
Abstract

In 2010, Vitale et al 11 demonstrated the rising rate of acromioplasties being performed in New York State, which increased from 5571 in 1996 to 19,743 in 2006. Despite the high rate of acromioplasties currently performed, the precise role of the acromion remains incompletely understood. With intimate attachment to the deltoid, the acromion provides a lever arm for strength in shoulder abduction. 8 However, numerous reports have implicated the acromion in the development of shoulder pain from impingement and rotator cuff tears. 1,2,5
Reginald Watson-Jones reported the first acromial excision in 1939 for the treatment of supraspinatus tendon lesions at a meeting of the British Orthopaedic Association. 1 In 1949, Armstrong 1 reported a series of 95 patients with supraspinatus syndrome thought to be the result of abnormal compression of the rotator cuff tendons and subacromial bursa between the humeral head and acromion. All patients underwent complete excision of the acromion to the acromioclavicular joint, with 84.2% (80/95) showing satisfactory results. 1 In 1962, Hammond 5 reported good-excellent outcomes in 85.7% (18/21) of patients after complete acromionectomy for the diagnosis of supraspinatus syndrome/tendinitis. In 1991, Bosley 2 described 34 shoulders treated with total acromionectomy for chronic impingement syndrome. At a minimum 2-year follow-up, 85.3% (29/34) of shoulders had good-excellent function in terms of pain, strength, range of motion (ROM), and patient satisfaction. 2
Despite initially promising results, complete/radical acromionectomy is subject to poor outcomes in some patients. In 1981, Neer and Marberry 9 reported a series of 30 consecutive patients who had poor results after complete acromionectomy. They identified 8 patients with serious wound complications, 27 with persistent pain, and all 30 exhibiting marked shoulder weakness with an inability to raise the arm above 90°. They advocated for partial excision of the anterior one-third of the acromion with release of the coracoacromial ligament to prevent impingement. 9 Jeon et al 6 reported on 10 patients requiring deltoid/acromion reconstruction after failed acromionectomy. All patients complained of disabling persistent symptoms, all exhibited deltoid muscle retraction with cosmetic deformities, and none of the patients could actively raise the arm above 90°. 6
We present the clinical history and outcomes of a 26-year-old man who underwent complete acromionectomy at the age of 16 years for pain secondary to an aneurysmal bone cyst (ABC). The findings demonstrate that the absence of the acromion may not significantly impair function, provided the deltoid is intact.
Case Report
At 16 years of age, an otherwise healthy male patient presented to an outside clinic with persistent pain in the right shoulder. Historical data of that time period were obtained from a complete review of the patient’s medical records, including office notes, imaging reports, operative report, and pathology report. Initial radiographs revealed a well-circumscribed, expansile, lytic lesion of the acromion consistent with an ABC, and surgical excision was elected. From the operative report of the outside surgeon, it was noted that the deltoid and trapezius were released from the acromion, complete acromionectomy was performed, and the deltoid and trapezius were directly repaired to one another. A pathological evaluation confirmed the diagnosis of an ABC.
At 6 months, the patient was seen in routine postoperative follow-up and was noted to have excellent strength in his deltoid, supraspinatus, infraspinatus, teres minor, and subscapularis muscles, with no perceivable deficit compared with the contralateral side. At 10-year follow-up, the patient underwent a formal examination to evaluate and document the function of this acromionectomy-treated shoulder. His unaffected contralateral side served as the control.
The patient was examined using standardized ROM assessments, including active and passive elevation and abduction as well as active internal and external rotation at 90° and 0° of abduction. Clinical evaluations of the scapular position both at rest and with overhead motion were performed (Figure 1). Functional outcomes were measured using the American Shoulder and Elbow Surgeons (ASES) score, Disabilities of the Arm, Shoulder and Hand (DASH) score, and Western Ontario Rotator Cuff Index (WORC). Strength testing, both isometric and isotonic, was performed using a work simulator (BTE). For isometric testing, torque was measured for internal and external rotation, forward elevation, and abduction from a position with the elbow at the side. The patient was asked to perform maximum effort for 3 seconds, with a 10-second break between each trial. The average of the 3 trials was reported, and the percentage deficit compared with the contralateral normal shoulder was calculated. For isotonic testing, torque was set at 50% of the maximum torque calculated during isometric testing. In isotonic testing, power was measured for internal and external rotation, forward elevation, and abduction from a position with the elbow at the side to 90°. Three trials were again averaged, and the percentage deficit compared with the contralateral normal shoulder was calculated.

