
Abstract
Background:
Several risk factors for the postoperative recurrence of instability after arthroscopic Bankart repair have been reported, but there have been few detailed investigations of the specific risk factors in relation to the type of sport.
Purpose:
This study investigated the postoperative recurrence of instability after arthroscopic Bankart repair without additional reinforcement procedures in competitive athletes, including athletes with a large glenoid defect. The purpose of this study was to investigate risk factors related to the postoperative recurrence of instability in athletes.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 115 athletes (123 shoulders) were classified into 5 groups according to type of sport: rugby (41 shoulders), American football (32 shoulders), other collision sports (18 shoulders), contact sports (15 shoulders), and overhead sports (17 shoulders). First, the recurrence rate in each sporting category was investigated, with 113 shoulders followed up for a minimum of 2 years. Then, factors related to postoperative recurrence were investigated in relation to the type of sport.
Results:
Postoperative recurrence of instability was noted in 23 of 113 shoulders (20.4%). The recurrence rate was 33.3% in rugby, 17.2% in American football, 11.1% in other collision sports, 14.3% in contact sports, and 12.5% in overhead sports. The most frequent cause of recurrence was tackling, and recurrence occurred with tackling in 12 of 16 athletes playing rugby or American football. Reoperation was completed in 11 shoulders. By univariate analysis, significant risk factors for postoperative recurrence of instability included playing rugby, age between 10 and 19 years at surgery, preoperative glenoid defect, small bone fragment of bony Bankart lesion, and capsular tear. However, by multivariate analysis, the most significant factor was not the type of sport but younger age at operation and a preoperative glenoid defect with small or no bone fragment. Compared with the other sports, there was a significantly greater recurrence rate among rugby players without the aforementioned significant risk factors (small glenoid defect, ≤10%; medium or large bone fragment, >5%; and no capsular tear).
Conclusion:
Younger age at operation and preoperative glenoid defect with small or no bone fragment significantly influenced recurrent instability among competitive athletes.
Keywords
In treatment of traumatic anterior shoulder instability in competitive athletes, arthroscopic Bankart repair is usually recommended for overhead athletes to minimize adverse effects on the range of motion and muscle strength. Although some authors have reported good results with arthroscopic Bankart repair in collision/contact athletes without significant glenoid defects, other studies have shown high recurrence rates in this population. 7,9,12,13,21 This has led some authors to advocate for a return to open Bankart repair for collision/contact athletes. While there have been various reports about the clinical outcome of arthroscopic Bankart repair in athletes, 5,7,9,11 –13,21,24 few investigations have assessed the influence of the type of sport. Castagna et al 6 performed arthroscopic Bankart repair in young, highly active athletes and reported that recurrence was frequent among those playing water polo, rugby, basketball, and soccer, while Rhee et al 21 reported that among collision athletes who underwent surgical treatment (including open surgery), recurrence was frequent in wrestlers.
There have been many reports about the risk factors for postoperative recurrence of instability after arthroscopic Bankart repair, 2,20,25 among which Balg and Boileau 1 identified 6 significant risk factors and proposed the Instability Severity Index Score as a simple preoperative measure for predicting the clinical outcome. Their score assigns 2 points each for the categories of “patient younger than 20 years,” “involved in competitive sports,” “Hill-Sachs lesion visible in external rotation,” and “loss of glenoid contour” (on anteroposterior radiographs), while a score of 1 point each is given for “contact or forced overhead activity” and “anterior or inferior hyperlaxity”; thus, the maximum possible score is 10 points. These authors reported that patients with a score >6 points had an unacceptably high risk of 70% for recurrent instability. In relation to this scoring system, young competitive athletes with several kinds of bone defects on the humeral head and/or glenoid appeared to be a contraindication for arthroscopic Bankart repair.
The Instability Severity Index Score is a simple and useful tool for preoperative screening in the outpatient clinic with plain radiographs. However, small glenoid defects and small bone fragments can be easily missed on radiographs. After the investigation by Sugaya et al 22 of anterior glenoid rim morphology in shoulders with recurrent anterior instability, performed using 3-dimensional reconstruction of computed tomography (CT) scans, assessment of the glenoid defect has come to be considered an essential part of planning surgery for traumatic anterior shoulder instability. However, there have been few reports regarding the relationship between glenoid rim morphology and postoperative recurrence of shoulder instability after arthroscopic Bankart repair in athletes.
