6). The patient, a 13-year-old, had surgery for a moderate-sized OCD lesion (Figure 6A). The postoperative course was good both clinically and radiographically (Figure 6B). Although the patient had no symptoms, the MRI at follow-up showed roughness of the articular cartilage. We were concerned that the lesion would get worse and we decided to perform an arthroscopic revision. Mild articular roughness of the lesion was found and was shaved arthroscopically (Figure 6C). The patient quickly returned to his previous daily and sporting activity after arthroscopy.
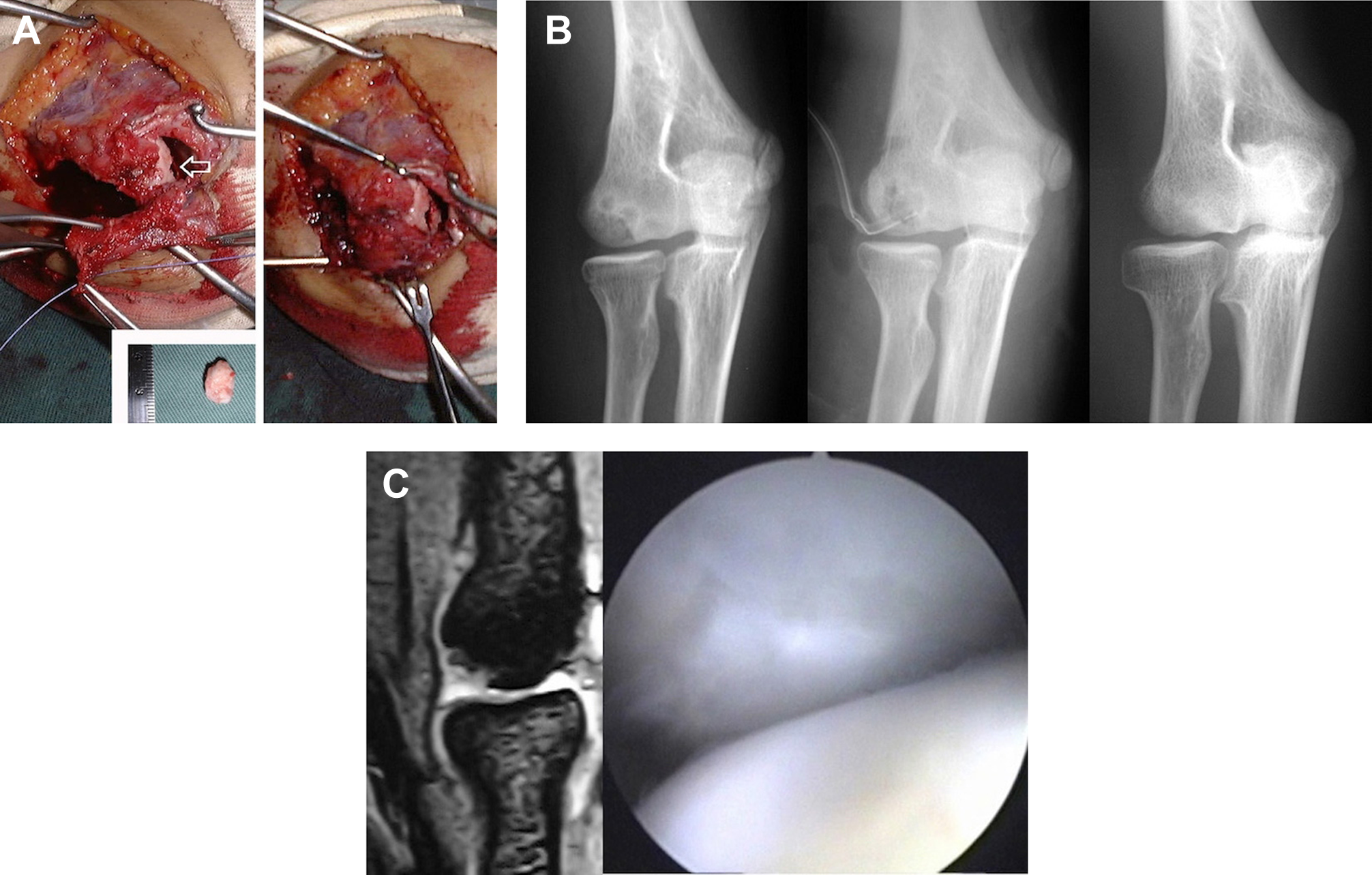
Operation, radiographs, magnetic resonance images (MRIs), and revision surgery (patient 1). (A) Left: A 13-mm free body was resected and pedicle bone was harvested. Right: The lesion was reconstructed using anconeus muscle-pedicle bone graft with periosteal coverage. (B) From left to right: radiographs taken preoperatively, shortly postoperatively, and at 4 years postoperatively. (C) MRI at 12 months postoperatively and revision surgery.