Clinical photographs demonstrating a normal-appearing scapular position with the extremities (A) at rest and (B) with overhead activity.
Imaging was performed at most recent follow-up. Standard shoulder radiographs including anteroposterior, axillary, and scapular-Y views were obtained. Magnetic resonance imaging (MRI; 1.5 T) of the affected and unaffected sides was performed, including T1 and T2 sagittal, axial, and coronal views. MRI scans were evaluated for rotator cuff integrity and muscle volume. Dynamic ultrasound (US) was performed by an experienced musculoskeletal radiologist using an iU22 US machine (Philips). US compared the affected and unaffected shoulders for humeral head position, rotator cuff motion, and scapulohumeral posture/motion, as previously described. 3
Clinical Findings
The patient presented 10 years after his index procedure and requested a formal evaluation of his shoulder function. At 10-year follow-up, the patient had no subjective complaints of pain, weakness, fatigue, or instability in his acromionectomy-treated shoulder. The ASES score was 98.3 of 100, with the only limitation being mild difficulty lifting 10 lb above the shoulder. The DASH score was zero, demonstrating an ability to perform activities of daily living without difficulty or pain. The WORC score was 100%, showing no subjective deficits in physical symptoms, sports/recreation, work, lifestyle, or emotions. The patient reported no deficits in his work (surgical technician) and no deficits with his recreational activities, which included weight lifting (eg, military press), golf, hockey, and throwing a ball overhead (dominant arm).
A physical examination of the operative shoulder revealed no tenderness to palpation, no skin retraction or indentation, and no visible atrophy. An inspection of the scapula demonstrated no obvious asymmetries at rest or with active ROM (Figure 1). The active ROM assessment revealed 180° of forward elevation and 180° of abduction bilaterally. ROM of the affected right shoulder (dominant side) at 90° of abduction was 54° of internal rotation to 111° of external rotation, for a total arc of 165°. ROM of the unaffected left shoulder showed external rotation of 98° and internal rotation of 68°, for a total arc of 166°. External rotation of the affected right shoulder at 0° of abduction was 77° compared with 57° on the unaffected left side. Internal rotation on the affected side was T7 compared with T6 on the unaffected side.