In the present study, we sought to investigate the effect of sporting category on the risk of recurrence after arthroscopic Bankart procedure. Specific risk factors for recurrence in relation to the sporting category were also investigated. We hypothesized that the postoperative recurrence rate of instability after arthroscopic Bankart repair would be higher in collision/contact athletes regardless of the type of sport as compared with other athletes and that risk factors for postoperative recurrence would be similar among collision/contact athletes.
Methods
Materials
This was a retrospective investigation of prospectively collected clinical data, and institutional review board approval was obtained. Between January 2010 and December 2013, we performed primary arthroscopic Bankart repair for traumatic anterior shoulder instability in 162 patients (173 shoulders). We limited our analysis to competitive athletes whose types of sport could be categorized. Therefore, 17 patients (17 shoulders) without sporting activity, 25 patients (28 shoulders) playing recreational sports, and 5 patients (5 shoulders) who played competitive sports that were difficult to categorize (motocross, 2; distance running, 1; gymnastics, 1; and snowboarding, 1) were excluded from this study. Subsequently, 115 competitive athletes (123 shoulders) were the focus of this study. Because of the high number of rugby and American football players in our study, we placed each in a category separate from the other collision sports. We therefore classified the athletes into 5 types of sports: group A (rugby), group B (American football), group C (other collision sports), group D (contact sports), group E (overhead sports). We also classified their level of competition as junior high school, high school, college, or semiprofessional. We had no professional athletes in our cohort. No doctors or physicians in our hospital were involved in any specific team as a team physician or medical staff.
Evaluation of Glenoid Rim Morphologies, Hill-Sachs Lesions, and Capsular Tears
The glenoid defect size, bone fragment size, and extent of bone fragment absorption were quantified with the methods shown in Figure 1.
16
Although Hill-Sachs lesion size and associated capsular tear, including humeral avulsion of the glenohumeral ligament (HAGL) lesions, could be preoperatively diagnosed on pain radiograph, CT, or MRI, intraoperative arthroscopic findings were adopted as a gold standard for diagnosis. Hill-Sachs lesions were assessed according to the arthroscopic criteria reported by Calandra et al
4
:
Negative (no bony lesion): grade 0 (no lesion) and grade 1 (defect of the articular surface not involving the subchondral bone)
Small bony lesion: grade 2 (small defect involving the subchondral bone, ≤1 cm)
Large bony lesion: grade 3 (large defect involving the subchondral bone, >1 cm)

Quantification method for the glenoid defect size, bone fragment size, and extent of bone fragment absorption. The inferior portion of the glenoid rim was approximated to a true circle on en face 3-dimensional computed tomography scans that were reconstructed with elimination of the head of the humerus. The size of the bone fragment size was measured on the image that gave the clearest view of the articular surface of the fragment. (A) The extent of the glenoid defect was calculated as a percentage of the glenoid rim length (b/a × 100%). (B) The size of the bone fragment was defined relative to the glenoid rim and was calculated as a percentage (c/a × 100%). The extent of bone fragment absorption was also calculated as a percentage: (1 – c/b) × 100%. a, the diameter of the fitted circle; b, the width of the glenoid defect; c, the width of the bone fragment.
Postoperative Recurrence Rate and Factors Related to Postoperative Recurrence
Postoperative recurrence was defined as any report of dislocation or subluxation. As 2-year follow-up data were available for 113 shoulders, the postoperative recurrence rate of instability was investigated separately for each sporting category. The recurrence rate was compared after stratification by the following factors via univariate analysis and multivariate analysis. Additionally, to clarify specific risk factors for each type of sport, the recurrence rates stratified by each factor were compared.
Factors analyzed were the type of event (primary/recurrent), sex, age at first instability and at operation (10-19 vs 20-29 years), interval between first instability and operation (<1, 1-2, or ≥2 years), total instability events (1-5, 6-10, or ≥11), preoperative glenoid defect size (0%, >0% to 10%, >10% to 20%, or >20%), preoperative bone fragment size (0%, >0% to 5%, >5% to 10%, or >10%) and extent of bone fragment absorption (0% to <50%, 50% to <100%, or 100%) in shoulders with bony Bankart lesions, Hill-Sachs lesion size (none, small, or large), and associated capsular tear including HAGL lesions (positive vs negative).