The second patient was an outfielder on a high school baseball team (patient 13). He experienced mild pain and catching 21 months postoperatively during high-level performance in baseball. His clinical assessment was fair, and the MRI showed mild irregularity of the reconstructed articular surface. A small cartilaginous flap and synovial plica were debrided during a mini-open procedure. He returned to his previous sporting activity quickly, and he successfully participated in a national high school baseball tournament 4 months after the second operation.
Discussion
Treatment for early-stage OCD should be conservative, but the symptoms are often mild and many patients continue to play sports, resulting in progression of the lesion. Advanced-stage OCD is difficult to treat, especially in young athletes who want to participate in high-level activity. OCD lesions include damage to both cartilage and subchondral bone, which requires substantial repair to allow the elbow to endure long-term sporting activity, especially when the lesion is large. Numerous treatment options are available for elbow OCD, such as open or arthroscopic debridement with or without microfracture or drilling, 2,5,6,12,19,22,24,27,28,30 closed-wedge osteotomy of the distal humerus, 13,32 and osteochondral autograft from the knee 1,8,9,26,31 or the rib. 16,18,23,25 However, consensus has been lacking regarding which treatment option is optimal. This is attributable to the poor outcomes seen in patients who have undergone resection/debridement arthroplasty, particularly for large lesions involving more than 50% of the capitellum. 27,28
Articular reconstructive procedures were developed in the late 1990s. Many reports have been published about multiple cylindrical osteochondral plug grafts (or mosaicplasty), and this technique has been used in other joints such as the ankle, elbow, and toes. 3,7,14,15 The first report of mosaicplasty for the treatment of elbow OCD in the English-language literature was by Nakagawa et al 15 in 2001, who reported mosaicplasty combined with intra-articular humeral osteotomy. The first case series of mosaicplasty for elbow OCD in the English-language literature was published in 2005, 26 and many other articles have followed. 1,8,9,31 Costal osteochondral autograft was introduced by Oka and Ikeda 18 in 2001. Costal osteochondral autograft represents another useful option to reconstruct large articular defects of the elbow, as indicated by some studies. 16,23,25 Those techniques can obtain good outcomes but carry unavoidable disadvantages such as the possibility of long-term progression of degenerative changes at the donor site. Small lesions can be treated by arthroscopic debridement and large lesions can be treated with osteochondral autografts, but what is a suitable threshold for differentiating large from small lesions?
The anconeus muscle-pedicle bone graft was originally described by Iwase 11 in 1987. This technique involves antegrade grafting of the anconeus-pedicle muscle to preserve blood supply to the bone that fills the OCD lesion. Periosteal coverage of the articular defect is also not a new idea. O’Driscoll 17 reported the utility of this method as offering hyaline-like neoplastic ability with continuous passive motion. We combined those 2 approaches for reconstruction of elbow articular defects. The muscle-pedicle graft offers vascularity that facilitates early bony union, while the periosteal coverage offers hyaline-like tissue regeneration that leads to good articulation. We first performed ABGP in 1998, on a patient initially diagnosed with a small ICRS class IV OCD lesion for whom arthroscopic debridement was planned. Intraoperatively, the OCD lesion was wider than had been anticipated and we had to change the procedure from simple debridement to reconstruction with minimal invasion. Results of MRI and second-look procedures showed reasonable, if not ideal, repair of the articular cartilage of the elbow. The first patient obtained a good result after a 4-year follow-up. Consequently, we routinely used this procedure in our treatment protocol for moderate-sized unstable capitellar OCD (see Figure 1).
The clinical and imaging results shown here were encouraging. Thus, in our clinic, when the lesion is stable and diagnosed in the early stage, conservative treatment is indicated (on suspicion of ICRS class I OCD). If the lesion has progressed and ICRS class II, III, or IV OCD is suspected, arthroscopic evaluation is indicated. In cases where the lesion is stable in ICRS class II, a repair procedure such as bone peg fixation is performed. In cases where the lesion is unstable and diagnosed as ICRS class III or IV OCD, arthroscopic debridement is performed. After removal of free bodies and complete debridement of the lesion, the diameter of the articular defect is measured. For a small lesion, the surgical procedure is concluded. For a large lesion, an articular reconstruction procedure such as mosaicplasty or costal osteochondral autograft is performed. For a moderate-sized lesion, 10 to 15 mm in diameter, ABGP is performed.
Although long-term follow-up is necessary, the approach described herein could represent a new surgical treatment option for articular reconstruction of severely damaged elbows with full-thickness, moderate-sized articular lesions such as OCD.
Conclusion
The surgical procedure of ABGP was reliable as treatment for an advanced and moderate-sized capitellum OCD lesion. A treatment algorithm for advanced capitellum OCD was based on the lesion size.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from JCHO Osaka Hospital Institutional Review Board (No. 2016-35).
Appendix
MRI Evaluation Criteria by Roberts et al 21

| Score | ||
|---|---|---|
| Feature | Normal or Near Normal | Abnormal |
| Surface integrity and contour | 1 | 0 |
| Cartilage signal in graft region | 1 | 0 |
| Cartilage thickness | 1 | 0 |
| Changes in underlying bone | 1 | 0 |
| Maximum total possible | 4 | |