Both isometric and isotonic strength testing was performed. For isometric testing, the affected right side was weaker than the left side for external rotation, internal rotation, and forward flexion by 12%, 5%, and 13%, respectively (Table 1). For isotonic testing, the affected right side was weaker than the left side for external rotation, internal rotation, forward flexion, and abduction by 24%, 16%, 3%, and 12%, respectively (Table 1).
Isometric and Isotonic Strength Testing: Affected vs Normal Shoulder a
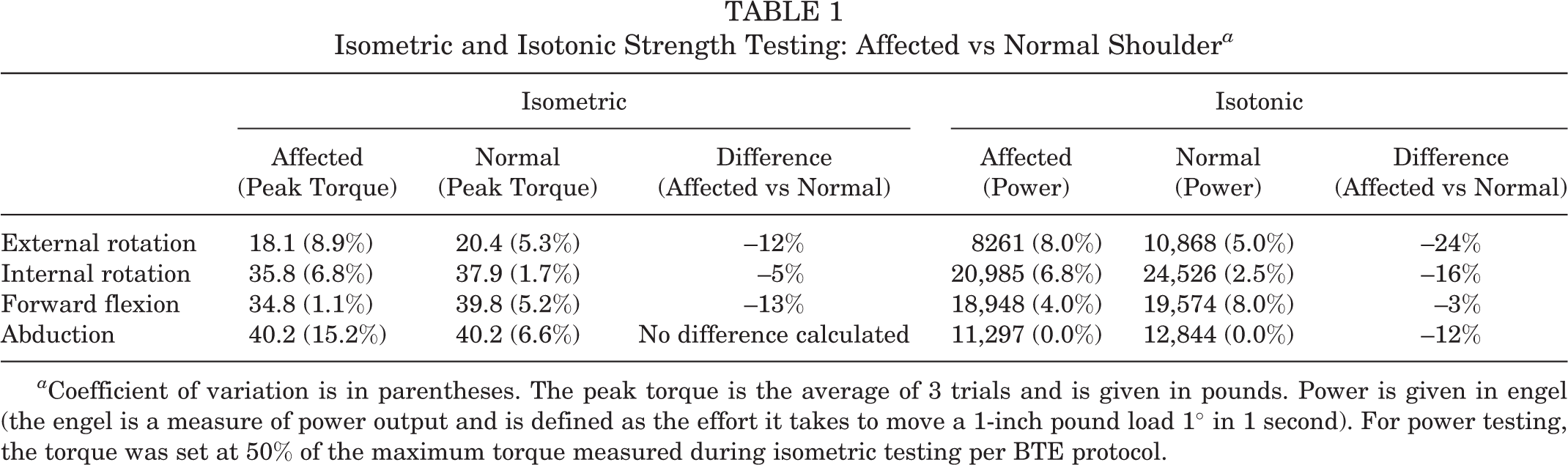
a Coefficient of variation is in parentheses. The peak torque is the average of 3 trials and is given in pounds. Power is given in engel (the engel is a measure of power output and is defined as the effort it takes to move a 1-inch pound load 1° in 1 second). For power testing, the torque was set at 50% of the maximum torque measured during isometric testing per BTE protocol.
Imaging Evaluation
Shoulder radiographs at most recent follow-up are shown in Figure 2. Anteroposterior, axillary, and scapular-Y radiographs showed complete acromionectomy to the base of the coracoid, with a well-centered humeral head and no evidence of humeral migration or glenohumeral osteoarthritic changes. When compared with the normal shoulder, MRI of the affected shoulder revealed normal-appearing rotator cuff tendons (Figure 3). On the affected right side, the infraspinatus showed slightly increased volume compared with the unaffected left side. Previous work has shown excellent intrarater reliability, consistently greater than 0.90, of static and dynamic US measurements of the shoulder when performed by an experienced radiological technician. 3 Dynamic US with abduction showed rotator cuff motion to be symmetric and appropriate. There was no elevation of the humeral head relative to the glenoid or coracoid on dynamic US. Only one asymmetry of the scapulohumeral posture was noted on US. Both dynamically and at rest, measurements of the humeral head–to–coracoid distance were obtained. The humeral head of the affected shoulder lay 3 mm posterior in relation to the coracoid in neutral position, external rotation, and abduction when compared with the unaffected shoulder. No other significant static or dynamic differences were found.
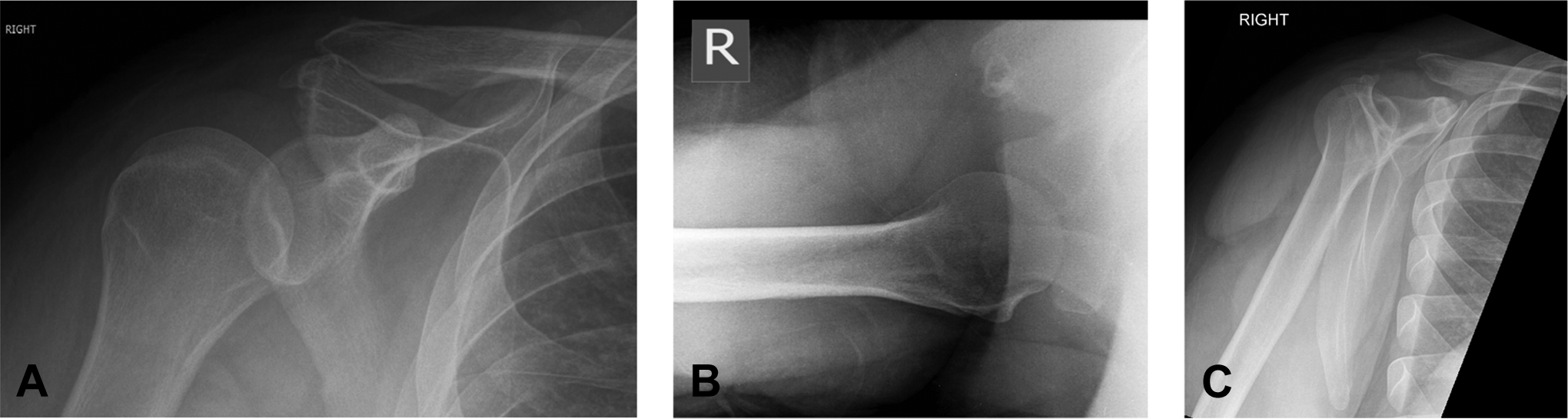
(A) Anteroposterior, (B) axillary, and (C) scapular-Y radiographs showing acromionectomy to the base of the coracoid, a well-centered humeral head, and no evidence of humeral migration or glenohumeral osteoarthritic changes.