Statistical Analysis
Statistical analysis was performed with the statistical software EZR (Easy R), which is based on R and R commander and freely available on the website (http://www.jichi.ac.jp/saitama-sct/SaitamaHP.files/download.html; Saitama Medical Center, Jichi Medical University). 10 Univariate analysis was performed with the Fisher exact probability test, unpaired Student t test, and 1-factor analysis of variance as appropriate, with significance being accepted at P < .05. Multivariate analysis was performed with logistic regression analysis. Several possible risk factors shown by univariate analysis were selected as independent variables. Significant risk factors were selected after stepwise regression analysis of variables with the P value.
Surgical Technique and Postoperative Regimen
Arthroscopic Bankart repair was performed by the single-row suture anchor fixation technique. The anteroinferior glenohumeral ligament–labral complex was detached and mobilized from the glenoid neck to the 6-o’clock position. Because the aim of our Bankart repair is to avoid residual capsular redundancy by elevating the anteroinferior glenohumeral ligament–labral complex, capsuloligamentous tissue was separated up to 7 o’clock in the right shoulder if mobilization was inadequate or capsular laxity was severe. To accelerate union of the anterior labrum with the glenoid, the anterior 3 to 4 mm of the articular cartilage on the glenoid was debrided down to bone. Then, 4 to 7 suture anchors were placed at the anterior bone trough created in the glenoid. The 2.4-mm FASTak suture anchor (Arthrex) was used until June 2011, and the 1.4-mm JuggerKnot soft anchor (Biomet) was used after July 2011. Because of their smaller diameter and easier insertion, a larger number of anchors (4-6 FASTak suture anchors vs 5-7 JuggerKnot soft anchors) were inserted in each shoulder after introduction of the JuggerKnot soft anchor regardless of sporting category. For the treatment of bony Bankart lesions, arthroscopic bony Bankart repair was performed without resection of the fragment. 16 Even in shoulders with a large glenoid defect, bone grafting or rotator interval closure was not performed during the study period. There were no patients with isolated capsular tears or isolated HAGL. However, associated capsular lesions were repaired simultaneously with the arthroscopic Bankart procedure. Remplissage or bone grafting was not performed even for a large Hill-Sachs lesion.
Patients wore a brace (allowing 90° of internal rotation and 0° of abduction) for 4 weeks postoperatively and started passive range of motion exercises after 2 weeks. Until 4 weeks after surgery, flexion and external rotation with the arm at the side were restricted to 150° and 30°, respectively. After 4 weeks, full motion was permitted. For athletes involved in overhead sports, returning to sporting activity was permitted 6 months after surgery. However, for athletes involved in collision/contact sports, returning to contact training and competition was not permitted for at least 6 and 8 months after surgery, respectively.
Results
Patient Profile
Athletes were classified into 5 groups according to the type of sport:
Group A: rugby (41 shoulders)
Group B: American football (32 shoulders)
Group C: other collision sports (18 shoulders: martial arts, 14; wrestling, 2; ice hockey, 2)
Group D: contact sports (15 shoulders: basketball, 7; handball, 4; soccer, 2; water polo, 1; naginata [a sport similar to kendo], 1)
Group E: overhead sports (17 shoulders: baseball, 11; volleyball, 4; softball, 1; tennis, 1)
Athletes were attending junior high school (9 shoulders), high school (56 shoulders), and college (48 shoulders), and there were 10 semiprofessional athletes. The profile of these patients is shown in Table 1. There were significant differences in sex, age at first instability and at operation, and presence and size of preoperative glenoid defect and bone fragment among the 5 groups.
Patient Characteristics

a Values reflect No. (%) of shoulders unless otherwise indicated.
b Values in this column are results of a statistical analysis between the 5 groups.
c Statistically significant difference between any 2 groups: A vs C (P = .004), A vs E (P = .0014), B vs C (P = .0012), B vs E (P = .033).
d Statistically significant difference between groups A vs B (P < .05).
e See Figure 1 for calculation of percentages.
f Statistically significant difference between groups A vs E (P < .05).
g Statistically significant difference between groups A vs E (P = .0051) and C vs E (P = .0437).
h There was no significant difference between any 2 groups.
i Statistically significant difference between groups B vs C (P = .0134).
jP value for positive vs negative finding of Hill-Sachs lesion.
Postoperative Recurrence of Instability in Each Sporting Category
Among the 113 shoulders followed for a minimum 2 years, postoperative recurrence of instability was recognized in 23 shoulders (23 athletes; recurrence rate, 20.4%). Regarding the influence of sporting category, the recurrence rate was 33.3% (12 of 36) for rugby, 17.2% (5 of 29) for American football, 11.1% (2 of 18) for other collision sports, 14.3% (2 of 14) for contact sports, and 12.5% (2 of 16) for overhead sports. The recurrence rate was significantly higher in rugby than the other sports (P = .0202) and the other collision sports (P = .0475).
Of the 23 athletes who sustained a recurrence, 1 rugby player and 1 wrestler underwent reoperation at other hospitals, and we could not obtain detailed information regarding these patients. Of the remaining 21 patients, the mean interval between primary operation and recurrence was 13.2 months, and 16 players were reinjured while playing their previous sports. Patient details are shown in Table 2. Major trauma (sufficient to cause recurrence) occurred in 6 shoulders, but recurrence was noted after moderate trauma in 12 shoulders and after minor trauma in 3 shoulders. Recurrence occurred while tackling for 12 of 16 athletes playing rugby or American football. Reoperation was done at our hospital for 7 shoulders and at other hospitals for 2 shoulders. Among 12 athletes who did not undergo reoperation, 4 returned to their previous sports at the preinjury level, while 4 returned at a lower level and 4 retired (Table 3).
Patients With Postoperative Recurrence of Instability: Preoperative and Intraoperative Factors a

a HAGL, humeral avulsion of glenohumeral ligament.
b Total instability events.
Details of Postoperative Recurrence and Postrecurrence Among Patients a

a ASB, arthroscopic Bankart repair; B&B, open Bristow procedure combined with arthroscopic Bankart repair.
b Interval since primary operation.
Factors Related to the Postoperative Recurrence of Instability
Significant risk factors related to the postoperative recurrence of instability by univariate analysis were age between 10 and 19 years at operation and capsular tear (including a HAGL lesion) (Table 4). Regarding preoperative glenoid defect size and bone fragment size, while there were no significant differences among 4 groups, the recurrence rate was significantly different between 2 groups (preoperative glenoid defect size, 0% or >0%; preoperative bone fragment size, ≤5% or >5%) and among 3 groups (preoperative glenoid defect size, 0%, >0% to 10%, or >10%). So, preoperative glenoid defect and small-sized bone fragment of a bony Bankart lesion (≤5%) were also shown to be significant risk factors.
Factors Related to the Postoperative Recurrence in All Athletes

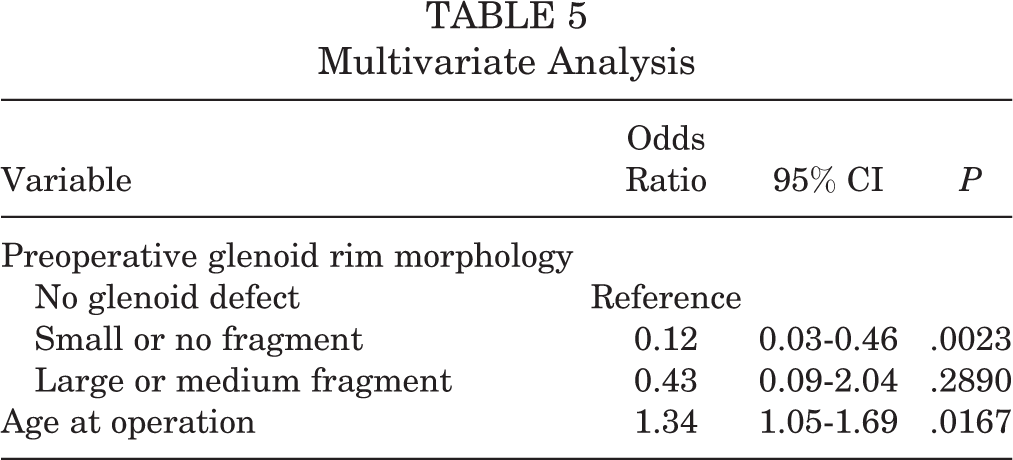
As the independent variables for multivariate analysis to analyze risk factors, type of sport (5 categories), preoperative glenoid rim morphology (3 categories), Hill-Sachs lesion (positive vs negative), and capsular tear (positive vs negative) were selected as the quality data, and age at operation, interval since first instability, total instability events, and preoperative glenoid defect size were selected as the quantity data. The preoperative glenoid rim morphology was classified into the following 3 categories according to the presence of glenoid defect and size of bone fragment of bony Bankart lesions: no glenoid defect, a glenoid defect with small or no bone fragment (≤5%), and a glenoid defect with medium or large bone fragment (>5%). By multivariate analysis, preoperative glenoid rim morphology and age at operation were shown to be the most significant risk factors (Table 5).