Coronal, sagittal, and axial T1-weighted magnetic resonance imaging (MRI) of the (A, C, and E) affected right shoulder and (B, D, and F) unaffected left shoulder. MRI of the affected right shoulder revealed normal-appearing rotator cuff tendons compared with the unaffected left shoulder. On the affected right shoulder, there was an apparent tendinous connection between the trapezius and deltoid at the site of surgical repair. In addition, the infraspinatus showed slightly increased muscle volume compared with the unaffected left shoulder.
Discussion
The acromion provides an insertion for the trapezius posteriorly and the origin for the deltoid anteriorly. 7 The middle third of the deltoid muscle, the strongest portion, originates along the lateral acromial border. The medial acromial border provides an attachment to a portion of the trapezius, and a small central portion articulates with the clavicle to form the acromioclavicular joint. The coracoacromial ligament attaches to the tip of the acromion and along its anterolateral undersurface. 10
With such intimate attachments, one must consider the potential detrimental effects to structure and function with complete acromionectomy. Despite concerns, numerous authors have published successful outcomes with complete acromionectomy in the treatment of impingement and rotator cuff tears. 1,2,5
Others have noted significant persistent pain and loss of function after partial and complete acromionectomies. 6,9 Forsythe et al 4 focused on the deltoid, asserting that the loss of the acromion weakens the deltoid by separating the muscle from its origin and mechanical fulcrum. Subsequent retraction of the tendon and the formation of subdeltoid adhesions to the rotator cuff and humerus led to stiffness and pain. 4
Using modern clinical measures and imaging, we found excellent shoulder function in this 26-year-old man at 10 years after complete acromionectomy. ROM assessments demonstrated full active forward flexion/abduction without deficits in the total arc of rotation at 90° and with the arm at the side. Strength testing demonstrated modest deficits in external/internal rotation, forward flexion, and abduction in the affected shoulder. However, testing was performed with the elbow at the side and cannot be extrapolated to suggest normal strength and endurance with the arm in overhead positions. While this patient’s outcomes go against the anti-acromionectomy doctrine that Neer and Marberry 9 proposed, our study represents one patient with acceptable functional outcomes that can be achieved in certain situations. We do not recommend that complete acromionectomy be performed for the treatment of common shoulder impingement. Furthermore, our report highlights outcomes at midterm follow-up, and the long-term effect of complete acromionectomy remains to be determined. It is our opinion, as Bosley 2 pointed out, that if complete acromionectomy is necessary and the complication of deltoid retraction is avoided, acceptable shoulder function can be achieved.
We believe that the main reason that our patient had good clinical outcomes is his well-preserved deltoid function. The deltoid was sutured to the trapezius after the acromion was excised during the index procedure. Our patient’s strength of abduction in the affected shoulder was equal to the unaffected contralateral shoulder in isometric testing and approximately 12% weaker in isotonic testing. Perhaps it is not the acromion itself but the functional outcome of the deltoid that should be the focus. When acromion removal does result in deltoid dysfunction, shoulder dysfunction likely follows. In short, we believe that functional outcomes after acromionectomy hinge on deltoid function. In our patient, deltoid function after acromionectomy was preserved, and functional outcomes were excellent.
Conclusion
Despite the rising rate of acromioplasties being currently performed, 11 the precise role of the acromion remains incompletely understood. For years, complete acromionectomy was performed in the treatment of chronic supraspinatus syndrome and rotator cuff tears, with reported satisfactory outcomes. Despite early promising results, complete acromionectomy has been reported to result in poor outcomes by numerous authors. In this case report, 10 years after complete acromionectomy, a young adult patient with good deltoid function and deltoid reattachment to the trapezius demonstrated minimal functional deficits.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.