Multivariate Analysis
As the recurrence rate was much higher in rugby players and the risk factors for rugby appeared to be different from those for other sports, the recurrence rate was compared between rugby and the other sports regarding the factors that were shown to be significant risks for postoperative recurrence by univariate analysis (Table 6). Compared with the other athletes, rugby players had a higher recurrence rate associated with the following factors: small glenoid defect (≤10%), large bone fragment (>5%), and no capsular tear. Thus, while recurrence rate was high in rugby players and the other athletes with significant risk factors, it was still high solely in rugby players without significant risk factors.
Comparison of Recurrence Rate Between Rugby and Other Sports

Discussion
The present study investigated postoperative recurrence after arthroscopic Bankart repair without additional reinforcement procedures for young competitive athletes with traumatic anterior shoulder instability, including athletes with large glenoid defects. We found there was high postoperative rate of recurrent instability (almost 20%). While there have been many reports about the risk factors for postoperative recurrence of instability after arthroscopic Bankart repair, 2,20,25 the significant risk factors for athletes shown in the present study were age at operation and preoperative glenoid rim morphology.
Age at operation has been reported as a risk factor in several previous works, and the critical age for recurrence has been reported to be 20 years, so our result was compatible with previous reports. 2,25 However, as all of our subjects were young athletes (<30 years) and teenagers showed a significantly higher recurrence rate when compared with older athletes (>20 years), it was shown that 20 years could be applied as the critical age for recurrence even for competitive athletes.
Regarding the preoperative glenoid rim morphology, a preoperative glenoid defect of 20% to 25% was generally the critical size for arthroscopic repair. However, Sugaya et al 23 reported that arthroscopic repair of a bony Bankart lesion with suture anchors was successful even in shoulders with a chronic large glenoid defect, as most of the bone fragments were preserved. In contrast, Boileau et al 2 and Mologne et al 14 reported that the risk of postoperative recurrence was significantly increased in patients with a large glenoid defect when a bone fragment was not present. Nakagawa et al 15 reported that the bone fragment displayed a marked decrease in size relative to the glenoid defect within 1 year of the initial event, suggesting that most bone fragments underwent extensive absorption within 1 year after primary injury. In another study, Nakagawa et al 16 reported that the postoperative bone union rate was lower and union was delayed after arthroscopic bony Bankart repair when the residual bone fragment was small, while the postoperative recurrence rate was significantly higher. The size of the bone fragment can therefore be considered an important factor for successful bony Bankart repair.
As a higher recurrence rate was recognized in shoulders having a glenoid defect with a small or no bone fragment, arthroscopic Bankart repair without additional reinforcement procedures might be contraindicated for competitive athletes with such glenoid morphology.
Regarding the influence of the type of sport, in the present study the recurrence rate was significantly higher in rugby players (33.3%) than other athletes, even other collision athletes. However, based on the results of multivariate analysis, type of sport was not necessarily the significant risk factor. The higher recurrence rate in rugby players in our study might be due to their other risk factors. Among them, younger age at operation might have the most significant effect on recurrent instability, because almost 90% of rugby players in the present study were <20 years old and their ratio was significantly higher than that of the other athletes. Furthermore, Nakagawa et al 17 reported that the glenoid defect was significantly larger in size in male collision athletes (rugby players and American footballers) than in male baseball players, while the size of the glenoid defect was similar between male baseball players and female athletes. As rugby players in the present study also had a larger glenoid defect on average, this might have affected their higher instability recurrence rate.
When compared with athletes of the other sports, rugby players with the following characteristics demonstrated a significantly higher recurrence rate: smaller preoperative glenoid defect, larger bone fragment, and no capsular tear. These factors are different from the risk factors that we found for athletes overall (a younger age at operation, the presence of preoperative glenoid defect, a small bone fragment of bony Bankart lesion, and the presence of a capsular tear). There have been few previous reports regarding the difference in postoperative recurrence rate after arthroscopic Bankart repair between collision and contact athletes. Burkhart and De Beer 3 studied 101 collision athletes (96 rugby players and 5 American footballers) and reported that postoperative recurrence was recognized in 14 of 96 (14.6%) rugby players and 0 of 5 (0%) American footballers. While the number of American footballers was small and all shoulders with significant bone defects were recognized in rugby players, the recurrence rate was different between rugby and American football. In the present study, the most frequent cause for recurrence was tackling among athletes playing rugby (8 of 11) or American football (4 of 5). As tackling is one of the most dangerous maneuvers for shoulder dislocation, unskilled tackling techniques among younger athletes might explain their higher recurrence rate. However, while almost all rugby players are involved in tackling, fewer American football players are involved in tackling skill. This difference in tackling frequency may therefore account for the higher recurrence rate among rugby players.
Castagna et al 6 performed arthroscopic Bankart repair in young, highly active athletes and detailed the risk factors for recurrence of instability in relation to type of sport. They excluded shoulders with a large glenoid defect (≥25%) from their study; however, the other inclusion criteria were similar to ours, as were their recurrence rates (21% for all subjects and 33.3% for rugby players), and they reported that the recurrence rate was highest among patients playing water polo. They described rugby as a very high-energy contact sport and water polo as a high-energy contact sport associated with the overhead position of the arm. While “contact or forced overhead activity” is one of the risk factors in the Instability Severity Index Score proposed by Balg and Boileau, 1 we think that it is important to investigate and understand the characteristic features of each sport, without bundling various kinds of collision/contact sports, so that the indications for surgery can be determined according to a more precise evaluation of the risk of injury related to various sporting activities. To lower the recurrence rate, bone grafting procedures with or without arthroscopic Bankart repair are recommended for younger rugby players with preoperative glenoid defect and small or no bone fragment or with capsular tear. However, arthroscopic Bankart repair should not be easily abandoned for other athletes with a large bone fragment, even in shoulders with a large glenoid defect.
A limitation of the present study was its retrospective design, while preoperative CT data that had been collected prospectively were used to evaluate preoperative glenoid rim morphology. Another limitation is that the number of athletes was small in the sports other than rugby and American football, so it was not possible to investigate detailed differences among sports. Evaluation of the size of Hill-Sachs lesions was also a weakness of this study. While Hill-Sachs lesions were classified according to arthroscopic findings in the present study, a more precise and simple CT classification has been established recently. 18,19 Moreover, not only the size but also the location of Hill-Sachs lesion was recently reported to be important according to the concept of the glenoid track. 8,26 Although we understood the importance of precise investigation regarding the influence of Hill-Sachs lesions on postoperative recurrence after arthroscopic Bankart repair, detailed investigation based on the size and location of Hill-Sachs lesions by CT might have caused our study to become more complicated. However, Nakagawa et al 18 have reported that the size of the Hill-Sachs lesion does not influence postoperative recurrence of instability, as there were no significant differences among the 3 groups with regard to all parameters of Hill-Sachs lesion size (length, width, and depth). Accordingly, we simply evaluated bony Hill-Sachs lesions according to the arthroscopic findings. Finally, low statistical power was a major limitation because of the small number of subjects. We know well that power analysis is important, but as the number of postoperative recurrence was very small as an endpoint, statistical significance was set at P < .05. Hereafter, we would like to increase the number of subjects and further investigate the factors influencing postoperative recurrence.
Conclusion
Among competitive athletes undergoing arthroscopic Bankart repair for traumatic anterior shoulder instability, postoperative recurrence of instability was most frequently recognized in rugby players. While several characteristics appeared to be risk factors by univariate analysis (younger age at operation, the presence of preoperative glenoid defect, a small bone fragment of bony Bankart lesion, and the presence of a capsular tear), by multivariate analysis, type of sport was not shown to be a significant risk factor, but preoperative glenoid rim morphology (glenoid defect of any size with a fragment ≤5%) and age at operation (<20 years) appeared to be the significant factors. In rugby players, however, postoperative recurrence often occurred without the presence of such risk factors.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Yukioka Hospital Institutional Review Board.